Family clinic out-patient follow-up
advertisement

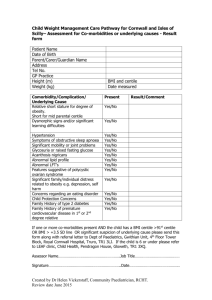
Family clinic out-patient follow-up Wt Ht SA OFC BP (Sticker) Clinical review Age: Date: Consultant________ Diagnosis knowledge kg centile___ Full: cm centile____ Partial: m2 None: cm centile____ HR Urinalysis Blood: Protein: Glucose: Leukocytes: Current medication Drug Susp/tabs Dose(in mg) Freq Adherence Any missed doses in last 7days Dose per kg / m2 Any missed doses in last month Body Shape Are you happy with the shape of your body? Do you think any part of you is too fat or too thin? Today’s changes Side effects of treatment Examination Pubertal stage Signs of Fat redistribution Increased central fat Thin limbs, buttocks Thin face yes / no yes / no yes / no Investigations performed today () FBC + diff T-cell subsets U+Es/LFTs Amylase Vitamin D/PTH Other Ix (specify) Cholesterol/TGs Lactate/bicarbonate Viral load (Roche/Chiron) CXR Diagnostic PCR HIV Serology Other virology (specify) New Referrals () Dentist Ophthalmology Multi-disciplinary Review Signature: __________________ Plan Next appointment: Growth chart? Flow chart? Where__________ When_________ Letter written? Signature: __________________