refferals to a renal clinical psychology service
advertisement

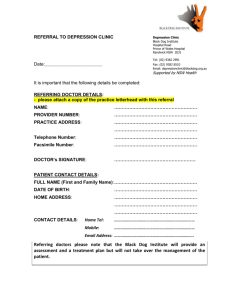
B39(W) REASONS FOR REFERRAL TO A RENAL CLINICAL PSYCHOLOGY SERVICE Coyne, E, Bebb, C Nottingham University Hospitals NHS Trust BACKGROUND: Significant levels of psychological distress have been identified in patients with CKD. NICE guideline (CG91) has specifically addressed the management of depression in patients with a chronic physical health problem, particularly recommending the use of medication and cognitive behavioural therapy 1. However, it has been argued that patients with CKD experience a wide range of psychological distress which may require a broader set of interventions2. There is a need to establish the type of difficulties for which renal patients are referred for psychological support. AIMS: (1) to identify the reasons for referral to a renal clinical psychology service (2) to ascertain the uptake of the service. DESIGN: A retrospective review was undertaken of all adult referrals to Renal Clinical Psychology from the Nottingham Renal and Transplant Unit during a 12 month time period from 1st August 2009 to 31st July 2010. Reason for referral was coded from the referral form/letter. RESULTS: Demographics: 98 Patients were referred to see a Clinical Psychologist. (45% Male, 55% Female). Mean age at referral 51 (range 18-88). All age groups were represented (18-25yrs: 9.18%, 26-35yrs: 12.24%, 36-45yrs: 15.31%, 46-55yrs: 24.49%, 56-65yrs: 12.24%, 66-75yrs: 17.35%, 76yrs +: 9.18%). The majority of referrals were dialysis patients (HD 62.24%, PD 13.27%, Pre-dialysis 15.31% and Transplant 9.18%). Referrals were made from all members of the multidisciplinary team although predominantly from the medical and nursing staff: Doctor 48.98%, Nurse 44.90%. Reasons for referral: Patients often presented with more than one problem, however only the primary reason for referral was coded: Reason for referral Adjustment (Coping with illness, dialysis, transplant or end of life care) Low mood Difficult decision making Concordance (fluid, diet, medication, clinic or treatment attendance) Trauma following medical/surgical procedure Anxiety/ Panic Fear/Phobia of medical or surgical procedure Other (e.g. bereavement, confusion) Denial of illness Weight Management (lose or gain weight) Percentage 30.61 19.39 9.18 8.16 7.14 6.12 6.12 5.10 4.08 4.08 Patient attendance: 88.78% attended an assessment appointment (6.12% DNA) (2.04% referred elsewhere prior to appointment) (3.06% Patients health circumstances changed). CONCLUSION/IMPLICATIONS: Renal patients are referred for a wide range of psychological issues which include depression. However, referral reasons are broader than depression and reflect the complexity of issues which occur within the renal care pathway. This data supports the view that provision needs to consider the range of psychological distress and not focus only on treatments for depression2. It also provides support for embedded psychological support within a multidisciplinary renal service rather than referral to a separate service for depression. 1 www.nice.org.uk/CG91 Attfield, R., Moran, J. & Mooney, A. (2010). The NICE guidance on depression in chronic illness. British Journal of Renal Medicine, 15 (3), 6-8. 2