LabDx-I_test1oldnotes

Friday, September 12, 1997:
Discussion of article and the questions handed in:
**Likes synthesis of knowledge questions and not the recall type of question**
**Know the flow chart on the back of the handout given to us the first day**
1.What are the most essential components of the differential diagnosis?
History and physical examination
PATIENT MANAGEMENT: broken down into diagnosis and treatment. The patient doesn’t have a
preference of which one they want they want both. Both issues must be addressed.
These are components of data acquisition.
These direct you to the correct management of the patient
1.What are the 2 fundamental reasons patients seek the services of a physician?
Correct diagnosis and intervention.
1.Where in VICTANE is radicular pain classified?
It is in more than one of the categories. It could be neoplasia, trauma, ect…
Sources of secondary gain:
Muachausen syndrome: patient creates a fable related to their particular disorder.
Muachausen by proxy: Parents who claim child is sick to gain attention.
Monday, September 15, 1997:
Differential Diagnosis: A Strategic Approach
1.Data Acquisition
Includes all information obtained from the patient encounter.
Data should be recorded in the form of a chart
Use interrogatory approach. You must ask the correct question. Also, look not so much at what they say but
how they say it.
As you, get better you will feel more than you think while obtaining the patient history.
Purpose of history taking is to get data and determine if the patient is going to be cooperative. You must
formulate how you are going to teach this patient as a student. Intellect, communication skills, education,
interest ect.. are all-important factors that are felt heart to heart as well.
PHYSICAL EXAMINATION:
Health inventory of the patient.
Look for signs
2.Analysis of Positive Findings
Prioritize positive findings.
3.Systems Assignment
Can be very broad in regards to systems or a very specific finding. (Vertigo vs. Fracture)
4.Differential Category
VICTANE
Positive SLR is typically associated with arthritide. Neoplasm could also be associated with positive SLR.
Trauma or metabolic disorders could be responsible for a positive SLR.
5.Differential Diagnosis
6.Testing Strategy
Take hypothesis and scrutinize it with expensive tests.
Laboratory Diagnosis, cultures, CBC, Chemistry, diagnostic imaging and physiological tests such as EKG,
EMC, NCV. Defensive testing is common to avoid malpractice suites. 20% of all testing in this country is
defensive testing.
Testing strategy reduced the differential diagnosis to the working diagnosis
7.Diagnosis
8.Treatment
Restoration of function and reduction of pain
The hard but important part of treatment is the prevention:
PREVENTION:
1.Primary prevention:
Focuses on risk factors and the elimination of risk factors.
Reversible and non-reversible risk factors. Age and gender are non-reversible risk factors.
Reversible risk factors for coronary artery disease could be blood pressure, exercise levels, diet,
stress and coping strategy.
Risk factors, which are normalized, are primary prevention factors.
Keep risk factor from getting established
2.Secondary prevention:
Reducing the established risk factor.
Reduce impact and duration
3.Tertiary prevention:
Risk factors have evolved into natural history, your goal is to reduce more aggressively than ever the
rehabilitation tactics.
The disease is in position to kill the patient but you use coronary rehabilitation to help out he patient.
This cycle is circular.
Wednesday, September 17, 1997:
Dr. Kettner in Denver:
Monday, September 22, 1997:
MIC-KIBIC at the Karolinska Institute: Hematology material. http://www.mic.ki.se/Diseases/c15.html
Data Acquisition
Chief complaint
Onset
Temporal: (differential value)
Chronic, subchronic, acute
Most rapid evolving disorder of a patient is in the vascular or nervous system
CVA: clot forms in a matter of seconds and in an instant the brain is Ischemic and the patient crashed very quickly.
Lengthy evolution of a diagnosis would be 10 years of shoulder pain due to arthritide. Osteoarthritis
Rapid loss of function minus pain is target within the vascular system within the brain.
Qualitative:
Insidious:
Abrupt:
Provocative (Most powerful constituent of chief complaint)
Must probe patient to find out what is really going on
If chief complaint cannot be provoked, it is not NMS condition
Vascular system frequently changes with provocative and palliative due to demand
Provocative feature in case study was rotatory adjusting
Palliative (Most powerful constituent of chief complaint)
If chief complaint cannot be palliative, it is not NMS condition
Palliation in case study was bending
Quality
Type of pain
Neural structure pain is sharp and shooting, somatic or muscular structures are dull and achy.
Radiation
Radiation from chest upward would be neurovascular.
Pat attention to radiating dermatomal pain. If it alternates, they should be imaged immediately. Could be neoplasia, MS, ect.
Severity/Site
Analog scale
Functional deficit. What is patient unable to do because of their chef complaint.
Acute recognition of pain is the lateral spinothalamic tract. Very fast pain processing.
Chronic pain sufferers remember their pain and remind themselves they are always in pain. People in chronic pain need to focus
on improvement of function and attitude, you should not focus on their pain.
Must know you if you have a tough, stoic person or a fragile person
Allodynia: crossed circuits. Mechanoreceptive activity short-circuits with nociceptive activity.
RSDS patients benefit the most from physical activity.
Timing
Friday, September 26, 1997:
Analysis
Priority
Probability
Prevalence
Pedantry
Categories
Vascular
Infection/Inflammation
Congenital
Trauma
Arthritide: most of the patients will be in this category along with trauma.
Neoplasm
Endocrine
Arthritide
Degenerative
Hypermobility
Instability
Disc herniation
Spinal stenosis
Myofascial pain
Tendonitis
Rostrocaudal subluxation: alteration of facet surfaces due to disc degeneration.
Infection/inflammatory
Metabolic
KNOW THIS CHART: In the handout
Monday, September 29, 1997:
Go over case study we did for extra credit.
DIFFERENTIAL DIAGNOSIS OF BLEEDING DISORDERS: (These overheads are in our folder)
1.Bleeding caused by vascular defects; purpura without significant hemorrhage arising from conditions or substances damaging the
vessel wall or endothelium.
A.scurvy
B.infections
C.Cushing’s (protein wasting)
D.simple/senile purpura (elevating estrogen)
E.multiple myeloma
F.Marfan’s disease
2.Bleeding caused by thrombocytopenia ; spontaneous bleeding results from platelet counts less than 20,000/ul; platelet deficiency arises from impaired production, increased rate of destruction, distorted distribution or dilution (excess intravascular volume)
A.chemicals
B.myeloproliferative neoplasm
C.infection
D.immune thrombocytopenic purpura
E.disseminated intravascular coagulation
F.aplenic sequestration
3.Bleeding caused by defective platelet function
A.congenital
B.acquired (alcoholism ect…)
4.Bleeding caused by coagulation protein defects ; results from the deficiency or dysfunction of one or more plasma glycoproteins
essential for coagulation or antibodies preventing normal protein interactions (inhibitors)
A.Factor VII deficiency
B.Factor VIII deficiency
B.
C.
5.Bleed associated with fibrinolytic system plasminogen-plasmin enzyme system may be excessive resulting in recurrent bleeding
KEY CLINICAL POINTS
Prolonged bleeding or at unusual sites (gingiva, GI, retroperitoneum)
Flowchart in text about the intrinsic, extrinsic and common pathways.
Read handout article about anemias for the next class period.
Wednesday, October 01, 1997:
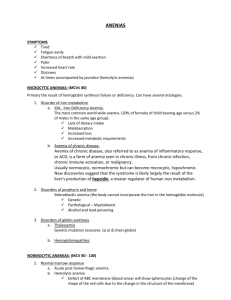
Talk about article from class last week: A FRAMEWORK FOR DIAGNOSING ANEMIA:
Vascular dementia is when anemias put holes in the brain or something.
Coronary artery becomes symptomatic when there is a 75% luminal reduction.
Even with less than 75% reduction you will have symptoms if hematocrit drops below _______
Athelerosclerotic disease can lower renal function because there is not as much pressure in the kidney as there once was.
Tubular system may be damaged
There are many systems dependent upon sufficient vascular tension.
If the onset of anemia is gradual, a normal individual can tolerate a 50% fall in hemoglobin with only minimal symptoms.
The most useful tests to confirm the diagnosis of iron deficiency are for serum iron and total iron binding capacity (TIBC) These are follow up tests.
Study this Stuff with KENDRA. Notes In red and white folder
64 year old male complaining of fatigue do CBC reticulocyte levels increased decreased MCV,MCHC hypochromic, Microcytic anemia pt. Is an alcoholic.
Do serum iron and TIBC
Serum iron returns decreased. Blood loss so check the GI, GU
Do hemmocult x3 to test GI blood loss
UA to determine GU blood loss
Look at test protocol on back of article.
Pt not given iron because you don’t know where blood loss is and you take care of the problem.
Physiological consequences
At 9000 feet a prompt response by the bone marrow.
Marrow makes reticulocytosis and get very many new RBC’s
Erythropoeitin comes from kidneys
Friday, October 03, 1997: GET NOTES FROM GARZONE!!!
Flow chart on the back of the notes. Page 4
Cyanocobalamine is the messenger for informational content molecules is dependent upon B12 for transportation.
Must look at these three forms with looking at any nutritional problems:
B12 deficiency comes in three forms. (Macrocytosis)
1.Decreased intake
Do nothing but drink alcohol and all B vitamins are used up.
Vegan diet not done properly.
2.Decreased absorption
3.Increased utilization.
Monday, October 06, 1997:
Pernicious anemia is an example of auto antibody response.
Results in no absorption and gastric lining is flat and smooth.
Myeloproliferative disorder
Lymphoma, leukemia and multiple myeloma (most common primary malignancy of the skeleton)
Myeloma cell type is an intermediate form of lymphocyte. Plasma cells explode in the marrow.
Myeloma occurs in hematopoietic cells (in long bones, pelvis, vertebrae, skull, shoulders) and present with pain in these locations.
Schilling test confirms this
Normochromic Normocytic
Before the age of 35 you produce more bone than you take away.
This is how we grow in developmental principal
At age 35 we are at equilibrium
After age 35 you loose more bone than you make (osteoporosis)
RBC count is low. Cell size is normal, hemoglobin content is normal.
Degeneration
RBC:
Without a nucleus they are subject to the forces of entropy. Membrane flexibility characteristic at about 90 days.
1/120th of RBC count is being reproduced every day.
Precursor to RBC is reticulocyte. .5-1.5% RBC is reticulocyte.
WHEN RBC is reduced, your reticulocyte count should go up to replace RBC.
In underproduction, reticulocyte count does not go up. Causes include malignancy and refractory anemia (not understood).
Bankrupt
Marrow and Get Underproduction.
Entities in underproduction include myelphthisic anemia. This means marrow is crowded probably due to neoplasm. Don’t have enough room to make RBC
Myelo means marrow and cord.
Aplastic Anemia is the cessation of growth in the marrow. You stop making marrow. These patients are usually pre-leukemia
Refractory anemia: these are terminal patients.
WBC
Platelets
Underproduction are the most threatening forms of anemia
Increased Red Cell Destruction Anemias
Acquired hemolytic anemias: splenomegally is most common
Differentiates underproduction from hemolysis comes from reticulocyte count.
Wednesday, October 08, 1997:
Write a case for class on Monday. Just one paragraph, it should only take a half an hour.
Use CBC in this case study.
Don’t use reference material outside of the course. Center it around the handouts we have been given.
Go over article HAEMATOLOGICAL PARAMETERS
Performance Characteristics: how well do these tests work.
Missed Class October 9,1997 to October 17, 1997:
Monday, October 20, 1997:
WBC infection does not occur after 40,000. You are dead.
Sepsis is low white count. It goes way up and then comes back down.
65,800 WBC means marrow is abnormal across all cell lines. Neoplasm should be considered. Neoplasm’s are associated with
hyperproliferative cell response.
Leukemia is a consideration of WBC over 45,000
Dysplasia is second choice for WBC this high. Myelodysplasia (dysplasia of marrow) disordered cell growth but not neoplastic.
Many times dysplastic patients become neoplastic.
Bands elevated
Immature
Lymphocytes:
Monocytes: one over at 9 (0-8)
White cell line shows marked leukocytosis with a differential shifted to left with elevated neutrophyls, elevated band elevated basophil.
Platelet shows marked increased (2nd cell line)
Thrombocytosis or thrombocythemia.
RBC: High
Hematocrit: high
Hemoglobin: High
MCV: Low
ESR: 0
Myelocytes in peripheral stream means almost all the time the person is neoplastic.
Myelocyte is an immature cell
Metamyelocytes and myelocytes are from the white cell line.
Eleveation of red count is polycythemia,. Cannot have this and anemia at the same time.
Secondary polycythemia
Has a definable etiology
Associated with cardiopulmonary disorder
COPD: emphysemia, Asthma, cystic fibrosis
Causes secondary polycythemia because they impair oxygen into the body
These people are hypoxic.
Hypoxia activates renal erythropoietin production
Platelets normal and White count differential is normal.
Leading cause of elevation in hemogram is lung disease. This is very common entity.
Cardiopulmonary disorders activate increase erythpoitein and produces polycytheia.
If you go to veil at a higher altitude you would have altitude impact on density of oxygen.
Cannot find oxygen there so you would make more RBC and increase your polycythemia.
At about 9000 feet you start more erythpoietic activity.
People with COPD cannot go to these altitudes cannot go to these altitudes.
Wednesday, October 22, 1997:
Polycythemia Vera was a case study
Red count rockets through upper end, elevated HCT, HGB do not give thought to anemia.
Primary and secondary polycythemia.
Target cells go with thalassemia.
Electrophoresis to rule out thalassemia.
MEMORIZE THIS AND IT WILL HELP:
CBC provides diagnosis such as
White cell line
1.Infection
Bacterial, viral
2.Neoplasm
Leukemia, myeloma would be lucky guesses.
3.Platelets
Causes of thrombocytopenia (autoimmune platelet deficiencies) idiopathic
Elevation would be neoplase
Reduction would be radiation, steriods, IPT
4.RBC
1.Anemia
2.Polycythemia
Monday, October 27, 1997:
Start Class with another case study:
Anemia
An infection that happens so quickly that there is hardly time to recover is intercurrent infections
Upper respiratory infections should not happen more than three to four times per year. If you have them more than that you are
probably overstressed.
Manifestations of thrombocytopenia is a spontaneous bleeding
Cutaneous manifestations from pettechia and purpura
When count gets below 20,000 platelets, they spontaneously hemorrhage. They are then battling for their life.
Thrombocytopenia is a life threatening syndrome.
What raises platelets? Neoplasm is often responsible for elevation of platelets.
Extremes are associated with neoplasm.
As soon as you see blast you can assume these cells have exploded.
Wednesday, October 29, 1997:
Review for exam:
22.Thrombocytopenia increases the risk of:
A.Polycythemia
B.Thrombosis
C.Anemia
D.Hemorrhage
22.Reticulocytosis that is accompanied by normochromic normocytic anemia is associated with:
A.Renal failure
B.Hypothyroidism
C.Aplastic anemia
D.Hypersplenism
22.Or the previous answers listed in question number twenty-two (22), which is the leading cause of acquired hemolytic anemia:
A.Renal failure
B.Hypothyroidism
C.Aplastic anemia
D.Hypersplenism
Look at more case studies.
When immature cells are present in the morphology think of neoplasm.
Can have schitzoid shift. Pt. Started with red cell count but now the white count is elevated with the bands. This picture is mixed with marked number or atypical lymphocytes
Bands are immature neutrophils but not immature enough to be considered Neoplastic..
This is CBC on mono delayed by a week.
Left shift means infection or inflammation is present
Right shift is when white is low or normal. Lymphocytes are elevated. Lymphocytosis and allopeia. Typically viral or bacterial.