HEMOGLOBIN: Structure, Function & Disorders
advertisement

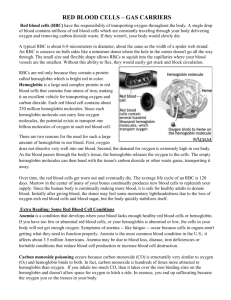
Red Blood Cells 1 Hemoglobin: Structure, Function & Disorders HEMOGLOBIN STRUCTURE: Hemoglobin is the oxygen carrying protein of red blood cells responsible for the red color characteristic of these cells. The amount of hemoglobin (Hb) present in red blood cells differs in males and females and varies also with age. Each hemoglobin molecule consists of 4 subunits and each subunit consists of a polypeptide chain conjugated to a heme moiety. Heme is an iron-containing porphyrin derivative and the polypeptides chains are collectively called globins. The 4 subunits of normal Hb are arranged as two pairs of different polypeptide chains. In normal adults, one pair of polypeptide chains is called the chains, each of which contains 141 amino acids and the other pair is called the chains, each consisting of 146 amino acids. Thus the structure of normal adult Hb, known as Hb-A, can be designated as 22. In adults, a small proportion of another type of Hb is also present, Hb-A2, representing about < 2.5% of the total Hb in blood. Instead of chains, Hb-A2 contains another type of polypeptide chain called , which is similar to but contains 10 different amino acid residues. Different hemoglobins are present in embryonic and fetal stages. Derivatives of Hb-A are also present in small amounts in normal blood. In one derivative called Hb-A1c the hemoglobin is glycosylated where glucose is attached to the terminal valine residue in each chain. Hb-A1c is elevated in patients with diabetes mellitus and is an indicator of the glucose levels in the preceding weeks to months. The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. Red Blood Cells 2 Hemoglobin: Structure, Function & Disorders HEMOGLOBIN SYNTHESIS: Heme synthesis: Heme synthesis occurs both in the cytosol and mitochondria in a series of enzymatically controlled steps that begins with the condensation of glycine and succinyl-CoA to form the first intermediary product -aminolevulinic acid. All successive steps are catalyzed by specific enzymes, the deficiency of each one leads to a group of disorders called Porphyria. The various steps of heme synthesis, the enzymes involved, and the disorders with their manifestations are shown in the figure below. [This picture is adapted from BLOOD: Principles & Practice of Hematology by Handin et al. Lippincott Press] The enzymes ALA Dehydratase & Ferrochetalase are inhibited by lead (Pb) that causes anemia in chronic lead poisoning, especially in children living in old houses with lead paint. [This picture is adapted from BLOOD: Principles & Practice of Hematology by Handin et al. Lippincott Press] The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. Red Blood Cells 3 Hemoglobin: Structure, Function & Disorders Globin synthesis: The two pairs of hemoglobin molecules are derived from two gene clusters: the globin gene cluster and the globin gene cluster. The globin gene cluster contains the gene, 2 and 1 genes and the globin gene cluster contains the , G, A, genes. During embryonic stages of development, the gene of the -chain gene complex associates with and chains of the globin gene complex form Hb-Gower 1 & 2, which are embryonic hemoglobins. Another embryonic hemoglobin called Hb Portalnd is formed by association of & chains. The various hemoglobins are also shown below. [The above picture is adapted from BLOOD: Principles & Practice of Hematology by Handin et al. Lippincott Press] The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. Red Blood Cells 4 Hemoglobin: Structure, Function & Disorders The sequence of expression of various chains of hemoglobin during various stages development is shown below. [This picture is adapted from BLOOD: Principles & Practice of Hematology by Handin et al. Lippincott Press] HEMOGLOBIN DEGRADATION: After an intravascular or an extravascular hemolysis or when old red blood cells are destroyed in the reticuloendothelial system, the globin portion of the hemoglobin molecule is split off and the heme is converted to biliverdin and finally to bilirubin. The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. Red Blood Cells 5 Hemoglobin: Structure, Function & Disorders HEMOGLOBIN FUNCTION: The main function of hemoglobin is to carry oxygen from lungs to peripheral tissues in the form of oxyhemoglobin; O2 attaches to the Fe+2 in the heme. This function is achieved by cooperative association of O2 with the heme moiety. The association of oxygen with heme and hence O2 saturation at a given O2 tension is governed by several factors including pH, temperature and the concentration of 2,3-DPG in red cells as shown below. The affinity of Hb-F for oxygen is greater than Hb-A. Nature has provided this property to Hb-F to facilitate movement of oxygen from maternal to the fetal circulation. From 828 weeks of gestation, Hb-F is the predominant form, accounting for almost all of the hemoglobin. The red cells of newborns, however, start forming Hb-A such that they have about 80% Hb-F and ~20% Hb-A and <0.5% Hb-A2. After 6 months of age, Hb-F is usually <1% of total hemoglobin. In some individual, however, fetal Hb persists long after without any clinical symptoms, a condition called hereditary persistence of fetal hemoglobin (HPFH). Hb-F is also increased as a compensatory mechanism in conditions causing decreased output of normal chains such as sickle cell anemia, Hb-C disease, thalassemia, and other conditions of chains. The embryonic hemoglobin forms also have oxygen affinity similar to Hb-F. When blood is exposed to various drugs and other oxidizing agents, the ferrous iron that is normally in the molecule is converted to ferric iron, forming methemoglobin. This Hb is darker in color and causes a dusky discoloration of the skin resembling cyanosis. Some oxidation of Hb to methemoglobin occurs normally, but an enzyme system in red cells, the NADH-methemoglobin reductase system, converts methemoglobin back to normal Hb. Congenital absence of this enzyme is one cause of hereditary methemoglobinemia. Carbon monoxide (CO) can also react with Hb to form carboxyhemoglobin. The affinity of CO is much greater for Hb than oxygen. This is why CO easily displaces O2 on Hb, thus reducing oxygen capacity of blood. The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. Red Blood Cells 6 Hemoglobin: Structure, Function & Disorders DISORDERS OF HEMOGLOIBIN: These are simply of two kinds A. Quantitative – called Thalassemias, and B. Qualitative – called Hemoglobinopathies THALASSEMIA: They are simply the result of reduced output of one or more globin chains and can be classified based on the type of globin chain deficiency. A total lack of synthesis of a chain is symbolized as 0 such as , and , whereas partial lack of a normal chain is characterized by a + sign such as , , , and . The genetic defects are either a deletion of the gene (partial or total) or any one or more of a variety of non-deletion mutations such as base substitutions in the gene itself or any of the regulatory regions. The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. Red Blood Cells Hemoglobin: Structure, Function & Disorders Clinical syndromes: Clinically all the thalassemia mutations can be categorized as follows: Clinically and hematologically normal: (Silent carrier state) 1. – 2. cs 3. /A Microcytosis with little or no anemia: (Thalassemia minor) (Asian type) 2. (African type) 3. cs/cs 4. 0/A 5. Lepore/A Microcytosis with moderate anemia: (Thalassemia intermedia) 1. African/African 2. 0 or + with or 3. ()o/()o 4. Lepore/Lepore Microcytosis with marked anemia: (Thalassemia major- <2 years of age) 1. 0/0 2. Medit/Medit Hemolytic anemia and microcytosis: (Hemoglobin H disease) 2. cs Lethal defects: (Hydrops fetalis) 1. for genes 2. mutants 3. ()0/()0 and thalassemia: The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. 7 Red Blood Cells 8 Hemoglobin: Structure, Function & Disorders See Robbins Pathologic Basis of Disease for a detailed description of each. HEMOGLOBINOPATHIES: These are the functional abnormal forms of hemoglobin and some of them are described in a table at the end of this handout. For sickle cell anemia see Robbins Pathologic basis of Disease. -Chain Abnormalities: -thalassemias1. 2. 3. 4. A/GA : no effect or slight hypochromia of fetal RBCs. Asymptomatic in adults. GA : mild hypochromia & microcytosis of fetal RBCs. Asymptomatic in adults. G or A : Moderate to severe fetal anemia with microcytosis. for -chains : incompatible with life. -hemoglobinopthies abnormal -Hb represents 10-20% of total Hb in the heterozygous states. No hematologic abnormalities except in Hb-F Poole, which presents with neonatal Heinz body hemolytic anemia. Unstable Hemoglobinopathies Several Hb variants that are unstable at high temperature (50 oC) and form a precipitate. About 100 variants have been described. About 75% are -chain variants and 25% are -chain variants. Heinz bodies (denatured Hb) are present in RBCs in most but not all cases. Patients usually present in early childhood with a hemolytic anemia, jaundice, and splenomegaly. Prominent basophilic stippling present. Red cell abnormalities are more pronounced after splenectomy. 1. Hb-Koln 2. Hb-Zurich 3. Hb-Indianapolis 4. Hb-Mississippi 5. Hb-Leiden 6. Hb-Gun Hill 7. Hb-Sydney 8. Hb-Bristol 9. Hb-Istanbul 10. Hb-Geneva The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. Red Blood Cells Hemoglobin: Structure, Function & Disorders The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. 9 10 Thalassemias Thalassemia type 0A African +African Medit+Medit A + Lepore /Lepore Lepore A / S +S C C E E thal thal CSCS CS CS Genetic defect Point mutations; deletions Point mutations; deletions/Hb-A Point mutations Point mutations Point mutations Point mutations; deletions/Hb-A Point mutations Point mutations Point mutations; deletions/Hb-S Point mutations/Hb-S Point mutations; deletions/Hb-C Point mutations/Hb-C Point mutations; deletions/Hb-E Point mutations/Hb-E Deletions Deletions Deletions Deletions Point mutations Deletions Various defects. Deletion. Point mutations. Deletion. Point mutations. Deletion. Point mutations. Deletion. Point mutations. Deletions, with or without gene Deletions and mutations Chain elongation mutation Deletions and mutations Hb g/dl 2-7 7-10 7-10 2-7 >10 2-7 2-7 >10 7-10 9-12 7-10 >10 2-7 7-10 9-10 >12 7-10 Normal Normal Normal 10-12 10-12 7-10 3-6 9-10 Normal 5-7 MCV fl 50-60 50-70 60-70 50-60 70-80 50-60 50-60 70-80 60-70 ~70 60-70 70-80 50-60 60-70 >80 70-80 60-70 Normal Normal 75-85 65-75 65-75 55-65 110-120 Normal - Hb-A Hb-A2 Hb-F Clinical features/Comments 0 ~90% ~65% 5-30% ~90% 2-10% 0 90% 0 5-40% 0 5-40% 0 5-40% 0 80% >95% Normal Normal Normal ~85% ~85% ~65% 0 Normal - 2-8% 3.5-8% 2-8% 2-8% 3.5-8% 3.5-5% 0 1.5-3% 3.5-5% 3.5-7% 3.5-5% 3.5-5% 3.5-5% 3.5-5% 0 <2% normal 0 Normal Normal 1.5-3% 1.5-3% <2% 0 Normal - >94% 1-5% 20-30% 60-90% 1-5% >85% 80-90% 3-5% 1-5% 1-5% 1-5% 1-5% 1-5% 1-5% 100% 5-15% normal Normal low Normal <1% <1% <1% 0 Normal - Thalassemia major. Mild at birth to 6 month of age. Premature death. Thalassemia minor. Thalassemia intermedia (African type). Thalassemia major (Mediterranean type ). Thalassemia minor. Thalassemia major. Mild at birth to 6 month of age. Thalassemia major. Hb-Lepore (-fusion protein) = 10-20% Thalassemia minor. Hb-Lepore (-fusion protein) = 2-5% Clinical severity like SS-disease. >90% Hb-S. Target & SS cells. Severity depends upon level of hemoglobin A. 60-70% Hb-S Thalassemia major. Hb-C = 95% Thalassemia intermedia. Hb-C = 60-70% Thalassemia major. Hb-E = 95% Thalassemia intermedia. Hb-E = 60-70% Thalassemia intermedia. High Hb-F thalassemia. Thalassemia minor. High Hb-F thalassemia. Heterocellular Hb-F Incompatible with life. Microcytic, hemolytic anemia in newborns. -thal trait in adults. May occur in other forms, ; A; A; 0 Asymptomatic, May occur in G-only or A-only varieties. Various syndromes. Severity depends on & chain imbalances. Silent carrier. Hb Bart’s () = 1-2% at birth; Hb-H (4) = rare -thal trait. Hb-Bart’s (4)= 5-10% at birth. Hb-H = rare. SE Asian -thal trait. Hb-Bart’s (4)= 5-10% at birth. Hb-H = rare. Africans Hb-H disease. Hb-H (4) in adults = 5-30%. Red cell inclusions. Hydrops fetalis. Hb-Bart’s = 80-95%; Hb-Portland (22)= 5-20% Hb-Bart’s ~15% in infants and ~5% in adults. Clinically and hematologically normal. 1% Hb-CS (longer proteins) Clinically Hb-H disease The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. 11 Hemoglobinopthies Hemoglobin variant Hb-S Genetic defect Ethnic group Homozygous or Heterozygous Heterozygous/Trait Homozygous/Disease 10% of American blacks. Clinically asymptomatic. A= 60; S = 33-40 0.2% of American blacks. Moderate to severe disease. Clinical features/Comments -6 Glu--Val African & American blacks -6 Glu--Val; -121 Glu--Gln American blacks Double heterozygous (rare) Moderate to severe hemolytic anemia & vasoocclusive complications. Sickled cells on smear. Neg sickle prep. Hb-S = 50%; Hb-D = 50% -6 Glu--Val; -6 Glu--Lys African & American blacks Double Heterozygous (0.13%) Mild chronic hemolytic anemia. Clinical course quite variable, from completely asymptomatic to severe. Hb-S = 50%; Hb-C = 50% Prominent target but rare SS-cells. Hb = 10-12 g/l. MCV = 70-90 -6 Glu--Val; -121 Glu--Lys African & American blacks Double Heterozygous Relatively severe chronic hemolytic anemia with vaso-occlusive episodes. -6 Glu--Val & -73 Asp--Asn American Blacks Heterozygous Double hetero with S Asymptomatic Resembles SS-disease Hb-C -6 Glu--Lys African & American blacks Heterozygous/Trait Homozygous/Disease Clinically and hematologically normal. 2% American blacks. 60:40 Mild hemolytic disease Hb-E -26 Glu--Lys South East Asia Heterozygous/Trait Homozygous Clinically asymptomatic. Slightly low MCV. Hb-E = 30% Clinically mild disease/-thal-trait. Low MCV. Hb-E = 99% Hb-DLA -121 Glu--Gln English/Irish; Punjab Heterozygous/Trait Homozygous Clinically & hematologically normal. Clinically not disabling. Hb-O Arab -121 Glu--Lys Arabs. African origin Heterozygous/Trait Homozygous/Disease 0.5% in American blacks. Hematologically and clinically normal. Hypochromia and microcytosis. Hb-GPhila -68 Asn--Lys African & American blacks Hb-SDLA Hb-SC Hb-SO Arab Hb-CHarlem Can occur with -thal with levels of Hb-G from 33-50% The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended. 12 The contents & pictures in this handout are derived from various sources including books, journal articles and patient material for teaching purposes only. No commercial incentives are sought or intended.