ECG`S MADE EASY
advertisement

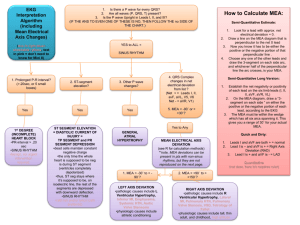
ECG’S IN THE ER Steven L. Marks BVSc, MS, MRCVS, DACVIM Small Animal Track 2012 ISVMA Annual Conference Proceedings The electrocardiogram or ECG is a valuable component of the medical evaluation of many dogs and cats. It can also be a useful tool for monitoring patients during hospitalization. It is imperative that a rapid and accurate rhythm diagnosis can be made so appropriate therapeutic intervention can be made. The ECG is most valuable when used in combination with a complete medical history and physical examination. It is also often used in combination with a diagnostic data base which may vary dependent on the clinical setting and the suspected differential diagnoses. It is important to remember that abnormalities detected on the ECG may be due to cardiovascular disease or diseases affecting systems other than the cardiovascular system. How to Perform the ECG Patients should be placed in right lateral recumbency. If using a metallic table top a blanket or cushion should be used to prevent artifact. There are generally 4 leads to attach to the patient. There are several techniques for attaching leads but the easiest for recording is to use alligator clip leads. These can be used in conjunction with alcohol or water soluble gel to help conduction. The leads should be placed behind the elbows on the forelimbs and over the stifles on the hindlimbs. The leads of the electrocardiograph are color coded, red, green, black and white. These colors correspond to placement on the patient. Lead White Black Green Red Leg Right forelimb Left forelimb Right hind limb Left hind limb There are several pneumonics that can be used to remember which colors go to which limbs. One is if you think of yourself driving your car on a sunny day, your left arm is out the window and getting tan (black) while your right arm remains in the car (white). Your right foot uses the brake to stop (red) and the gas to go is on the left (green). Your patient should be as calm as possible when recording the ECG, as motion such as struggling and tremors will cause artifact. When ready to record the ECG the settings on the electrocardiograph should be checked. It is considered standard to record leads I, II, III, AVR, AVL and AVF at a sensitivity of 1.0 cm = 1.0 mv and a paper speed of 50 mm/sec. An additional lead II recording can be made at 25 mm/sec and is referred to as a rhythm strip. Each lead should be recorded for a couple of seconds and the rhythm strip for longer. Once the recordings are made they should be labeled with the patient name and or number, time and date. ECG Interpretation There are 4 basic steps to follow when evaluating an ECG. It is crucial that you follow these 4 steps consistently in order to not make interpretation errors. Step 1: RATE. Calculate heart rate. The nice aspect of this procedure is you have a gold standard to compare it to and that is the pulse or the heart rate you can auscult on the patient. There are several techniques for calculating heart rate. One technique is to use ECG paper with time marks. The time marks are set at intervals of 15 boxes. When an ECG is run at a paper speed of 50 mm/sec each large box represents .1 seconds and therefore counting 30 boxes or between 2 time marks is 3 seconds. By counting the number of complexes in 3 seconds and multiplying by 20 (3 x 20 = 60) you are able to calculate the number of beats per one minute. Another easy technique is to take a standard sized pen. In most cases the length of a Bic® or Paper Mate® ballpoint pen is 30 boxes. If the paper speed is 50 mm/sec, the number of complexes counted within these 30 boxes multiplied by 20 will provide the number of beats per minute. The third technique for calculating heart rate is to count the number of small boxes between two R complexes. If the paper speed is 50 mm/sec 3000 is divided by the number of small boxes to calculate a spontaneous heart rate. Step 2: RHYTHM. Evaluate if the rhythm is regular or irregular. It is also valuable to evaluate if the complexes are conducted from a supraventricular focus or a ventricular focus. As a rule of thumb, normal complexes should be upright and narrow, ventricular complexes tend to be wide and bizarre. The question should also be asked is there a P wave for every QRS complex and is there a QRS complex for every P wave. Step 3: MEA. This is the mean electrical axis. The MEA tells the main direction of electrical activity within the heart. Normal for the dog is 60-90 degrees. The clinical significance of the MEA in the cat is unknown. There are several techniques to calculate the MEA. The first technique is to identify the isoelectric lead. This lead is the lead with the same approximate positive deflection on the QRS complex as negative deflection. Once this lead is identified, the perpendicular lead is identified. By evaluating the QRS complex as positive or negative on this lead indicates the MEA. A second technique involves looking at all six leads and determining which lead has the tallest QRS complex. The direction of deflection on this lead (positive or negative) is the MEA. The final technique is to examine leads I and AVF. As you can see from the figure above these leads divide the chart into 4 quadrants. The next step is to look at lead I and lead AVF and see if the QRS complexes are negative or positive on those leads. On a normal ECG lead I and lead AVF will have positive QRS complexes. This means that the MEA is between 0 and 90 degrees. Now if we compare the size of the QRS complexes on lead I and lead AVF, which ever is larger means the MEA is closer to that direction. Step 4: Measure Complexes. Evaluate and measure the P QRS T complexes and intervals. This is when you must know the published normal values for with width and height of all complexes. Measure the following: P-wave PR interval QRS complex ST segment T-wave QT interval P wave: The P wave is represents the depolarization of the atria. The duration of the P-wave indicates the time the impulse takes to travel from the SA node to the AV node. The evaluation of the P-wave should include the height and the width. A wide p-wave is suggestive of left atrial enlargement. A tall p-wave is suggestive of right atrial enlargement. PR interval: This is the time required for the impulse to travel from the SA node to the ventricle. It is actually measured as the PQ interval. QRS complex: The evaluation of the QRS complex should also include height and width. For the most part increase amplitude of the QRS complex implies left ventricular enlargement, while increased duration (widening) of the QRS implies right ventricular enlargement. ST segment: This is measured from the end of the QRS complex to the T wave. The segment may be depressed or elevated. It can be affected by many factors including heart disease and electrolyte abnormalities. T wave: The T wave represents repolarization of the ventricles. Evaluation of the T-wave is primarily based on size and it should be no greater than ¼ of the height of the R wave. QT interval: The QT interval is measured from the start of the Q wave until the end of the T wave. This interval will change with heart rate. It is not commonly used for diagnostic criteria in veterinary patients. Suggested Reading Edwards NJ. Bolton’s Handbook of Canine and Feline Electrocardiography. WB Saunders, 1998. Tilley LP. Essentials of Canine and Feline Electrocardiography. WB Saunders, 1992