1. venipuncture
advertisement

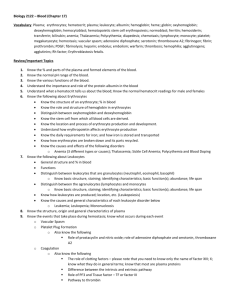
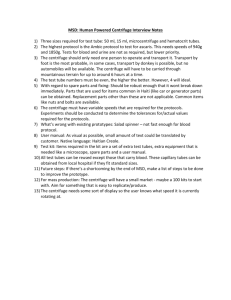
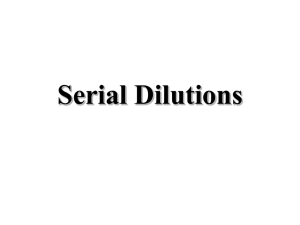
P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D 1. VENIPUNCTURE Most routine hematological studies are performed on venous blood, which is usually obtained from an antecubital vein. Occasionally, in very obese persons or those whose veins have been thrombosed by chemotherapy, it may be necessary to puncture one of the veins on the forearm or on the dorsum of hand. Materials: Cotton swab Disinfectant (Ajatin) Tourniquet Sterile plastic disposable syringe and sterile disposable needle Plaster Procedures: 1. Attach a sterile needle with its cover to the syringe. 2. Apply a tourniquet round the upper arm over the middle of the biceps. 3. Choose a vein for venipuncture. It should be straight, not tortuous, and should be well fixed in the subcutaneous tissue so that it does not roll away. Patient's arm should be extended. 4. Carefully clean the skin at the cubital fossa with a swab soaked in Ajatin. 5. Stretch the skin at the cubital fossa by one hand. Push the needle with the syringe attached through the skin and then slowly into the prominent vein with the opposite hand. The direction of the needle should be almost parallel with the vein chosen for obtaining blood. 6. Try to draw up small amount of blood into the syringe to make sure that you managed to puncture the vein. 7. Remove the tourniquet and draw up amount of blood required. 8. Withdraw the needle from the vein and immediately place a swab on the puncture site. Instruct the patient to hold his forearm firmly flexed against his arm for a minute or so. 9. Strap the puncture site. 10. Blood obtained by venipuncture place immediately into a specimen container suitable for the particular test required. CAUTION: Procedure of blood manipulation should be slow and careful because of easy damage to blood cells and hemolysis. Hemolysed blood should not be used for many kinds of blood tests. It is necessary to remove the needle before releasing obtained blood into a container. The needle used for obtaining blood should be sharp and it should have sufficient diameter. 2. SEDIMENTATION RATE (ACCORDING TO FAHRAEUS AND WESTERGREEN) If the blood is kept fluid by means of an anticoagulant and is allowed to stand in a narrow tube, the corpuscles settle progressively to the bottom leaving clear plasma above. The rate at which this takes place is known as sedimentation rate. Normally the sedimentation rate is 2 – 5 mm/hour in males and 3 - 8 mm/hour in females. Materials: Citrated human blood (1 part of sodium citrate 3.8 % and 4 parts of blood) Wintergreens sedimentation apparatus with narrow graduated tube 1 P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D Figure 1. Wintergreens sedimentation apparatus: a) before filling, b) initial adjustment - Wintergreen’s narrow tube filled with blood to 0 mm mark, c) after one hour sedimentation rate as height in mm of the column of clear plasma = 5 mm/h Procedures: 1. Fill the tube with citrated blood to the 0-mm mark. 2. At the end of one and two hours read the height in mm of the column of clear plasma. See figure 1. 3. Compare your result with normal values. Results: Conclusion: 2 P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D 3. DETERMINATION OF HEMOGLOBIN CONCENTRATION Hemoglobin is essential for oxygen carriage and participates in the transport of carbon dioxide. In a healthy adult man the hemoglobin content of blood is 135 - 170 g/l (average content 150 g/l), in a healthy adult woman 120 - 158 g/l (average content 140 g/l). Materials: Non-coagulating human blood (an anticoagulant: sodium EDTA) 20 mm3 blood pipette with rubber tube and disposable mouthpiece Drabkin's cyanmethemoglobin reagent solution (caution: poison!) 5 ml automatic burette Test tubes Cyanmethemoglobin standard solution Carl Zeiss Jena Specol spectrophotometer and spectrophotometer cuvettes Procedures: 1. Measure off 5 ml Drabkin's cyanmethemoglobin reagent solution with an automatic burette and place it in a test tube. 2. Collect 20 mm3 of blood with a blood pipette, add this sample to the test tube and mix thoroughly. 3. Allow the tube to stand for at least 10 minutes. 4. Read the absorbance of the standard and the blood sample in a spectrophotometer at 540 nm wavelengths. Use the tube with the reagent solution as the blank for all spectrophotometer readings. (Absorbance readings are determined by a lab technician.) 5. Calculate the hemoglobin concentration of the sample according to the formula: hemoglobin hemoglobin concentrat ion absorbance of the sample concentrat ion absorbance of the standard (g/l) in the standard 251 (dilution) 0,001 (to convert to g/l) 6. Compare your value with standard values. Results: Conclusion: 4. HEMATOCRIT DETERMINATION The test specifically measures the relative volume of erythrocytes in the blood. The hematocrit value is 44 5 % for men and 39 4 % for women. 3 P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D Materials: Non-coagulating human blood (with sodium EDTA as the anticoagulant) Heparinized capillary tubes Laboratory burner Safety matches Hematocrit centrifuge Hematocrit reader Procedures: 1. Allow the blood to fill 4/5 of two capillary tubes. 2. Seal the free end of the tubes in the flame of a laboratory burner. 3. Place the tubes in a hematocrit centrifuge with the sealed ends directed outward, one opposite the other. 4. Secure the top of the centrifuge and spin for 2 minutes at 16 000 r.p.m. (revolutions per minute). 5. Remove the tubes from the centrifuge and determine the hematocrit value as the ratio of packed cells to the total blood volume according to figure 2. 6. Compare your value with physiological (standard) values. Figure 2. Hematocrit reader: a) initial adjusting, b) hematocrit reading Results: Conclusion: 4 P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D 5. DETERMINATION OF MCH, MCHC, MCV MEAN CELL HEMOGLOBIN (average amount of hemoglobin per cell) mean cell hemoglobin hemoglobin in grammes per litre of blood red cells count per litre Normal values are 28 - 32 pg. MEAN CELL HEMOGLOBIN CONCENTRATION (amount of hemoglobin in 1 liter of red corpuscles) mean cell hemoglobin concentration = hemoglobin in grammes per litre of blood hematocrit Normal values are 300 - 350 g/l. If the corpuscular hemoglobin concentration is within the normal range the cell is normochromic; if it is below the normal range the cell is hypochromic. MEAN CELL VOLUME hematocrit red cells count per litre The normal range is 85 10 fl. Cells of average volume are called normocytes; cells whose volume exceeds the normal range are called macrocytes, while small cells are called microcytes. mean cell volume = Calculate the MCH, MCHC, and MCV in the following cases: 1) woman, 29 years old, red cells count: 4.2 x 1012/l; hematokrit 0.38; hemoglobin 142 g/l 2) man, 55 years old, , red cells count: 4.25 x 1012/l; hematokrit 0.32; hemoglobin 108 g/l Results: Conclusion: 6. FRAGILITY OF RED CORPUSCLES IN HYPOTONIC SALINE Because of the higher osmotic pressure inside the cells in hypotonic saline, fluid passes into the corpuscles until they burst and their hemoglobin is liberated. Normally hemolysis begins in 0.4 % NaCl (minimal resistance) - old erythrocytes are only destroyed, and it is complete at 0.3 % NaCl (maximal resistance). 5 P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D Materials: Non-coagulating human blood (an anticoagulant: sodium EDTA) Test tubes with distilled water 1 % NaCl Pipettes Pasteur’s pipette Procedures: 1. Prepare a series of hypotonic NaCl solutions in a set of test tubes, using 1 % NaCl solution and distilled water. See table 1: (ml) 0.5 1.0 1.5 (ml) 4.5 4.0 3.5 0.8 (%) 0.9 Distilled water: 2.0 2.5 3.0 3.5 4.0 4.5 1 % NaCl solution: 3.0 2.5 2.0 1.5 1.0 0.5 Final concentration of NaCl: 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Table 1. 2. Add one drop of blood to every test tube and gently mix. 3. Allow the tubes to stand for approximately 2 hours and after this exposure observe the content of tubes. Erythrocyte sediments and colorless NaCl solutions above them are seen in tubes with isotonic and slightly hypotonic NaCl. When hemolysis begins, red NaCl solution is visible above the erythrocyte sediment (read minimal osmotic resistance). All erythrocytes ruptured in tubes with red NaCl solution without any sediment. The highest concentration of NaCl with complete hemolysis is denoted as maximal osmotic resistance. See figure 3. 4. Compare your results with physiological values. Figure 3. Test tubes with erythrocytes in hypotonic NaCl: a) erythrocyte sediment + colorless NaCl solution, b) erythrocyte sediment + red NaCl solution (minimal fragility), c) red NaCl solution without erythrocyte sediment (maximal fragility) 6 P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D Results: Conclusion: 7. QUICK’S PROTHROMBIN TIME This is a test for deficiency in clotting factors I, II, V, VII, X in vitro because prothrombin - to thrombin reaction proceeds here by means of the extrinsic clotting pathway. The normal human prothrombin time is approximately 12 seconds and the length of its duration is used to control clotting in patients treated with vitamin K antagonists (for example dicoumarol). Their administration prolongs Quick’s prothrombin time. Materials: Citrated human blood (9 parts of blood, 1 part of sodium citrate 3.8 %) Normal saline Test tubes Reagent (CaCl2 solution and tissue thromboplastin) Pasteur’s pipette Pipettes Water bath (37oC) Glass stick Procedures: 1. Centrifuge citrated blood for 5 minutes at 3 000 r.p.m. 2. Separate plasma with Pasteur’s pipette. 3. Mix 0.1 ml plasma and 0.2 ml reagent. All ingredients are incubated at 37°C. The time taken for fibrin threads to form after the addition of reagent is measured. 4. Make this test also with 50 % (one part of 100 % plasma, one part of normal saline), and 25 % (one part of 50 % plasma, one part of normal saline). With plasma dilution the concentration of blood clotting factors falls and blood coagulability is depressed, Quick’s prothrombin time is prolonged. 5. Construct the curve showing the relationship between prothrombin time and plasma dilution. Results: Graph: 7 T R A I N I N G I N P H Y S I O L O G Y O F B L O O D Time (sec) P R A C T I C A L 25% 50% 100% Plasma dilution Conclusion: 8. BLOOD TYPING Blood typing is based upon the presence of certain antigenic substances localized on the red cell membrane. The most powerful antigens comprise the AB0 series. Other substances found on the erythrocyte membrane define the Rh series. Materials: Cotton Disinfectant (Ajatin) Sterile needles Paper cards Microscope slides Anti-A, anti-B, and anti-Rh (anti-D) blood sera Procedures: 1. Disinfect your finger with Ajatin, allow it to dry, and puncture with a sterile needle. 2. Allow one drop of your blood to fall into each of two large circles on the paper card (see figure 4) and one drop on a microscope slide. 3. Carefully place one drop of anti-A serum in first small circle, one drop of anti-B serum in second small circle, and two drops of anti-Rh serum on the slide. 4. Mix the blood and anti-sera with corners of the slide and observe results. Agglutination should occur within 2 minutes with anti-A and anti-B serum and within 5 minutes with anti-Rh serum. The results in the AB0 system are diagnosed by the following table (table 2). The Rh blood group is 8 P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D determined as follows. If the anti-Rh serum agglutinates erythrocytes, the individual has Rh+ blood. When no agglutination with anti-Rh serum occurs, the blood is Rh-. Figure 4. Paper card for blood typing in the AB0 series Serum anti-A anti-B Blood group + + - + + - A B AB 0 Table 2. Blood typing in the AB0 series using anti-A and anti-B sera: (+) agglutination, (-) no agglutination 5. Describe reactions with anti-A, anti-B, and anti-Rh agglutinins and determine your blood group in AB0 and Rh systems. Results: Conclusion: CROSS - MATCHING OF BLOOD Before transfusion, it is advisable to test directly the donor’s cells against the recipient’s serum, and the recipient’s cells against the donor’s serum, a procedure known as cross-matching. This is a precaution not only against errors in grouping, but also tests for the presence of other agglutinins, which may occasionally be present. Materials: Test tubes Pipettes Pasteur’s pipette Recipient’s and donor’s blood (HIV and HBsAg negative) 9 P R A C T I C A L T R A I N I N G I N P H Y S I O L O G Y O F B L O O D Centrifuge Microscope slides and cover glasses Microscope Physiological solution of NaCl Procedures: 1. Remove plasmas recipient’s and donor’s bloods with Pasteur’s pipettes into the tubes marked RPl (recipient’s plasma) and DPl (donor’s plasma). 2. Prepare suspensions of red corpuscles. The suspensions must be prepared from cells that had been washed. Add physiological saline solution to blood cells and centrifuge for 5 minutes at 5 000 r.p.m. Pipette off the supernatant fluid and use erythrocyte sediment for the preparation of a 2 % suspension. Place 0.1 ml of washed donor’s erythrocytes to the tube ErDP and 0.1 ml of washed recipient’s erythrocytes to the tube ErRP. Add 4.9 ml of physiological saline to both test tubes. 3. Turn the suspensions a few times upside down closing the mouth of the test tube with your thumb. 4. Prepare colloid erythrocyte suspension mixing one drop of blood cells with 1.0 ml of corresponding plasma in test tubes ErRC and ErDC. It is important not to have the colloid suspension too thick. 5. Make cross - matching by mixing equivalent volumes (0.1 ml) of ingredients as shown in the table3: donor’s plasma DPl recipient’s erythrocyte suspension DPl+ErRP in physiologic solution of NaCl (ErRP) colloid recipient’s erythrocyte suspension DPl+ErRC (ErRC) suspension of donor’s erythrocytes ----------------------in physiologic solution of NaCl (ErDP) colloid donor’s erythrocyte suspension ----------------------(ErDC) recipient’s plasma RPl --------------------------------------------------RPl+ErDP RPl+ErDC Table 3. 6. After 10 minutes incubation centrifuge the test tubes for one minute at 1 000 r.p.m. 7. Make readings of agglutination with the naked eye and by means of a low power objective of the microscope. When no agglutination in any test tube occurs, the donor’s and recipient’s bloods are compatible and the donor’s blood may be used for transfusion. Results: Conclusion: 1 0