Household characteristics associated with handwashing with
advertisement

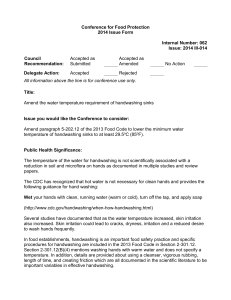
LRH: LUBY AND OTHERS RRH: HANDWASHING WITH SOAP IN RURAL BANGLADESH Household Characteristics Associated with Handwashing with Soap in Rural Bangladesh Stephen P. Luby, Amal K. Halder, Carole Tronchet, Shamima Akhter, Abbas Bhuiya, and Richard Johnston International Centre for Diarrhoeal Disease Research, Bangladesh, Dhaka, Bangladesh Centers for Disease Control and Prevention, Atlanta, Georgia Water and Environmental Sanitation Section, UNICEF Bangladesh, Dhaka, Bangladesh ABSTRACT Handwashing with soap prevents diarrhea and respiratory disease, but it is rarely practiced in high need settings. Among 100 randomly selected villages in rural Bangladesh, field workers enrolled 10 households per village and observed and recorded household activities for five hours. Field workers observed 761 handwashing opportunities among household members in 527 households who had just defecated or who cleaned a child’s anus who had defecated. In the final multivariate analysis, having water available at the place to wash hands after toileting (odds ratio = 2.2, 95% confidence interval 1.3, 4.0) and having soap available at the place to wash hands after toileting (odds ratio = 2.1, 95% confidence interval 1.3, 3.4) were associated with washing both hands with soap after fecal contact. Interventions that improve the presence of water and soap at the designated place to wash hands would be expected to improve handwashing behavior and health. 2 INTRODUCTION An estimated 1.9 million children under the age of 5 years die annually from diarrheal disease1 and an additional 2 million die from pneumonia.2 Small scale studies (fewer than 4,000 households) in settings where diarrhea and respiratory disease are leading causes of death demonstrate that households that receive intensive handwashing promotion report less diarrhea3, 4, 5, 6 and respiratory disease7 compared to control households. However, in settings where diarrhea is an important cause of child mortality, the prevalence of handwashing with soap after contact with feces as assessed by structured observation is typically <30%.8, 9, 10, 11 In 2007 the Government of Bangladesh, Department of Public Health Engineering in collaboration with UNICEF and with support from the Department for International Development (DFID) of the British Government launched a program, SHEWA-B (Sanitation, Hygiene Education and Water supply-Bangladesh) that is among the largest intensive handwashing, hygiene/sanitation and water quality improvement programs ever attempted in a low income country. In the first stage the intervention is targeting 19.6 million people in rural Bangladesh. A primary objective of the intervention is to increase the proportion of persons who wash their hands at key times, that is before preparing food, before eating, before feeding a child, after defecating and after cleaning a child’s anus. Earlier work from urban Dhaka, Bangladesh noted that children living in households that field workers confirmed had water at the most convenient place to wash hands, had 5% less respiratory symptoms compared to households without water available at the place to wash 3 hands after correcting for differences in socioeconomic status.12 We analyzed data collected from 100 villages for the baseline assessment before initiation of the SHEWA-B program. The objective of this analysis was to explore characteristics associated with handwashing, and specifically to explore if elements of handwashing infrastructure, that is having a designated place to wash hands, and having water and soap present at the place, was associated with handwashing with soap independent of socioeconomic status. METHODS Study population. During the first two years the SHEWA-B program targeted 68 sub districts (upazilas) with a population of 19.6 million people (Figure 1). The government and UNICEF selected the specific sub-districts because of the perceived need in these communities and the absence of other active programs addressing water, sanitation and hygiene in these sub-districts. Upazilas are further subdivided into unions. We listed all of the unions in the 68 targeted sub-districts and randomly selected 50 unions with the probability of selection proportional to the size of the union. The only exception to strict proportionality by population was an intentional oversample of the subdistricts in the Chittagong Hill Tracts. These sub-districts are among the most impoverished in the country, and because an important objective of the program is to reach the poorest groups, 10% of the evaluation sample was reserved for Chittagong Hill Tract communities to assure sufficient observations to permit separate analysis. 4 Within each selected union we listed all village names, and using a random number generator selected the evaluation village. UNICEF and the Department of Public Health Engineering selected one non-intervention control sub-district that had no major hygiene promotion intervention, but had similar infrastructure, agricultural productivity, household construction and hydrogeology for each randomly selected intervention sub-district. Unions and villages within the control sub-districts were enrolled as controls using the same methods used for enrolling intervention villages. Field workers asked residents of the selected village to identify the village center. Field workers identified the household closest to the village center that had a child <5 years of age and sought consent for participation in the evaluation. As part of the consent process, field workers explained that the objective of the evaluation was to understand water, sanitation, and hand hygiene practices. To enroll the next household, fieldworkers skipped the next two closest households, and then looked for the next household with a child <5 years of age. Field workers repeated the process for enrolling additional households until 10 households in each selected village were enrolled. Since intervention activities had not been initiated and we were interested in associations between characteristics and handwashing behavior throughout rural Bangladesh we included both the intervention and control households in this analysis. Data collection. Structured observation. Trained field workers conducted 5-hour structured observations of handwashing behavior of all persons in selected households between 9:00 AM and 2:00 PM, a culturally acceptable hour for 5 visitors and the typical time for a range of personal hygiene and food preparation behaviors. Using a pre-tested instrument field workers noted handwashing behavior at key times -- before preparing food, before eating or feeding a child, after defecating and after cleaning a child’s anus who had defecated. Cross sectional survey. Two months after the structured observation field workers returned to the households and administered a pre-tested cross sectional survey and spot check. Questions included on the cross sectional survey included demographic information as well as household construction and possessions to permit a measurement of acquired household wealth. Field workers asked respondents to, “Show me where you usually wash your hands after you use the toilet.” The field worker coded whether this was inside or near the toilet facility, inside or near the kitchen, elsewhere in the yard, outside the yard, or no specific place. The field worker also observed whether there was water available and whether there was soap available at the identified location. We classified latrines as improved according to the WHO definitions, that is a pit latrine with a slab, a ventilated improved pit latrine, a composting toilet or a flush toilet connecting to a piped sewer system, septic tank or pit latrine.13 Outcomes. We linked data from the household structured observation with the household cross sectional survey. The primary outcome variable was whether or not a person under observation in the 6 household who had defecated or had cleaned the anus of a child who had defecated, subsequently washed both hands with soap. The objective for handwashing within rural Bangladesh culture differs from the germ theory conceptualization used by public health practitioners 14. After defecation most adults in rural Bangladesh clean their anus by using water and their left hand. The left hand is most commonly subsequently rinsed with water. Because of its impurity, the left hand should not touch the right.14 We focused on handwashing after fecal contact because this is a situation where handwashing with soap would be expected to interrupt gastrointestinal pathogen transmission. We focused on handwashing with soap because of the strength of evidence that this improves health. We evaluated washing both hands because earlier studies noted that both the right and left hands were contaminated with fecal coliforms.15 Data analysis. We calculated odds ratios to evaluate the association between individual and household characteristics with washing both hands with soap. To account for the repeated observations in single households and the clustering of observations in villages we used general estimated equations to calculate these odds ratios and 95% confidence intervals.16 To construct a multivariate model we began with the characteristic that had the greatest effect on the goodness of fit of the general estimated equation model. We sequentially tested additional variables that were associated with handwashing in the bivariate analysis with a p-value < 0.10 into the multivariate model. For the final multivariate model we retained all variables that were significantly associated with handwashing with soap (p<0.05) and significantly improved fit (p<0.05). We used a nested correlation structure for all general estimated equations analyses to account for the clustering of observations within households, and the clustering of measures 7 within the same villages. We tested for interaction by combining characteristics of hypothesized interactions and evaluating if they made an independent contribution to the model. We used SAS for Windows, Version 9.1 (SAS Institute, Cary, NC, USA) for the general estimated equations modeling. We used principal component analysis to evaluate household wealth.17 We excluded hygiene and sanitary infrastructure from the wealth index, because we wanted to analyze the impact of wealth independent of the specific facilities and supplies that might contribute to handwashing. We analyzed variables in the wealth index by means, frequencies and standard deviations and calculated score coefficients. We used the correlation matrix of the 24 variables to calculate sample weights.18 The coefficients were calculated by rounding the expression (Loading/standard deviation) x 100 to the nearest integer. We used the first principal component as the wealth score.19 Ethics. All households provided informed consent. Because this was an evaluation of a public health program rather than a primary research project, the program evaluation was not reviewed by a human subjects research panel. RESULTS The field team completed structured observations of 1000 households. In 529 households (53%), field workers observed a household member who had just defecated or who cleaned a child’s 8 anus who had defecated. Two to four months later field workers interviewed the mother of the youngest child in 527 of these households (99%) with the cross sectional survey. This analysis is based on the handwashing behavior following the 761 episodes of fecal contact observed in these 527 households. Approximately one third of mothers and fathers within the observation group did not have any formal education. Only 15% of fathers and 8% of mothers completed secondary school. Most used a tubewell for drinking water and owned a latrine (Table 1). The most common type of latrine (56%) was a pit latrine with a slab, but without a lid or water seal. Respondents in 95% of households identified a place to wash hands after toileting, though only 38% of these were inside or near the toilet. Field workers observed water present at 72% of the designated handwashing locations and soap at 52% (Table 1). In the wealth analysis, the first principle component retained 29% of the total data variability. The first principle component was highly correlated with 16 variables. The majority of fecal contacts were observed among females (79%) and among adult caregivers (58%) (Table 2). After contact with feces 134 persons (18%) washed both hands with soap. Adults and females were significantly more likely to wash both hands with soap following fecal contact than children and males in bivariate analysis. Household characteristics that were significantly associated with washing both hands with soap after fecal contact on bivariate analysis included 9 the mother of the youngest child having education above the primary level; wealth in the top two quintiles, and having soap, water, or water plus soap available at the place of handwashing after toileting (Table 3). The presence of water at the place to wash hands doubled the probability of washing both hands with soap. Similarly the presence of soap at the place to wash hands doubled the probability of washing both hands with soap. The location where household members specified that they usually washed their hands after toileting was not significantly associated with handwashing with soap after fecal contact. In the multivariate analysis, the characteristics that were independently significantly associated with handwashing were being an adult caregiver, mother’s education above primary level, having water available at the place to wash hands after toileting and having soap available at the place to wash hands after toileting (Table 4). The odds ratios in the multivariate analysis were little changed from the bivariate analysis. We tested the possible contribution of a place to wash hands after toileting that included both water and soap by adding this as a combined variable to the model in Table 4 that coded the presence of water and the presence of soap separately. The combined variable, neither improved fit nor was it significantly associated with observed handwashing with soap. We also constructed a model with the combined water plus soap at the place to wash hands, being an adult caregiver and mother’s education level. The model in Table 4 that included the presence of water separately from the presence of soap fit the data significantly better (p=0.01) than the model with only the combined variables. DISCUSSION 10 Rural Bangladeshi residents living in households with either water or soap at the place they usually wash their hands were twice as likely to wash both hands with soap after contact with feces than those whose handwashing location lacked soap or water. These findings are consistent with studies of handwashing in hospitals that concluded that hand hygiene was improved when equipment and supplies were present that made it easier to wash hands.20, 21, 22 It is possible that having a designated place to wash hands that included soap and water was purely an external manifestation of household residents’ intent to wash hands, and so was only a marker of handwashing intent, and not an independent facilitator. But this extreme interpretation ignores the broad scholarship on ecological models of behavior change which stress the contribution of an appropriate environment to facilitate healthy behavior.23 The relationship of handwashing infrastructure and supplies with improved handwashing behavior suggests that encouraging households to equip a place to wash hands with water and soap would be expected to increase the rate of handwashing. Ninety-five percent of households identified a place to wash hands after toileting. The proximity of the handwashing location to the toilet did not predict handwashing behavior. Thus, environmental interventions are most likely to change handwashing behavior if they focus on adding water and/or soap to the household’s designated handwashing site. Measuring handwashing behavior has proved difficult. Careful studies have repeatedly confirmed that reported handwashing behavior is not a valid measure of observed behavior.9, 24, 25, 26 Structured observation is time consuming, expensive, and risks altering behavior in the presence of an observer. Microbiological measures of hand contamination are expensive and 11 only weakly associated with health outcomes.27, 28, 29 Earlier work suggested that the presence of a place to wash hands with water in urban Bangladesh was associated with a slight decrease in respiratory disease symptoms.12 The findings from the presented analysis are new evidence that a spot check to identify a convenient place to wash hands that has soap and water present, is a rapid, inexpensive, objective proxy measure associated with handwashing. If studies in other settings confirm the associations between a place for handwashing that has soap and water, and handwashing behavior and handwashing associated diseases, then this may become a useful indicator for assessing progress in handwashing promotion efforts in high need communities globally. An important limitation to this evaluation is that the handwashing behavior that was observed during the structured observation session may not be typical behavior of the household’s residents after fecal contact. The presence of the observer and the disclosure of our interest in hand hygiene may have changed the behavior so the associations between handwashing with soap and the specific characteristics may be spurious. However, educated persons would be the most likely group to recognize that the observers were interested in a public health conceptualization of handwashing behavior, and so be the most likely to change their behavior. The association of water and soap at the place to wash hands with handwashing was independent of education, suggesting that such bias is an unlikely explanation of the association. Indeed, the consistency of these results with experience in hospitals and ecological behavior change theory suggests that the association is not a result of bias. 12 A second limitation is that this program evaluation was not specifically designed to test the hypothesis that the presence of soap and water at the designated place to wash hands was associated with washing hands with soap. Thus, these results could have arisen by chance association and should not be considered as final confirmation of the hypothesis. However, these results did not come from mining the data for significant associations. Indeed, this analysis was outlined before the data were collected. Moreover, the associations were not borderline. The probability that either association would occur by chance is one in a thousand. Thus, while no single study is ever definitive, these data strongly support the hypothesis that having water and soap available at the place to wash hands improves the probability that both hands will be washed with soap following contact with feces. A third limitation is that the study population was restricted to 100 communities in rural Bangladesh. It was not a statistically representative sample of rural Bangladesh. No urban households were included, and outside of Bangladesh determinants of handwashing may be different. However, the study population is a large diverse sample from high need communities across rural Bangladesh, precisely the type of communities that would be expected to benefit most from improved handwashing behavior. Important barriers to realizing broader public health benefits from handwashing include the difficulty of changing handwashing habits and the difficulty in measuring handwashing behavior. These results suggest that interventions that improve the presence of water and soap at the designated place to wash hands would be expected to improve handwashing behavior and health. 13 Important next steps include active promotion of such interventions and careful evaluation of their impact on handwashing behavior and health. ACKNOWLEDGMENT This program evaluation was funded by the United Kingdom Department for International Development (DFID) through UNICEF Bangladesh. ICDDR,B acknowledges with gratitude the commitment of DFID and UNICEF to the Centre’s research efforts. Stephen P. Luby, Infectious Diseases and Vaccine Sciences, ICDDR,B, GPO Box 128 Dhaka-1000, Bangladesh, p : 88 02 988 1761 f: 8802 882 3963, sluby@icddrb.org Amal K. Halder, World Vision, Darfur, Sudan, Amal_Halder@wvi.org Carole Tronchet , UNICEF Bangladesh, BSL Office Complex, 1 Minto Road, Dhaka 1000, Bangladesh, Tel:(880-2) 9336701, Fax:(880-2) 9335641, Email: ctronchet@unicef.org Shamima Akhter, Department of Epidemiology, School of Public Health, University of Alabama Birmingham, shamima@uab.edu Abbas Bhuiya, ICDDR,B, GPO Box 128, Dhaka-1000, Bangladesh, abbas@icddrb.org Richard Johnston, Water and Environmental Sanitation Section, UNICEF Bangladesh BSL Office Complex, 1 Minto Road, Dhaka 1000, Bangladesh, Tel:(880-2) 9336701 ext. 486 14 Mobile: (880) 1713-030-536, Fax:(880-2) 9335641, Email: rjohnston@unicef.org 15 REFERENCES 1. Boschi-Pinto C, Velebit L, Shibuya K, 2008. Estimating child mortality due to diarrhoea in developing countries. Bull World Health Organ 86: 710-7. 2. Rudan I, Boschi-Pinto C, Biloglav Z, Mulholland K, Campbell H, 2008. Epidemiology and etiology of childhood pneumonia. Bull World Health Organ 86: 408-16. 3. Stanton BF, Clemens JD, 1987. An educational intervention for altering water-sanitation behaviors to reduce childhood diarrhea in urban Bangladesh. II. A randomized trial to assess the impact of the intervention on hygienic behaviors and rates of diarrhea. Am J Epidemiol 125: 292-301. 4. Pinfold JV, Horan NJ, 1996. Measuring the effect of a hygiene behaviour intervention by indicators of behaviour and diarrhoeal disease. Trans R Soc Trop Med Hyg 90: 366-71. 5. Han AM, Hlaing T, 1989. Prevention of diarrhoea and dysentery by hand washing. Transactions of the Royal Society of Tropical Medicine and Hygiene 83: 128-31. 6. Luby SP, Agboatwalla M, Painter J, Altaf A, Billhimer WL, Hoekstra RM, 2004. Effect of intensive handwashing promotion on childhood diarrhea in high-risk communities in Pakistan: a randomized controlled trial. Jama 291: 2547-54. 7. Luby SP, Agboatwalla M, Feikin DR, Painter J, Billhimer W, Altaf A, Hoekstra RM, 2005. Effect of handwashing on child health: a randomised controlled trial. Lancet 366: 225-33. 8. Omotade OO, Kayode CM, Adeyemo AA, Oladepo O, 1995. Observations on handwashing practices of mothers and environmental conditions in Ona-Ara Local Government Area of Oyo State, Nigeria. J Diarrhoeal Dis Res 13: 224-8. 16 9. Biran A, Rabie T, Schmidt W, Juvekar S, Hirve S, Curtis V, 2008. Comparing the performance of indicators of hand-washing practices in rural Indian households. Trop Med Int Health 13: 278-285. 10. Curtis V, Kanki B, Cousens S, Diallo I, Kpozehouen A, Sangare M, Nikiema M, 2001. Evidence of behaviour change following a hygiene promotion programme in Burkina Faso. Bull World Health Organ 79: 518-27. 11. Gilman RH, Marquis GS, Ventura G, Campos M, Spira W, Diaz F, 1993. Water cost and availability: key determinants of family hygiene in a Peruvian shantytown. Am J Public Health 83: 1554-8. 12. Luby SP, Halder AK, 2008. Associations among handwashing indicators, wealth, and symptoms of childhood respiratory illness in urban Bangladesh. Trop Med Int Health. 13. World Health Organization and UNICEF, 2008. Progress on drinking water and sanitation: Special focus on sanitation. New York: WHO/UNICEF. 14. Zeitlyn S, Islam F, 1991. The use of soap and water in two Bangladeshi communities: implications for the transmission of diarrhea. Rev Infect Dis 13 Suppl 4: S259-64. 15. Hoque BA, 2003. Handwashing practices and challenges in Bangladesh. Int J Environ Health Res 13 Suppl 1: S81-7. 16. Hanley JA, Negassa A, Edwardes MD, Forrester JE, 2003. Statistical analysis of correlated data using generalized estimating equations: an orientation. Am J Epidemiol 157: 364-75. 17. Vyas S, Kumaranayake L, 2006. Constructing socio-economic status indices: how to use principal components analysis. Health Policy Plan 21: 459-68. 17 18. Barros AJD, Victoria CG, 2005. A nationwide wealth score based on the 2000 Brazilian demographic census. Rev Saude Publica 39: 1-6. 19. Houweling TA, Kunst AE, Mackenbach JP, 2003. Measuring health inequality among children in developing countries: does the choice of the indicator of economic status matter? Int J Equity Health 2: 8. 20. Kaplan LM, McGuckin M, 1986. Increasing handwashing compliance with more accessible sinks. Infect Control 7: 408-10. 21. Graham M, 1990. Frequency and duration of handwashing in an intensive care unit. Am J Infect Control 18: 77-81. 22. Bischoff WE, Reynolds TM, Sessler CN, Edmond MB, Wenzel RP, 2000. Handwashing compliance by health care workers: The impact of introducing an accessible, alcoholbased hand antiseptic. Arch Intern Med 160: 1017-21. 23. Sallis JF, Owen N, Fisher EB, 2008. Ecological Models of Health Behavior. Glanz K, Rimer BK, Viswanath K, eds. Health Behavior and Health Education. San Francisco: Josey-Bass, 465-485. 24. Manun'Ebo M, Cousens S, Haggerty P, Kalengaie M, Ashworth A, Kirkwood B, 1997. Measuring hygiene practices: a comparison of questionnaires with direct observations in rural Zaire. Trop Med Int Health 2: 1015-21. 25. Stanton BF, Clemens JD, Aziz KM, Rahman M, 1987. Twenty-four-hour recall, knowledge-attitude-practice questionnaires, and direct observations of sanitary practices: a comparative study. Bull World Health Organ 65: 217-22. 18 26. Curtis V, Cousens S, Mertens T, Traore E, Kanki B, Diallo I, 1993. Structured observations of hygiene behaviours in Burkina Faso: validity, variability, and utility. Bull World Health Organ 71: 23-32. 27. Pinfold JV, 1990. Faecal contamination of water and fingertip-rinses as a method for evaluating the effect of low-cost water supply and sanitation activities on faeco-oral disease transmission. II. A hygiene intervention study in rural north-east Thailand. Epidemiol Infect 105: 377-89. 28. Kaltenthaler E, Waterman R, Cross P, 1991. Faecal indicator bacteria on the hands and the effectiveness of hand-washing in Zimbabwe. J Trop Med Hyg 94: 358-63. 29. Luby SP, Agboatwalla M, Billhimer W, Hoekstra RM, 2007. Field trial of a low cost method to evaluate hand cleanliness. Trop Med Int Health 12: 765-71. 19 Table 1. Characteristics of participating households, rural Bangladesh 2007, (N=527) n Percent/mean Number household residents 3042 5.8 Father of the youngest child lacks formal education 184 35 Mother of the youngest child lacks formal education 171 32 Drinking water source is a tubewell 505 96 Owns source of drinking water 170 32 Owns latrine 433 82 Uses improved latrine 416 79 Inside or near the toilet 198 38 Inside or near kitchen 47 9 Elsewhere in the yard 121 23 Outside the yard 136 26 No specific place 25 5 Water is available 378 72 Soap is available 276 52 Water and soap are available 225 42 Characteristic General Where the household usually washes hands after toileting At place of handwashing after toileting 20 Characteristics used in constructing wealth index Proportion who own House 493 93 Bicycle 132 25 Television (B/W) 109 21 Television (Color) 56 11 Refrigerator 15 3 Motor cycle 10 2 Sewing machine 42 8 Mobile phone 169 32 Wardrobe 155 29 Tables 527 1.1 Chairs 527 2.3 Watches/clocks 527 1.5 Beds 527 0.9 Inexpensive sleeping cots 527 1.4 Cement floor 55 10 Brick walls 52 10 Tin roof 479 91 Mean number of rooms 527 2.2 Mean number of items owned House construction 21 Electrical connection 236 45 Wood 133 25 Crop residue /grass / Dung 390 74 4 1 Median amount of homestead land (acre) 527 .08 Median amount of other land (acre) 527 .17 Cooking fuel Liquid gas/ gas 22 Table 2. The number and percentage of fecal contact events by age and sex (N=761) Age in years No (%) <3 9 (1) 3- <5 54 (7) 5- 12 90 (12) > 12 608 (80) Female 601 (79) Male 160 (21) Adult caregivers 438 (58) Adult (> 12 years) old non-caregivers 170 (22) Children (< 12) 153 (20) 23 Table 3. Household characteristics associated with washing both hands with soap after fecal contact (N=761 observed fecal contact events) Characteristic Number and proportion of persons with this characteristic who washed both hands with soap n (%) Number and proportion of persons without this characteristic who washed both hands with soap n (%) Adjusted odds ratio* (95% confidence limit) P-value Adult caregiver 102 (23) 9 (6) 4.3 (2.4, 7.3) <0.001 Adult non-caregiver 23 (14) 9 (6) 2.1 (1.0, 4.4) 0.05 Female sex 119 (20) 15 (9) 2.2 (1.3, 3.8) 0.004 Some primary education 40 (17) 25 (10) 1.8 (1.0, 3.1) 0.04 Above primary education 69 (26) 25 (10) 3.0 (1.8, 5.1) <0.001 Age (compared to child <12 years) Mother’s education (compared to uneducated) Father’s education (compared to uneducated) 24 Some primary education 37 (16) 37 (14) 1.2 (0.67, 2.0) 0.58 Above primary education 60 (23) 37 (14) 1.9 (1.1, 3.2) 0.03 2nd quintile 21 (14) 17 (11) 1.3 (0.64, 2.6) 0.47 3rd quintile 23 (16) 17 (11) 1.4 (0.72, 2.9) 0.30 4th quintile 32 (20) 17 (11) 2.0 (1.1, 3.9) 0.03 5th quintile 41 (26) 17 (11) 2.8 (1.4, 5.2) 0.02 Inside or near the toilet facility 56 (19) 30 (16) 1.3 (0.74, 2.3) 0.37 Inside or near kitchen 14 (21) 30 (16) 1.4 (0.60, 3.2) 0.44 Elsewhere in the yard 32 (18) 30 (16) 1.2 (0.64, 2.1) 0.63 2 (6) 30 (16) 0.33 (0.06, 1.7) 0.19 Wealth index (compared to poorest quintile) Where the household usually washes hands after toileting (compared to outside the yard) No specific place 25 At place of handwashing after toileting Water is available 116 (21) 18 (9) 2.7 (1.5, 4.7) <0.001 Soap is available 93 (24) 41 (11) 2.5 (1.3, 1.6) <0.001 Water plus soap is available 79 (24) 55 (13) 2.1 (1.4, 3.1) <0.001 Has separate soap for handwashing 39 (21) 95 (16) 1.2 (0.89, 2.1) 0.15 Has spare soap available in the household 55 (21) 79 (16) 1.5 (0.95, 2.3) 0.09 Buys soap weekly 47 (19) 87 (17) 1.2 (0.75, 1.8) 0.48 Drinking water source is shallow tube well 113 (18) 21 (15) 1.2 (0.64, 2.2) 0.59 Has other container to wash hands in 28 (21) 106 (17) 1.4 (0.81, 2.3) 0.25 Water observed in other container to wash hands in 16 (16) 118 (18) 1.0 (0.53, 1.9) 0.97 Has a household water tap 2 (40) 132 (18) 3.3 (0.47, 23.6) 0.23 111 (19) 23 (14) 1.3 (0.78, 2.2) 0.29 Has access to improved sanitation facilities *Odds ratio was calculated using a general estimated equations model that adjusted for neighborhood clustering and repeated sampling from the same household with a nested correlation structure. 26 Table 4. Multivariable analysis* of characteristics associated with handwashing Characteristic Adjusted Odds P-value ratio* (95% Confidence Limit) Age group compared to child <12 years of age Adult caregiver 4.2 (2.3, 7.6) <0.001 Adult non-caregiver 1.8 (0.78, 4.0) 0.17 Some primary education 1.6 (0.89, 2.7) 0.12 Above primary education 2.4 (1.4, 4.1) 0.002 Water is available 2.2 (1.3, 4.0) 0.006 Soap is available 2.1 (1.3, 3.4) 0.002 Mother’s education compared to uneducated At place of handwashing after toileting *Odds ratio was calculated using a general estimated equations model that accounted for neighborhood clustering and repeated household sampling using a nested correlation structure. 27 Figure 1. Sub-districts included in the SHEWA-B Health Impact Evaluation 28