Ch. 2 Sallis
advertisement

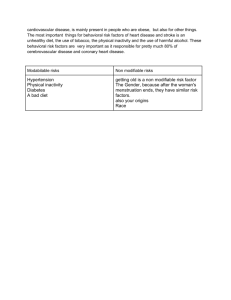
PHYSICAL ACTIVITY, LONGEVITY AND PHYSICAL HEALTH - first step in behavioral epidemiology framework is to establish link between physical activity and health – no doubt, this has been done summary of current scientific understanding of the effects of physical activity and inactivity on indicators of physical health PHYSICAL ACTIVITY AND LONGEVITY - studies of this type help answer the question of whether exercise adds years to life - best answer; it consistently reduces risk of dying at any one point in time - physically active individuals live longer, therefore the benefits outweigh the risks - most common type – assess physical activity in a sample population at some endpoint, compare morbidity rates between those physically active and those that are not - classic study by Paffenbarger, et al. 1986, showed all-cause mortality reduced by 53% in men who played sports 3 or more hrs per week compared to those < 1 hr per week death rates 33% lower in men who walked > 15 km per week compared with men who walked < 5 km per week active men lived ~ 2 years longer than inactive men Blair et al (1989) used fitness measures (as opposed to subjective questionnaire responses and found that highest fit men had a 71% lower death rate than fit men also, men in lower high fit categories had lower death rates (60% all-cause mortality) than least fit men analogous findings were also shown for women subsequent studies by Blair (1996) showed that independent of other risk factors – those with higher fitness levels had lower death rates - what about changing fitness category? Paffenbarger et al. (1993) – evaluated the changing of physical activity levels in 10,000 men and concluded: compared with men physically inactive at two different assessments, those who became active decreased risk by 15% (44% reduction as reported by Blair et al. 1995), those who became inactive increased their risk by 10% - last question: How much activity is needed for health benefits? Figure 2-1 what is the general trend and where are the greatest benefits seen? PHYSICAL INACTIVITY’S CONTRIBUTION TO THE BURDEN OF DISEASE AND PREMATURE DEATH - estimate the number of deaths for which physical inactivity is responsible – “population attributable risk” is based on RR associated with inactivity and the prevalence of inactivity in the population - for example, inactivity doubles risk of CHD; high prevalence > 50% < recommendations - population attributable risk is large – Hahn et al (1990) estimated > ¼ million deaths in 1985 could have prevented if physical inactivity was eliminated ~ 23% of all deaths; while 33% smoking, 23% lipids, 24% obesity PHYSICAL ACTIVITY AND CARDIOVASCULAR DISEASE - physical activity decreases all-cause mortality by reducing risk of cardiovascular diseases (the most common form of death in industrialized nations) - arteriosclerosis in the arteries which eventually leads to blockage of blood flow - heart attack – blockage in the heart; stroke – blockage in the brain - CHD is most deadly form of CVD - there is a dose-response relationship with the largest change occurring from sedentary to some level of activity ~35% of deaths from CHD due to physical inactivity; HP 2000 – 30% goal PHYSICAL ACTIVITY AND RISK FACTORS FOR CARDIOVASCULAR DISEASE - statistically adjusting for other risk factors for CVD decreases strength of association with physical activity - indicative of what? – positive influence of physical activity on other risk factors - vigorous activity reduces risk of hypertension 19-30% in men; physically active women 30% less likely to get hypertension then sedentary (6-7 mm Hg drop in both systolic and diastolic) - cholesterol? – physical activity doesn’t necessarily affect total cholesterol or LDL cholesterol; however, physical activity increases HDL: 20-30% higher in endurance trained athletes; HDL – reverse cholesterol transport PHYSICAL ACTIVITY AND PREVENTION OF OBESITY Physical Activity and Body Fat - overweight and obesity linked to several diseases: CVD, hypertension, cancer - excess body fat is the culprit; however, difficult to measure in epidemiological research - BMI = wt (kg)/ht2(m) - overweight increasing rapidly: 1970 – 25%; 1990 – 33% (adults); 10.9% of children > 95th percentile compared to children in 1963 (more than doubled) - highest prevalence: African-American and Mexican-American women 49 and 47%, respectively - excess body fat believed to develop from energy imbalance – genetics also plays a role – however, prospective studies generally support effectiveness of physical activity in preventing excess weight gain Fitness or Fatness? - fit men had same risk of dying no matter status of overweight PHYSICAL ACTIVITY AND WEIGHT LOSS - exercise alone results ~ 3 kg weight loss - not much, but the combination of weight loss (fat) with increases in muscle mass lead to exponential benefit - physical activity – very important in the maintenance of weight loss PHYSICAL ACTIVITY AND DIABETES - excessive levels of glucose in the blood and inability of insulin to metabolize it (insulin resistance) - NIDDM ~ 90% of all cases of diabetes – 3-6% prevalence with equal numbers being undiagnosed - higher for non-Caucasian and 40-80% higher for females - can lead to blindness and liver disease – but, most importantly a CVD risk factor - can be eliminated through weight loss - - positive benefits of physical activity in two ways: o reduces blood glucose and increase insulin sensitivity o reduces central obesity 15% reduction for women who exercised vigorously at least once per week; 25% in men population attributable risk – physical activity responsible for 35% of NIDDM deaths now recognized as important as prescription medication in treatment PHYSICAL ACTIVITY AND CANCERS - second leading cause of death in many industrialized nations - lung, breast, prostate and colon - 32% of deaths due to colon cancer – physical inactivity (“PAR”) - some evidence for prostate and breast cancer PHYSICAL ACTIVITY AND OSTEOPOROSIS - peak bone mass and rate of decline determine risk of osteoporosis – both of which are directly related to physical activity PHYSICAL ACTIVITY AND FUNCTIONING IN THE ELDERLY - ADL - loss of function is due to inactivity PHYSICAL ACTIVITY AND LOW-BACK FUNCTION - experienced by 80% of population at some point in life - not much evidence one way or the other PHYSICAL ACTIVITY, PSYCHONEUROIMMUNOLOGY AND HIV - the study between psychological variables, the nervous system and the immune system - evidence is emerging that demonstrates positive affects of physical activity in dealing with the stress of HIV also, important for enhancing strength of immune system – decreases depression, decreases strength of stress inducing hormones (cortisol and catecholamines), increases beta endorphins and direct and positive effects on immune system HEALTH RISKS OF PHYSICAL ACTIVITY - benefits should outweigh the risks - risks include musculoskeletal injuries and cardiac deaths - risks and benefits – Table 2.1 PHYSICAL ACTIVITY AND THE HEALTH OF CHILDREN AND ADOLESCENTS - influence morbidity but not mortality, why? - positive affects on body weight, psychological stress, athletic performance, strengthen immune system - reduces risk for CVD as an adult - aerobic fitness important now and in the future a difficult parameter to measure and elicit statistical relationship with other, logical parameters - overweight and obesity – similar to fitness levels measures of sedentary living and adiposity are very consistent and strong - Table 2.2 – Physical Activity and Health SUMMARY - ~ 200,000 deaths attributable to sedentary lifestyles each year