Application and Deposit Deadline: March 1, 2015
advertisement

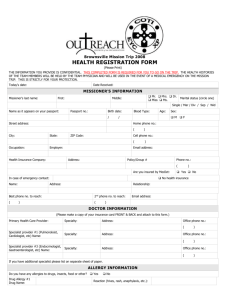
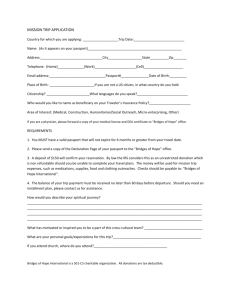
HONDURAS MISSION TRIP 2015 Mission Team Participant Application & Covenant Trip dates: June 19-27, 2015 Please note: The Team Leaders and Spiritual Director will keep the information contained in this sheet confidential. Personal Information: Name: Address: City: Home Phone: Other: Birth Date: Passport #: Zip: Cell Phone: Email Address: Marital status: Country of Issue: (PLEASE ATTACH A LEGIBLE PHOTOCOPY OF YOUR PASSPORT!) *International Law: Your passport must be current through 6 mos. beyond the return date of the trip! Place of Employment: Address: City: Job Title/Description: Zip: In the event of an emergency, please notify this person (someone not going to Honduras) Name: Address: City: St: Zip: Day Phone: Evening Phone: I am a member of Church of the Incarnation If you do not attend Church of the Incarnation, where do you worship? Congregation/Church Name: Spanish: How proficient are you? Speak _____________ Write______________ What specific skills do you have that you can contribute to our mission work? Construction Dental Education (Teaching, Art, Music) Spiritual Medical Other ____________________ HONDURAS MISSION TRIP 2015 Mission Trip Covenant By signing this sheet, I understand and agree to meet the following requirements. (Please check off each statement.) Before and during the trip, I will commit myself to praying for our trip and to attending team meetings. I will be responsible for obtaining financial support of my trip; including housing, meals, airfare, and necessary immunizations (current Tetanus is required). Cost per person is $1500. I understand that the application, covenant and the deposit of $200 are due at the time the application is submitted, and the remaining balance of $1300 will be due no later than May 1, 2015. (Partial need-based grant applications are available upon request.) For the success of this mission and the well-being of the entire team, I will follow the authority of the Team Leadership and Spiritual Director. I will cooperate with the Team Leaders’ directives and decisions throughout the entire mission. The Team Leaders for this trip are Larry Tate and Melanie Brewer. During the trip, I understand and will accept the conditions that may be different and uncomfortable compared with those I am used to. So that I will not hamper the team through avoidable illness, I will acquire all immunizations recommended by my personal physician and will carefully follow the health guidelines established for the team. I understand that I am expected to attend planning and informational meetings. The team retreat is Saturday, May 2 and Packing Day is Saturday, June 6. I understand that I will be part of a team, and I agree to work to promote team unity. I understand that on this trip, I am a representative of Church of the Incarnation and will be expected to act in ways becoming of Christians and, in this regard, will abstain from consuming excessive amounts of alcohol. I certify that all information I have supplied in this application is true to the best of my knowledge. Application and Deposit Deadline: March 1, 2015 I have attached: Legible photocopy of my passport Legible photocopy of both sides of my insurance card (personal insurance is required) Completed Health History Form Release Form Non-refundable deposit of $200 (payable to COTI, Memo: Honduras Payment) (Your application will be considered upon completion of all the above items.) Signature: _________________________________ Date: _____________ Please return to: Church of the Incarnation, attn: Mission and Outreach Department 3966 McKinney Avenue, Dallas, TX 75204 Email: outreach@incarnation.org or Fax: 214-528-7209 HONDURAS MISSION TRIP 2015 Release of All Claims, Waiver of Liability, and Assumption of the Risks 3966 McKinney Avenue, Dallas, Texas 75204-8211, (214)-521-5101 I, the undersigned, wish to participate, on a purely voluntary basis, in a mission/outreach activity of the Church of the Incarnation (COTI). This mission/outreach activity includes travel to and works in the country of Honduras from June 19 through June 27, 2015. I understand that this work is not for remuneration, but is volunteer/pro bono work, and is likely to involve manual labor and/or construction work in which I may not have expertise or skills. Never the less, I wish to participate, but understand that there is risk of injury which could arise in the course of this trip and the work in which we will engage. In consideration of being permitted to participate in this mission/outreach activity, I agree to be bound by this agreement, which provides for release of claims, waiver of liability, and assumption of the risks. Further, I sign this document and agree to its terms on behalf of myself, my heirs, executors and administrators, and assigns. I hereby WAIVE ANY AND ALL CLAIMS, ACTIONS, AND CAUSES OF ACTION OF ANY TYPE OR NATURE, I may now have or may have in the future against, and RELEASE FROM ALL LIABILITY, AND AGREE NOT TO SUE, the COTI, its vestry, teachers, employees, volunteers, agents, successors, and assigns for any accident, personal injury, death, property damage, damages of whatsoever kind or loss that I may suffer or be otherwise entitled to under the law, as a result of my participation in the mission/outreach activity or any activities related in any way thereto, due to any cause whatsoever, including, without limitation, negligence on the part of the COTI, its agents, employees, or volunteers. Further, I agree to indemnify COTI for any and all legal fees or cost that may be incurred in defending any lawsuit or claim I or my representatives may bring against COTI related to the above described activities. Additionally, I will HOLD HARMLESS AND INDEMNIFY COTI from any and all liability or claims for any loss, damage, injury, or expense brought by any third party, which claims result in any way from my participation in any activity related in any way to the above described mission/outreach activity. Finally, should I be injured during the course of the mission/outreach activity, and I am unable to communicate my authorization for medical treatment, I authorize COTI representatives to ask for medical treatment on my behalf, should the same be necessary. To that end, I have provided to the COTI my medical insurance coverage information. Signed this ____day of ________, 2015. Printed Name: Address: Phone: Signature: HONDURAS MISSION TRIP 2015 Health Registration Form THE INFORMATION YOU PROVIDE IS CONFIDENTIAL. THIS COMPLETED FORM IS REQUIRED FOR YOU TO GO ON THE TRIP. THE HEALTH HISTORIES OF THE TEAM MEMBERS WILL BE HELD BY THE TEAM PHYSICIAN AND WILL BE USED IN THE EVENT OF A MEDICAL EMERGENGY ON THE MISSION TRIP. THIS IS STRICTLY FOR YOUR PROTECTION. (Please Print) Today’s date: Date Received: MISSIONER’S INFORMATION Missioner’s last name: First: Mr. Mrs. Dr. Miss Ms. Middle: Marital status (circle one) Single / Mar / Div / Sep / Wid Name as it appears on your passport: Passport no.: Birth date: / Blood Type: Home phone no.: ( State: ZIP Code: Employer: Health Insurance Company: ) Cell phone no.: ( Occupation: Sex: M F / Street address: City: Age: ) Email address: Address: Policy/Group # Phone no.: ( Are you insured by MedJet: Yes No No health insurance In case of emergency contact: Name: ) Address: Relationship: Best phone no. to reach: 2nd phone no. to reach: ( ( ) Email address: ) DOCTOR INFORMATION (Please make a copy of your insurance card FRONT & BACK and attach to this form.) Primary Health Care Provider: Specialty: Address: Office phone no.: ( Specialist provider #1 (Pulmonologist, Cardiologist, etc) Name: Specialty: Address: Office phone no.: ( Specialist provider #3 (Endocrinologist, Gastroenterologist, etc) Name: Specialty: Address: ) ) Office phone no.: ( ) If you have additional specialist please list on separate sheet of paper. ALLERGY INFORMATION Do you have any allergies to drugs, insects, food or other? Yes Drug Allergy #1 Drug Name: Drug Allergy #2 Drug Name: Insect Allergy #1 Insect Type: No *please note any anaphylactic Reaction (hives, rash, anaphylaxis, etc.): Reaction (hives, rash, anaphylaxis, etc.): Reaction (hives, rash, anaphylaxis, etc.): reactions you have had to any medications* Insect Allergy #2 Insect Type: Food Allergy #1 Food Type: Food Allergy #2 Type: Other Allergy #1 Type: Other Allergy #2 Type: Reaction (hives, rash, anaphylaxis, etc.): Reaction (hives, rash, anaphylaxis, etc.): Reaction (hives, rash, anaphylaxis, etc.): Reaction (hives, rash, anaphylaxis, etc.): Reaction (hives, rash, anaphylaxis, etc.): Have any reactions ever required emergency room care?_______ Please list all allergies, if needed please use separate sheet of paper. CURRENT HEALTH PROBLEMS Problem #1 (i.e. diabetes, high blood pressure): Medicine you are taking for this: Problem #2 (i.e. diabetes, high blood pressure): Medicine you are taking for this: Problem #3 (i.e. diabetes, high blood pressure): Medicine you are taking for this: Please use additional sheets of paper for any additional problems you feel the Team Doctor(s) should know about. Asthma Angina Diabetes Migraines Ulcers Bleeding abnormalities Kidney Stones Gall Stones Seizures/Epilepsy Alcohol/drug Addition Heart Disease Hearing Disorder Hypertension Orthopedic Condition Skin Disorder Eye/Vision Disorder Psychiatric Disease: Bipolar Schizophrenia Anxiety Depression Blood Pressure average Reading: Thyroid Disease High/low Blood Pressure Diabetic last HgbA,C: Please explain any of the above: Past Major Surgery #1 Date: Surgery: Past Major Surgery #2 Date: Surgery: Past Major Surgery #3 Date: Surgery: MEDICATIONS Please list all PRESCIPTION medications you are take (including the ones listed above): Name of Drug: Dosage: Frequency: Purpose: Please list all OVER-THE-COUNTER medications you are take (including the ones listed above AND vitamins): Name of Drug: Dosage: Frequency: Purpose: Tetanus shot is required for all Mission Trips. Tetanus Shot: Yes Date: Hepatitis A Inoculation: Yes No Date: Typhoid Immunization: Yes No Date: Hepatitis B Inoculation: Yes No Date: Other information you would like us to know: