Group5 - OpenWetWare
advertisement

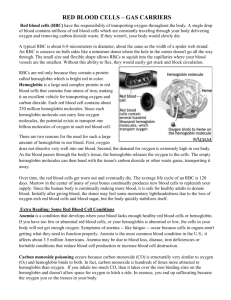
Bacto-Blood: A Bacterial Blood Substitute Austin Day, Josh Kittleson, and Lane Weaver Abstract Surgeries, severe injuries, chronic diseases, and a host of other conditions generate a strong demand for blood transfusions worldwide. However, the current system of relying on blood donations is fraught with difficulties, including a fluctuating supply, potential contamination, and high expense. In developing countries, these problems are particularly exacerbated, creating an environment where lives are needlessly lost due to insufficient blood supplies. Although a range of blood substitutes are currently being developed, none has emerged as a clear winner. To fill this vacuum, and to develop a platform for additional therapeutic applications, we propose using E. coli expressing human hemoglobin as a blood substitute. Although this approach faces a variety of unique challenges, each can be overcome to ultimately yield a limitless supply of blood substitute. Sufficient oxygen transporting capacity will be established by controlled expression of both hemoglobin subunits, supported by a small array of auxiliary proteins. Aversion of a fatal septic response to injected bacteria will be accomplished by altering the structure of the offending molecule, while immune system clearance will be ameliorated by encapsulation in a thick layer of polysaccharide. Converting the cells into passive oxygen carriers, either through destruction of their DNA or direct suppression of their ability to replicate, will prevent unintended infection. Finally, the shelf life of transfusion-ready cells will be extended through exploration of traditional preservation methods such as desiccation. Ultimately, the developed bacteria will be tested in animal models to provide confidence that they will function as designed in their final target, the human blood stream. Although the process of taking this concept from mere idea to clinical reality could take many years, a prototype may be developed in just a few months. Progress in this arena promises not only to aid millions of people, but also to drive our understanding of bacterial systems, the human immune response, and the role of erythrocytes forward in the years to come. Part I: Motivation and Goal Motivation The global demand and importance for cheap, available, and disease free blood substitutes is undisputed. Battlefield trauma, road traffic accidents, and blood loss during surgery all currently require blood transfusions for successful treatment. However, there are currently no red blood cell substitutes approved for clinical use in the US or the UK and whole blood is almost always in short supply. 1 The global collection of blood per year is approximately 81 million units. However, only 27 million of these units are collected in low and medium income countries where 82% of the world’s population lives. 2 The frequency of blood donation in such underdeveloped countries has been reported to be less than 1% of the entire population. 3 To complicate matters even more, a significant portion of that population are disease carriers. As a result, cheap, effective red blood substitutes will provide the most benefit to the populations of developing nations. The reality of the situation is that inexpensive blood substitutes, even those that don’t meet the safety standards of blood substitutes in the US and the UK, will allow patients to receive treatments ordinarily requiring blood transfusion, and could dramatically improve the health in many developing countries. 4 Blood shortages are frequently reported even in the developed world and are due primarily to the unpredictable nature of emergency situations, as well as the inconsistent frequency of blood donors due to seasonal variation, holidays, and religious festivals. 5 To make matters worse, donated red blood cells only have a shelf life of about 35 days. 6 The health of the developed world can be improved by the introduction of a safe blood substitute as well. The optimal transfusion is given to a patient before it is needed. Presently, doctors might exercise restraint in giving patients a transfusion because there are currently no quantitative guidelines for when a transfusion is needed and the doctors must rely on somewhat of a “gut” instinct. Also, blood is expensive, has risks of disease transmission or immune rejection7, and is usually in short supply. If doctors were able to exercise less restraint due to cheaper and safer blood substitutes, that in itself could save lives. 8 Goal The ideal red blood cell substitute must satisfy the following criteria: It must deliver oxygen efficiently. It must cause no undesirable side effects. It must require no compatibility testing. It must remain stable during prolonged storage. It must persist in circulation. It must be easily reconstituted, and it must be available at a reasonable cost. 9 Our project goal is meet all of the criteria for an ideal blood substitute using a hemoglobin producing bacterium as the basis of a red blood cell substitute. By expressing mutant human hemoglobins within E. Coli, we can achieve oxygen transport with similar characteristics to real human red blood cells. The expression of the bacterial K1 capsule and the O16 antigen will help to protect the bacterium from the immune system to increase half life. This capsule combined with a modification to the lipid A component of the lipopolysaccharide (LPS) layer will reduce sepsis, a fatal over-stimulus of inflammatory responses. Such an artificial red blood cell would not require typing, would be relatively inexpensive, and free from the possibility of disease transmission. A red blood cell substitute made from E. Coli would require a bacterial chassis which would not induce sepsis, even at high concentrations. Once this hurdle is overcome, the possibilities of in vivo therapeutic bacteria applications become more realistic. In a sense, a safe bacterial chassis would provide the much needed stepping stone towards more advanced therapeutic bacteria applications. One such application currently being researched is tumor killing bacteria, 10 but other projects such as artificial, fast acting platelets, bacterial sensing, production, and delivery of protein therapeutics, artery cleaning bacteria, toxin eliminating bacteria, and bacterial extensions of the human immune system might follow. One might even envision potential near term applications involving a sepsis free bacterial chassis with enzymes capable of breaking down or sequestering toxins. However, the most immediate applications of a successful artificial blood substitute include not only the obvious ones such as resuscitation and surgery, but also ischemic disease, angioplasty, extracorporeal organ perfusion, cell culture media, hematopoietic stimulation, cardioplegia, sickle-cell anemia, tumor therapy, and chronic anemia. 11 Part II: Background Cell-Free Hemoglobin Blood Substitutes Because of the importance and need for blood transfusions in many situations, there are many different substances currently under research as blood substitutes. Cell free hemoglobin based oxygen carriers are solutions of structurally modified human hemoglobin. The modifications aim to address the problems which occur when you take the hemoglobin outside of the protective environment of the red blood cell. Due to being suspended in solution, hemoglobin based blood substitutes are capable of reaching capillaries that normal red blood cells have a hard time reaching, thus increasing the ability to oxygenate tissues. 12 The hemoglobin is either extracted from animals or produced in E. Coli cultures, and has potential to be readily available. 13 Hemoglobin based substitutes degrade due to autoxidation, but it has also been suggested that hemoglobin based blood substitutes can be stored for up to 36 months.14 The half life of modified hemoglobin has been reported to be around 12-48 hours. 15 The first generation cell free hemoglobin based blood substitutes were riddled with vasoconstriction problems, toxicity issues, oxidative damage issues, and binding affinity mismatching. These problems are all currently being addressed through protein structure engineering. 16 17 18 The primary mechanism thought to account for vasoconstriction is the free hemoglobin binding and scavenging nitric oxide from the nearby environment of the blood vessels. Nitric oxide is a well known stimulant of arterial relaxation. Many types of recombinant hemoglobin mutants are being researched to correct this problem by reducing the hemoglobin’s ability to bind nitric oxide, while leaving the ability to bind oxygen or carbon dioxide intact. 19 Toxicity issues arise due to the alpha and beta subunits of hemoglobin dissociating in dilute solutions, like how they are when suspended in free solutions. The small size of the individual subunits of hemoglobin cause rapid uptake by the renal system and can cause long term damage to the kidneys. Current research has concentrated on cross linking the alpha and beta subunits of hemoglobin to decrease their dissociation, and thus reduce their toxicity. 20 The oxidative damage caused by cell free hemoglobin blood substitutes is due to autoxidation. 21 Hemoglobin, when outside its protective environment, undergoes unhindered oxidation of its iron center. Spontaneous oxidation of the ferrous/oxy derivative (HbFe2+) leads to non-functional ferric heme (HbFe3+) and a superoxide ion (O2*), which subsequently dismutates to generate hydrogen peroxide, which can damage the protein and/or the heme group itself. 22 There have been attempts to remedy this issue either by conjugating antioxidant enzymes such as catalase and superoxide dismutase onto the hemoglobin23, or to create mutants with inherently lower ability to autoxidize. 24 Because there are no free hemoglobin based blood substitutes currently on the market, 25 the cost of them can’t be accurately determined. However, Robert Winslow, a prominent figure among artificial blood substitutes field mentioned in his book that the cost of hemoglobin based oxygen carriers is “probably high.” 26 Encapsulated Hemoglobin Another potential blood substitute involves encapsulating free hemoglobin within liposomes. Liposomes are synthetic lipid derivatives of poly(ethylene glycol) (PEG) which are used to encapsulate high concentrations of mutant hemoglobin. The idea behind encapsulation is that it would help to separate the hemoglobin from the environment, similar to the function of a real erythrocyte membrane, and would thus prevent dissociation of hemoglobin dimers and the subsequent renal toxicity. They are considered the closest technology to creating artificial red blood cells. These liposomes come in a range of sizes from less than 60nm to greater than 200nm. 27 Due to the small size of these liposomes, they also can reach areas of the circulation that red blood cells may have a hard time reaching, and similarly to cell free hemoglobin, they may also enhance oxygen transport. The size of the liposome greatly determines its half life. The ideal liposome would be as large as possible, while still retaining a PEG-mediated prolonged circulation half life. By using charged lipids, researchers can enhance the encapsulation efficiency; however, by doing this, they may be encouraging undesirable interactions with other circulating proteins which can cause their rapid uptake by the reticulendothelial system (RES). 28 There have been a few problems with toxicity issues as well, involving pulmonary hypertension and other hypersensitivity reactions. 29 The manufacturing technologies which create these encapsulations are currently high cost and have difficulties in producing consistently sized particles. 30 This lack of large scale production technology is the primary downfall of encapsulated hemoglobin. The liposome encapsulation has been proven to be devoid of the vasoconstrictive effects that are commonly seen with cell free hemoglobin substitutes. 31 Researchers have obtained concentrations greater than 36g/dl within these liposome encapsulations. This is significant compared to regular adult plasma, which contains approximately 15 g/dl.32 This artificial membrane also provides the potential to co-encapsulate allosteric modifiers and antioxidants, to even more closely mimic a red blood cell in oxygen binding affinity, as well as repression of reactive oxygen species. 33 The half life of the liposome particles has been estimated to be about 42 hours34 and the shelf life estimated to be about 3-6 months. 35 Perfluorocarbon Emulsions The most advanced, non-hemoglobin based blood substitutes are perfluorocarbon emulsions. Perfluorocarbons are basically hydrocarbons with fluorine atoms in place of hydrogens. They are chemically inert and appear as a clear liquid that readily dissolves many gases, including oxygen and carbon dioxide. 36 Because these perfluorocarbons are immiscible with water, they are emulsified using egg phospholipids. These perfluorocarbon products are the most advanced in terms of FDA approval. OxygentTM, made by Alliance Pharmaceuticals Corp, is already FDA approved and is being used with a combination of volume expanders and hemoglobin based substitutes on a small scale. 37 The safety profiles of such perfluorocarbon emulsions aren’t published in the scientific literature, but they form the basis to allow for clinical testing. 38 Perfluorocarbon emulsions currently have no known metabolism in the human body and are cleared through exhalation by the lungs or taken up by the reticuloendothelial system. 39 40 41 With droplet sizes of less than .2 µm 42, perfluorocarbon emulsions also show the same enhanced oxygen transport over red blood cells as free hemoglobin and liposome encapsulated blood substitutes do. 43 However, the gases aren’t bound to the perfluorocarbon chains like how they are in hemoglobin. Gases are simply dissolved loosely in the liquid. An important benefit arises because of this property. Perfluorocarbons have been shown to augment local oxygen delivery much more than would be expected from the increase in oxygen content in arterial blood. 44 The oxygen in the perfluorocarbons is taken up preferentially over bound oxygen in hemoglobin based blood substitutes or even natural red blood cells. The primary issue with perfluorocarbon emulsions is that the oxygen dissociation curve is linear, as opposed to the sigmoidal curve seen for hemoglobin. Figure 1: 45 Oxygen dissociation curves for cell-free hemoglobin and for the perfluorocarbon emulsion OxygentTM. The linear curve of the perfluorocarbons is due to gases dissolving into the solution, as opposed to being bound to a molecule. For any given partial pressure, hemoglobin will have higher oxygen content than perfluorocarbon emulsions. This linear oxygen dissociation curve for perfluorocarbons results in lower oxygen capacities than hemoglobin based substitutes. The half life of these perfluorocarbon emulsions are also shorter than the ideal blood substitute, being about 9.4 hours. 46 However, it should also be noted that due to their small sizes, it may take up to 2 years to fully clear the particles from the system. Whole Blood The most widely used substance for transfusion and resuscitation is still donated human blood. The obvious benefit of whole blood transfusions is that you are replacing lost blood with real blood, so there are not worries with oxygen binding affinities or toxicity. If you plan an autologous transfusion for a planned surgery, the success rate is very good. But more often, one must rely on donated blood, which introduces many possible complications. There are many things to consider when using donated blood. In developed countries, there are many safeguards in place to prevent disease transmission. There is sensitive screening prior to recruitment, disease testing, and post-donation product quarantine. But even with these safeguards, disease transmission may still occur due to human error or inadequate testing. Also, in developing countries, these safeguards aren’t financially practical. Globally, over 13 million blood donations are not tested for human immunodeficiency virus, hepatitis B, or hepatitis C, 47 and 39 countries reported issuing some blood and blood components without testing for transfusion-transmissible infections, owing to interruptions to supplies of test kits. 48 Disease testing procedures, along with pre-donation information literature, deferral procedures, and donor tracing, notification when instances of disease transmission are detected, storage, and shortages greatly increase the cost of whole blood. The cost of a single unit of whole blood is approximately $373. 49 With specialized procedures, the cost can reach upwards of $500 a unit. Immune rejection is also a notable risk with blood transfusions. Human error in serotype choice is responsible for 2.2% of all fatal transfusion reactions. 50 There have been successes in blood type conversion technology recently by using bacterial glycosidases to cleave the A and B antigens from erythrocytes.51 This is an important advance because hospitals still only allow the use of blood type O in emergency situations. If the possibility of disease transmission, immune rejection, and a high cost wasn’t enough, there is also the reality that red blood cells have a shelf life of about 35 days, and rely on regular donation to ensure an adequate supply. 52 Bacterial Blood Substitute After considering the competition, a bacteria blood substitute introduces a different set of problems for a blood substitute, the main issues being the half life and control of sepsis. Even though these are limiting issues, they are unique limits in the artificial blood field and provide another route by which an artificial blood substitute may be developed. The remainder of the proposal will cover the details and planning involved in building a bacterial blood substitute from a typical lab strain of bacteria. Part III: Hemoglobin Expression The first step in achieving a bacterial blood substitute is the expression of an oxygen carrier within the bacterium. There are a few issues to consider when choosing an oxygen carrier. Adult human hemoglobin seems like the most likely candidate because it was made for this purpose, but free hemoglobin has a significantly lower p50 value (partial pressure of oxygen at which 50% of the hemoglobin is saturated) than erythrocytes, primarily due to the absence of an allosteric modifier, 2,3diphosphoglycerate (DPG). 53 It was reported that the p50 is directly proportional to the amount of delivered oxygen. A p50 value which is too low will not deliver sufficient oxygen. There are two promising solutions to this problem. The first solution is to simply express the eukaryotic enzyme, DPG mutase, in the bacterium so that it can create the missing 2,3-DPG from the glycolysis pathway and hopefully correct the p50 value an appreciable amount. This enzyme has already been expressed in E. coli, making this a possibly quick solution. 54 Another way around this problem may be by the introduction of mutations within the globin subunits themselves. There are various mutations in the literature that increase p50, decrease auto-oxidation rates, and increase tetramer stability. One mutation is termed a “Presbyterian mutation”, and involves the change of Asn-108 Lys in the β-subunit of hemoglobin. It was reported to create a mutant with decreased oxygen binding affinity (increased p50) to a level comparable to that of native hemoglobin bound to DPG in erythrocytes. 55 Chien Ho came across a set of mutations capable of reducing the auto-oxidation of hemoglobin as well as increasing the p50. 56 Another issue is the level of soluble hemoglobin expression. The highest reported amount of soluble hemoglobin expressed in E. coli found was .64g/dL.57 This is significantly different than the ~15g/dL found in human blood. 58 The .64g/dL amount was expressed in the present of three fold molar excess of heme, on a high copy number plasmid, and used E. coli codon optimized synthetic hemoglobin genes. It should be noted that in addition to the soluble hemoglobin, there was twice as much insoluble hemoglobin produced. This may suggest room for improvement. We suggest a few tricks that may be attempted to improve this estimate. One method may be to increase the heme production from the endogenous biosynthetic pathway. 59 This may seem redundant due to the excess of heme outside of the cell, but it has been suggested that the hemoglobin subunits are stabilized by the insertion of heme, and if the uptake of heme by the cell were limiting in any way, it may cause less soluble protein to form. 60 61 It is mentioned that the alpha subunit of hemoglobin is unstable on its own in solution and needs to either be incorporated quickly into a tetrameric hemoglobin, or it will aggregate and precipitate. To aid in the proper folding of these subunits, coexpression of the alpha and beta subunits on the same cistron has been shown to improve yield. 62 Another issue to consider is the presence of the extra N-terminal methionine residue due to the protein being expressed in E. Coli. This extra residue affects the binding affinity of the hemoglobin and changes its final conformation. 63 64 65 This may be significant not only because it affects the oxygen binding affinity, but also because it might be hindering the solubility of the protein, decreasing its yield. To correct this problem, the genes for E. Coli methionine aminopeptidase (Met-AP) can be overexpressed, which will cleave the extra methionine residue. 66 There also may be an issue with auto-oxidation of our heme centers. It is hard to predict the rate of auto-oxidation of the hemoglobin mutants we want to use, but there will most likely be some significant amount of auto-oxidation. It is most likely sufficient to simply express the natural erythrocyte anti-oxidant enzymes catalase, superoxide dismutase, and possibly a methemoglobin reductase enzyme, to prevent damage to the heme centers of our hemoglobin. We suspect that other factors which haven’t been extensively studied, such as the expression rates, temperature, various other combinations of mutations, and the presence of stabilizing chaperone proteins67 may also play important roles in the expression level of soluble hemoglobin and may provide possible routes for future exploration. However, the system we suggest for an initial trial would include a vector that co-expresses the alpha and beta mutant human hemoglobin A, methionine aminopeptidase, catalase, superoxide dismutase, methemoglobin reductase, AHSP (alpha Hb stabilizing protein), and extra genes that encode for bottleneck molecules in the heme biosynthetic pathway. Part IV: Bacterial Chassis The first challenge for deliberate introduction of hemoglobin totting bacteria into the bloodstream is development of a bacterial coat that minimizes immune response, clearance rate, and risk of opportunistic infection. One of the primary concerns of delivering a high load of bacteria intravenously is causing sepsis, which is an often fatal overreaction of the immune system to bacteria and bacterial components68. In order to be useful as a blood substitute, the bacteria need to remain in circulation for at least several hours69. However, a normal immune system is capable of clearing the vast majority (>90%) of bacteria in under an hour70. While immune response suppression may mitigate both of these concerns, significantly weakening a patient’s immune defense for hours or days risks opportunistic infection. Fortunately, the synthetic biology approach offers a way to navigate these challenges: selection of an appropriate chassis, removal or alteration of known surface antigens, and addition of a protective covering should do the trick. Selection of a Chassis When considering what bacterial coat to use in a blood substitute, the first major question to explore is whether gram positive or gram negative bacteria make more sense. As illustrated in figure 2, there are several gross morphological differences between the two types of bacteria. Where gram positive bacteria have an inner membrane surrounded by a thick outer cell wall composed of petidoglycans, gram negative bacteria have an inner membrane, a thin layer of peptidoglycan, and an outer membrane sporting an asymmetric inner and outer leaflet. Both types of bacteria may further have an outer coating, called a capsule. A rough measure of the relative ability of each type of bacteria to survive in the blood can be garnered from the fact that the majority of bacteremia is caused by gram positive bacteria71. However, they are also the leading cause of sepsis72. Thus, a more detailed biochemical analysis of each cell type in the context of the immune system is needed to determine which of the two provides a better option. Figure 273 Differences between gram negative and gram positive cell envelope. An in-depth examination of how gram positive bacteria survive so well in our blood reveals a multi-faceted defense system. Group A Streptococcus inhibits macrophage recruitment, blocks opsonization (biochemical labeling by the immune system), prevents phagocytosis, resists phagocytotic killing mechanisms, and kills macrophages74. Because the goal is to minimize the negative impact on the immune system of injecting bacteria, only relatively unaggressive mechanisms associated with the cell surface would be of use. Of the listed mechanisms, only a few are a consequence of the cell surface and surface associate proteins: a hyaluronic acid capsule and a protein called protein M that inhibits opsonization. Similarly, Staphylococcus aureus employs a broad range of strategies to avoid the immune system75. Those relevant to the cell surface are a protein (protein A) that blocks specific antibodies, a protein (ClfA) that blocks opsonization by binding fibrinogen, and several modifications to the cell envelope structure that make it resistant to both anti-microbial peptides and lysozyme. However, in all of these cases, the peptidoglycan structure of the cell wall is left largely unaffected. Since a critical component of the cell wall, lipotechoic acid, is recognized by a Toll-like receptor, all gram positive bacteria are potent activators of sepsis76. Thus it seems difficult to justify the use of gram positive bacteria. Gram negative bacteria similarly rely on a capsule for protection, as well as a variety of secreted proteins77. Also like gram positive bacteria, a core component of the cell envelope, lipopolysaccharide (LPS, also known as endotoxin), induces a strong immune system response, potentially leading to sepsis78. However, unlike in gram positive bacteria, methods for reducing the toxicity of LPS have been described79. Exploitation of this (and other) discoveries will be described in further detail below. Given that gram-negative bacteria are a better choice for synthetic blood, the question of what specific organism to use remains. Because of its loss of undesirable virulence factors, ease of growth and manipulation, and well studied genetics, everyone’s favorite lab strain of E. coli (E. coli K-12 MG1655) presents a very reason choice. Removal of Remaining Unwanted Structures Although lab strains of E. coli generally lack virulence factors, they are still capable of creating structures that can contribute to virulence and be recognized by the immune system. Specifically, they can create fimbriae (pili) and flagella80,81. Because fimbriae are involved in adhesion and localization and flagella are involved in motility, and ideally a blood substitute would neither stick to anything nor move of its own accord, it seems to make sense to knock out the genes responsible in the E coli chassis being developed. The fimbriae of E. coli have been extremely well studied, and as such, the genes responsible for both their structure and formation have been identified82. Deletion of all of the fim genes will be accomplished by well-established genomic deletion methods83,84,85. The flagella of E. coli have also been extensively studied, and the structural and regulatory genes involved identified86. Rather than attempting to remove all of the genes involved, deletion of the master activators of the flagellum, flhD and flhC87, by standard methods will ensure that no flagella are expressed. Reducing Sepsis by Altering Lipid A Biosynthesis Septic shock, as noted above, is a frequently deadly overreaction of the immune system to components of a pathogen. The routes of activation of septic shock have been extensively studied88,89, and in the case of gram negative bacteria, the lipid A moiety of lipopolysaccharide (see Figure 3) is the primary bioactive component responsible for causing sepsis90. However, several alterations to the canonical lipid A structure have been identified that reduce the toxicity of lipid A. In experiments using multiple indicators of septic shock, Zhang and coworkers demonstrated that synthetic lipids with modifications such as shorter lipid chains, modified phosphorylation patterns, and added palmitoyl groups had toxicities reduced by as much as 1000-fold91. It has also been noted that underacylated lipid A molecules only have about 1% the toxicity of the canonical structure in both in vivo and in vitro models92. Enzymes responsible for these types of modifications have been identified in natural pathogens and commensal bacteria. In Salmonella typhimurium, PagL and PagP are responsible for removing one acyl chain and adding a different palmitoyl group, as illustrated in figure 4. These changes result in a roughly 100 fold decrease in toxicity93. In E. coli, a mutant was identified with a nonfunctional msbB gene, which was incapable of adding one of the acyl groups to lipid A. The resulting lipid A precursor, illustrated in figure 5, was originally reported to have a 1,000-10,000 fold reduction in toxicity94. However, further studies more properly characterized both the MsbB mutant lipid A and another under-acylated form of lipid A created by Porphyromonas gingivalis as antagonists of the human response to canonical lipid A, even going so far to suggest their use as a therapeutic95. Finally, recent work has challenged the minimal structure of lipid A needed for bacterial viability. Meredith and coworkers isolated a viable mutant defective in an early part of the lipid A biosynthesis process that resulted in synthesis halting at lipid IVa (see figure 6), which also appears to be an antagonist of the septic response96. Presented with this variety of mechanisms for reducing lipid A toxicity, the most straightforward approach is to simply delete msbB from our chassis. A known complication of the mutation, however, is that it reduces the ability of the bacterium to effectively express a K-capsule97 (discussed in greater detail below). Since some evidence suggests that this is due to problematic assembly of the outer membrane98, two approaches to solving the problem seem viable. First, simple overexpression of the components of the capsule may overcome the assembly difficulty. As that may equally well exacerbate the problem, a second approach is to mutate the gene partly responsible for lipid A transport and assembly, msbA. Such mutations have previously been shown to rescue defects in lipid A assembly because of upstream synthesis mutations, presumably because of a shift in transporter specificity toward the precursor rather than the final lipid A product99. Figure 3100 Basic Structure of Lipopolysaccharide. Figure 4101 Modification of lipid A by Salmonella typhimurium Figure 5102. Lipid A molecule of MsbB E. coli mutant. Figure 6103. Lipid IVa, Precursor to Lipid A lacking 2 acylations and core connections. Reducing Clearance through Encapsulation The initial, rapid clearance of bacteria by the immune system is mediated by the complement system. This component of the immune response relies on multiple pathways to opsonize (chemically label) pathogens, as illustrated in figure 7 104. While the classical complement pathway relies on the presence of pathogen-specific antibodies, both the lectin and alternative pathways are part of the innate immune response and recognize pathogens and particulates non-specifically. Opsonization can lead either to direct killing of cells via a membrane attack complex, or more often, killing by phagocytosis105. Figure 6J106 Three Pathways of Complementation Activation. a The classical pathway triggers through binding of specific antibodies. b The lectin pathway triggers through binding to LPS associated carbohydrates and other surface molecules c The alternative pathway is triggered by non-specific cleavage and adhesion of the C3 protein. Not surprisingly, natural pathogens have evolved a variety of mechanisms for evading opsonization107. The presence of an outer capsule composed of high molecular weight polysaccharides, known as the K capsule (see figure 8), can help evade all three mechanisms of opsonization, and as such, represents a powerful way to prolong the lifetime of bacteria in the bloodstream. More specifically, a variant of the K-capsule known as K-1 has been shown to be particularly effective at resisting complementation108. Because the K-1 capsule contains sialyic acid, a component expressed on the surface of some human cells, it does not induce a strong specific response from the immune system109,110. It also prevents non-specific complementation mechanisms by both hiding underlying cell surface structures and binding to factor H, which interferes with the signaling cascade necessary for effective complementation111. The biosynthesis of K capsules in general, and the K-1 capsule in particular, have been extensively studied112. Figure 9 shows the island needed for K-1 capsule synthesis, which includes 14 genes113. In order to protect the artificial blood cells, our chassis will be altered by insertion of this island of genes into the genome using published techniques114. Should direct manipulation of the entire island prove technically difficult, serial addition of smaller fragments of the island can be used instead. The efficiency of the bacteria at expressing K-capsule can be selected for by using serum to kill those that haven’t developed resistance115. A B Figure 8116 A Cartoon representation of the capsule layer of gram negative bacteria. B Electron micrograph of the actual K1 capsule of E coli. Figure 9117 Genes required for K1 capsule synthesis. Part V: Safety Mechanisms Safety, of course, must play a paramount role in the development of a surrogate E. coli blood cell. To effectively address concerns arising from the introduction of a foreign organism into the blood stream, two strategies are proposed. Strategy I: Genomic Destruction The first strategy entails complete destruction of the E. coli genome, prior to intravenous administration of the substitute blood solution. This provides three benefits: (1) Without any genetic material to pass on to progeny, the cell cannot reproduce, thus eliminating the possibility of unchecked growth; (2) the cell is also unable to acquire mutations which could be passed horizontally (via plasmids) to other cells, abrogating a primary evolutionary mechanism of pathogenesis; and, finally, (3) without the genetic machinery necessary to sense and interact with the environment, the cell is much more likely to play the role of a passive hemoglobin transporter, rather than perturbing the blood environment and possibly inducing an immune response. A simple design is proposed to accomplish this goal, as outlined in Figure 10. Various restriction endonucleases (in this example BamHI, PstI, and EcoRI) are placed under the control of a tightly repressed promoter (e.g. pBAD/pBAD+fim). Thus, the default expression from the promoter will be “off,” and the cell will function normally. However, when induced with arabinose, repression of the promoter will be relieved and the restriction enzymes will be expressed. To assay genomic destruction, we will place several reporter genes (with LVA degradation tags for quick response) throughout the genome. Alternatively (or additionally), we may perform RT-PCR and/or southern blot analysis on several candidate genes. Using these assays, we will build a small library of ribosome binding sites placed upstream of our restriction enzymes to obtain expression levels and subsequent genomic destruction in congruence with timescales relevant to our experiment. Figure 10. Strategy for (measuring) genomic destruction Depending on the results of these experiments, a more radical approach incorporating Deoxyribonucleases (DNase), which indiscriminately cleave phosphodiester linkages in DNA, may need to be employed. However, the structural integrity of a cell (in particular that of its cell wall) in the absence of DNA is somewhat uncertain. A report linking methylglyoxal (a metabolite that induces genomic DNA destruction) production to cell viability118 demonstrated that turbidity of a culture appears to stay constant while its viability decreases (a proxy for genomic destruction), suggesting that cells may stay intact even after their DNA is degraded (see Figure 11). However, it should be noted that this was not the main result of the report and the correlation is far from definitive. Figure 1: Kinetics of growth inhibition and killing by xylose and camp. Open circles: experimental, Squares: control. Even in the presence of DNA, the cell wall is highly dynamic. Cell wall recycling is a well-established phenomenon that is often exploited in antibiotic mechanisms of action. These antibiotics, particularly the -lactams, interfere with cell wall recycling, consequently triggering lysis as a result of osmotic stress. While these antibiotics are only effective in growing cells, it is difficult to predict how the complete loss of genetic control might perturb the complex recycling system. To measure cell-stability, we will induce DNA destruction in a hemoglobinproducing cell via the aforementioned methods and measure structural stability at multiple time points by centrifuging the cells, running the supernatant on an SDS-PAGE gel and staining for heme. Strategy 2: Growth Suppression If there is found to be hemoglobin leakage from cells, an alternative strategy, in which the cells are kept viable, but in a quiescent, or non-growing state, may be pursued. This method has the advantage of utilizing the cells’ natural genetic machinery to keep it structurally intact, but of course suffers from accompanying risks of introducing a viable organism into the body. However, recent studies119 in which cells are administered intravenously to target and destroy tumors, have lent precedent to this approach. Regulator of Cell Division (Rcd) is a small RNA that, when over-expressed in an hns– E. coli strain, causes the cell cycle to arrest, resulting in a stable quiescent state120. Overexpression of Rcd additionally results in an increase in production of plasmid-borne proteins (in some instances constituting as much as 40% of total cellular protein) for up to 10 hours. Morphologically, these cells are non-filamentous, and grow on average to about four times normal E. coli cell length. Thus, overexpression of Rcd results in a large, non-growing, high proteinproducing cell that is stable for many hours, making it an excellent candidate for a surrogate RBC. To create an hns- strain, the -red recombination method can be used. This background strain would be employed for subsequent capsular and LPS modification work. In addition, Rcd will be placed under control of a strongly repressed promoter, such as pCI. When co-transformed with a temperature-sensitive CI repressor protein, this strain can be grown at permissive ambient temperatures (<30C), but will not grow when transferred to the bloodstream (>30C)121. In a therapeutic scenario, these quiescent bacteria would need to be eliminated after the initial period of emergency has passed. While application of externally administered antibiotics would be effective clearance agents, it would be desirable to have a means of control that is specific to the engineered bacteria. CcdB (controller of cell death protein B) is a cytotoxic killer protein that is used in many current cloning strategies to decrease background122. This gene can be controlled by a switch-like system, such as the fim Inversion system, in which there is no leaky expression in the uninduced state123. Part VI: Storage The allure of an E. coli based blood substitute is the easy with which it can be made, transported, and stored, and the low cost of this process. One can envision a scenario where master culture is periodically used to inoculate a preparative culture that will be induced to synthesize hemoglobin and subsequently induced to degrade its DNA. Two alternatives routes of storage prior to administration are then proposed. In the first, the cells may be desiccated or lyophilized. Cell viability has been shown to reach levels up to ~80% after being desiccated for timescales of days to hundreds of years, and industry commonly freeze-dries starter cultures for dairy products124. Additionally, capsular polysaccharides may also aid in desiccation tolerance125. Judging from this viability data, it is likely that intracellular proteins are able to be reversibly dried without major loss of function. The second option would be to centrifuge the preparative culture, resuspend in a volume expander, and store as-is prior to administration. Because the main constituent of the volume expander is albumin, which is stable at room temperature for years126, this solution may be refrigerated or possibly even stored on the shelf. Part VII: In Vivo Testing Following the construction of the requisite E. coli blood cells and several in vitro preliminary tests (oxygen-delivery, immune response), the ability of the cells to act as a blood surrogate will be tested in an in vivo blood stream environment. Protocols from previous studies will be adapted for this purpose. Hemoglobin containing vesicles (HbV) are the most analogous blood substitute to E. coli cells, thus its protocols can be employed for these studies127 128. The E. coli cells will be reconstituted in a human albumin (HSA, 25%) and saline solution to regulate the colloid osmotic pressure similar to that in blood vessels (~40mmHg) Data from Hemoglobin expression studies will be used to match hemoglobin concentrations close to levels observed in the blood (10 g/dL)126. These solutions will then be administered to specified animals (mice, hamsters, and/or rabbits) suffering from hemorrhagic shock127. Cardiac, circulatory, and pulmonary variables will then be measured, including Mean Arterial Pressure (MAP), heart rate, cardiac index, tissue oxygenation, and blood gas concentrations (pO2, pCO2). Part VIII: Timeline Pursuing all of the proposed lines of investigation to the point where a therapeutic product would be ready for use in humans would require a vast amount of time and money. We thus consider instead a timeline for development of a minimal system that demonstrates some of the key characteristics needed for a successful blood substitute, including expression of hemoglobin, protection from the immune system, reduced immune response to lipid A, and possibly stalled growth due to DNA destruction. This minimal system can then be tested in an animal model to suggest what challenges remain insufficiently addressed. Note that the encapsulation work has already been successfully performed by Chris Anderson. Concluding Remarks The proposed project to develop E. coli into a bacterial blood substitute presents a variety of interesting problems. In exploring how to overcome those difficulties, significant inroads will be made into both bacterial systems and mammalian systems, and importantly, their interaction. Should the project be successful, millions of people stand to benefit worldwide, and the future of therapeutic bacteria will be bright indeed. 1 2 3 Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 World Health Organization, Europe ,“Blood safety: a global overview”; Fact Sheet, Copenhagen, 10 June 2005 Leikola, J. (1992) Blood donation. Lancet, 340 (8810), 57. Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 World Health Organization, Europe ,“Blood safety: a global overview”; Fact Sheet, Copenhagen, 10 June 2005 6 World Health Organization, Europe ,“Blood safety: a global overview”; Fact Sheet, Copenhagen, 10 June 2005 7 B.A. Myhre and D. McRuer, “Human error – a significant cause of transfusion mortality”, Transfusion, Vol. 40, pg. 879-885, July 2000. 8 Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 9 Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 4 5 J. Christopher Anderson et al., “Environmentally Controlled Invasion of Cancer Cells by Engineered Bacteria”, J. Mol. Biol., 355, 619-627, 2006. 10 Robert M. Winslow, “Blood Substitutes”, Pg. 115, Academic Press, 2005 Robert M. Winslow, “Blood Substitutes”, Pg. 61, Academic Press, 2005 13 Weickert et al, “A Mutation that improves soluble recombinant hemoglobin accumulation in Escherichia coli in heme excess”, Applied and Environmental Microbiology, P.640-647, Feb. 1999. 14 Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 15 Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 16 Vandegriff et al, “MP4, a new nonvasoactive PEG-Hb conjugate”, Blood components, 2003. 17 Moreira et al, “Effect of Hemopure on the Performance of Ektachem and Hitachi Clinical Analyzers”, Clinical Chemistry, 43, 1790-1792, 1997. 18 Caswell et al, “A novel hemoglobin-based blood substitute protects against myocardial reperfusion injury”, AJP – Heart and Circulatory Physiology, 2004. 19 Winslow et al., “Kinetics of NO and O2 binding to a maleimide poly(ethylene glycol)-conjugated human haemoglobin”, Biochem Journal, 183-189, 2004. 20 Abdu I. Alayash, “Hemoglobin-based blood substitutes: oxygen carriers, pressor agents, or oxidants?”, Nature America, 545-549, Vol 17, June 1999. 21 Christine C. Winterbourn, “Free-Radical Production and Oxidative Reactions of Hemoglobin”, Environmental Health Perspectives, Vol. 61, 321-330, 1985. 22 Robert M. Winslow, “Blood Substitutes”, Pg. 198, Academic Press, 2005 23 Privalle C, Talarico T, KEng T, DeAngelo J, “Pyridoxalated hemoglobin polyoxyethylene: a nitric oxide scavenger with antioxidant activity for the treatment of nitric oxide-induced shock”, Free Radical Biology and Medicine, Vol. 28, Issue 10, Pg. 1507-1517, May 2000. 24 Ho et al., “Recombinant Hemoglobin … Exhibits Low Oxygen Affinity and High Cooperativity Combined with Resistance to Autoxidation”, Biochemistry, 38, 13433-13442, 1999. 25 Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 26 Robert M. Winslow, “Blood Substitutes”, Pg. 116, Academic Press, 2005 27 Robert M. Winslow, “Blood Substitutes”, Pg. 506, Academic Press, 2005 28 Robert M. Winslow, “Blood Substitutes”, Pg. 503, Academic Press, 2005 29 Robert M. Winslow, “Blood Substitutes”, Pg. 507, Academic Press, 2005 30 Robert M. Winslow, “Blood Substitutes”, Pg. 506, Academic Press, 2005 31 Robert M. Winslow, “Blood Substitutes”, Pg. 502, Academic Press, 2005 32 R. M. Winslow, “Current status of blood substitute research: towards a new paradigm”, Journal of Internal Medicine, 253: 508-517, 2003 33 Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 11 12 34 W. T. Phillips, R. W. Klipper, V. D. Awasthi, A. S. Rudolph, R. Cliff, V. Kwasiborski and B. A. Goins, Polyethylene Glycol-Modified Liposome- A Long Circulating Red Cell Substitute”, The Journal of Pharmacology and Experimental Therapeutics Vol. 288, Issue 2, 665-670, February 1999 35 Rudolph AS, Cliff RO., Dry storage of liposome-encapsulated hemoglobin: a blood substitute. Cryobiology. 1990 Dec;27(6):585-90. 36 Jerry E. Squires, “Artificial Blood”, Science, Vol 295, 2002. 37 Alliance Pharmaceuticals, <http://allp.com/Oxygent.htm> 38 Donat R Spahn, “Artificial oxygen carriers: perfluorocarbon emulsions”, Critical Care, Vol 3, No. 5, 1999. 39 Spahn DR, Leone BJ, Reves JG, Pasch T: Cardiovascular and coronary physiology of acute isovolemic hemodilution: a review of nonoxygen-carrying and oxygen-carrying solutions. Anesth Analg 1994; 78:1000–1021. 40 Keipert PE: Perfluorochemical emulsions: future alternatives to transfusion. Blood Subst Princ Meth Prod Clin Trials 1998;2:127–156. 41 Riess JG: Overview of progress in the fluorocarbon approach to in vivo oxygen delivery. Biomater Artif Cells Immobil Biotechnol 1992;20:183–202. Keipert PE, “Perfluorochemical emulsions: future alternatives to transfusion.” Blood Subst. Princ. Meth. Prod. Clin. Trials, 2:127-156, 1998. 43 Hogan MC, Willford DC, Keipert PE, Faithful NS, Wanger PD, “Increased plasma O 2 solubility improves O2 uptake of in situ dog muscle working maximally.” J Appl Physiol, 73: 2470-2475, 1992. 44 Donat R Spahn, “Artificial oxygen carriers: perfluorocarbon emulsions”, Critical Care, Vol 3, No. 5, 1999. 45 Robert M. Winslow, “New Transfusion Strategies: Red Cell Substitutes”, Annual Reviews 50:337-53, 1999. 46 Donat R. Spahn “Blood substitutes Artificial Oxygen carriers :perfluorocarbon emulsions”, Critical Care, 1999 47 Robert M. Winslow, “Blood Substitutes”, Pg. 26, Academic Press, 2005 48 World Health Organization, Europe ,“Blood safety: a global overview”; Fact Sheet, Copenhagen, 10 June 2005 49 Robert M. Winslow, “Blood Substitutes”, Academic Press, 2005 50 B.A. Myhre and D. McRuer, “Human error – a significant cause of transfusion mortality”, Transfusion, Vol. 40, pg. 879-885, July 2000. 51 Liu et al., “Bacterial glycosidases for the production of universal red blood cells”, Nature Biotechnology, April 1, 2007. 52 World Health Organization, Europe ,“Blood safety: a global overview”; Fact Sheet, Copenhagen, 10 June 2005 53 George J. Brewer, “2,3-DPG and Erythrocyte oxygen affinity”, Annual Reviews, 1974. 54 Marie-Cladue Garel, Virginie Joulin, and Michel Cohen-Solal et al., “Human Bisphosphoglycerate Mutase”, The Journal of Biological Chemisty, Vol. 264, No. 32, Nov. 1989. 55 Michael J. Weickert, Maria Pagratis, Richard Blackmore et al., “A Mutation That Improves Soluble Recombinant Hemoglobin Accumulation in Escherichia coli In Heme Excess”, Applied and Environmental Microbiology, p. 640647, Fe. 1999. 56 Seong Tae Jeong, Nancy T. Ho, Michael P. Hendrich, and Chien Ho, “Recombinant Hemoglobin (α29Leucine -> Phenylalanine, α96Valine -> Tryptophan, β108Asparagine -> Lysine) Exhibits Low Oxygen Affinity and High Cooperativity Combined with Resistance to Autoxidation”, Biochemistry, 38, 13433-13442, 1999 57 Michael J. Weickert, Maria Pagratis, Richard Blackmore et al., “A Mutation That Improves Soluble Recombinant Hemoglobin Accumulation in Escherichia coli In Heme Excess”, Applied and Environmental Microbiology, p. 640647, Fe. 1999. 58 R. M. Winslow, “Current status of blood substitute research: towards a new paradigm”, Journal of Internal Medicine, 253: 508-517, 2003 59 Seok Joon Kwon, Arjo L. de Boer, Claduia Schmidt-Dannert, “High-Level Production of Porphyrins in Metabolically Engineered Escherichia coli: Systematic Extension of a Pathway Assembled from Overexpressed Genes Involved in Heme Biosynthesis”, Applied and Environmental Microbiology, Aug. 2003 60 Vasudevan G., McDonald M.J, “Ordered Heme Binding Ensures the Assembly of Fully Functional Hemoglobin: A Hypothesis”, Current Protein and Peptide Science, Vol. 3 No.4, pp. 461-466, Aug. 2002. 61 Kazuhiko Adachi, Yi Zhao, and Saul Surrey, “Effects of heme addition on formation of stable human globin chains and hemoglobin subunit assembly in a cell-free system”, Archives of Biochemistry and Biophysics 413, 99-106, 2003 62 Ho et al, “Production of unmodified human adult hemoglobin in Escherichia coli”, Proc. Natl. Acad. Sci. USA, Vol. 90, pp. 8108-8112, Sept 1993. 42 Ho et al, “Production of unmodified human adult hemoglobin in Escherichia coli”, Proc. Natl. Acad. Sci. USA, Vol. 90, pp. 8108-8112, Sept 1993. 64 Stetler et al., “Expression of fully functional tetrametic human hemoglobin in Escherichia coli”, Proc. Natl. Acad. Sci. USA, Vol 87. 65 Arnone et al, “High-Resolution X-ray Study of Deoxy Recombinant Human Hemoglobins Synthesized from βGlobins Having Mutated Amino Termini”, Biochemistry, 31, 8640-8647, 1992. 66 Ho et al, “Production of human normal adult and fetal hemoglobins in Escherichia coli”, Protein Engineering, Vol. 10, No. 9, pp. 1085-1097, 1997. 67 Corinne Vasseur-Godbillion, Djemel Hamdane, Veronique Baudin-Creuza et al., “High-yield expression in Escherichia coli of soluble human α-hemoglobin complex with its molecular chaperone”, Protein Engineering, Design & Selection, 2006 68 Van Amersfoort, E.S., Van Berkel, T.J.C., & Kuiper, J. (2003). Receptors, mediators, and mechanisms involved in bacterial sepsis and septic shock. Clinical microbiology reviews, 16(3), 379-414. 69 Scott, M.G., Kucik, D.F., Goodnough, L.T., & Monk, T.G. (1997). Blood substitutes: evolution and future applications. Clinical chemistry, 43(9), 1724-31. 70 Rogers, D.E. (1960). Host mechanisms which act to remove bacteria from the blood stream. Bacteriological reviews, 24(1), 50-66. 71 Bearman, G.M., & Wenzel, R.P. (2005). Bacteremias: A Leading Cause of Death. Archives of Medical Research, 36(6), 646-659. 72 Van Amersfoort, E.S., Van Berkel, T.J.C., & Kuiper, J. (2003). Receptors, mediators, and mechanisms involved in bacterial sepsis and septic shock. Clinical microbiology reviews, 16(3), 379-414. 73 Baron, S. (1996). Medical Microbiology. University of Texas Medical Branch. 74 Voyich, J.M., Musser, J.M., & DeLeo, F.R. (2004). Streptococcus pyogenes and human neutrophils: a paradigm for evasion of innate host defense by bacterial pathogens. Microbes and Infection, 6(12), 1117-1123. 75 Foster, T.J. (2005). Immune evasion by staphylococci. Nature reviews. Microbiology, 3(12), 948-58. 76 Leaver, S.K., Finney, S.J., Burke-Gaffney, A., & Evans, T.W. (2007). Sepsis since the discovery of Toll-like receptors: Disease concepts and therapeutic opportunities. Critical care medicine, 35(5), 1404-10. 77 Finlay, B.B., & McFadden, G. (2006). Anti-immunology: evasion of the host immune system by bacterial and viral pathogens. Cell, 124(4), 767-82. 78 Rabehi, L., Irinopoulou, T., Cholley, B., Haeffner-Cavaillon, N., & Carreno, M.P. (2001). Gram-positive and gramnegative bacteria do not trigger monocytic cytokine production through similar intracellular pathways. Infection and immunity, 69(7), 4590-9. 79 Somerville, J.E., Cassiano, L., Bainbridge, B., Cunningham, M.D., & Darveau, R.P. (1996). A novel Escherichia coli lipid A mutant that produces an antiinflammatory lipopolysaccharide. The Journal of clinical investigation, 97(2), 359-65. 80 Karch, H., Leying, H., Goroncy-Bermes, P., Kroll, H.P., & Opferkuch, W. (1985). Three-dimensional structure of fimbriae determines specificity of immune response. Infect. Immun., 50(2), 517-522. 81 Kuwajima, G. (1988). Flagellin domain that affects H antigenicity of Escherichia coli K-12. J. Bacteriol., 170(1), 485-488. 82 Schembri, M.A., Ussery, D.W., Workman, C., Hasman, H., & Klemm, P. (2002). DNA microarray analysis of fim mutations in Escherichia coli. Molecular genetics and genomics : MGG, 267(6), 721-9. 83 Pósfai, G., Kolisnychenko, V., Bereczki, Z., & Blattner, F.R. (1999). Markerless gene replacement in Escherichia coli stimulated by a double-strand break in the chromosome. Nucleic acids research, 27(22), 4409-15. 84 Kang, Y., Durfee, T., Glasner, J.D., Qiu, Y., Frisch, D., Winterberg, K.M., et al. (2004). Systematic mutagenesis of the Escherichia coli genome. Journal of bacteriology, 186(15), 4921-30. 85 Link, A.J., Phillips, D., & Church, G.M. (1997). Methods for generating precise deletions and insertions in the genome of wild-type Escherichia coli: application to open reading frame characterization. Journal of bacteriology, 179(20), 6228-37. 86 Macnab, R.M. (1992). Genetics and biogenesis of bacterial flagella. Annual review of genetics, 26, 131-58. 87 Claret, L., & Hughes, C. (2002). Interaction of the Atypical Prokaryotic Transcription Activator FlhD2C2 with Early Promoters of the Flagellar Gene Hierarchy. Journal of Molecular Biology, 321(2), 185-199. 88 Van Amersfoort, E.S., Van Berkel, T.J.C., & Kuiper, J. (2003). Receptors, mediators, and mechanisms involved in bacterial sepsis and septic shock. Clinical microbiology reviews, 16(3), 379-414. 89 Cohen, J. The immunopathogenesis of sepsis. Nature, 420(6917), 885-91. 63 90 Trent, M.S. (2004). Biosynthesis, transport, and modification of lipid A. Biochemistry and cell biology = Biochimie et biologie cellulaire, 82(1), 71-86. 91 Zhang, Y., Gaekwad, J., Wolfert, M., & Boons, G. (2007). Modulation of Innate Immune Responses with Synthetic Lipid A Derivatives. J Am Chem Soc. 92 Lu, M., Zhang, M., Takashima, A., Weiss, J., Apicella, M.A., Li, X., et al. (2005). Lipopolysaccharide deacylation by an endogenous lipase controls innate antibody responses to Gram-negative bacteria. Nat Immunol, 6(10), 989-994. 93 Kawasaki, K., Ernst, R.K., & Miller, S.I. (2004). 3-O-deacylation of lipid A by PagL, a PhoP/PhoQ-regulated deacylase of Salmonella typhimurium, modulates signaling through Toll-like receptor 4. The Journal of biological chemistry, 279(19), 20044-8. 94 Somerville, J.E., Cassiano, L., Bainbridge, B., Cunningham, M.D., & Darveau, R.P. (1996). A novel Escherichia coli lipid A mutant that produces an antiinflammatory lipopolysaccharide. The Journal of clinical investigation, 97(2), 359-65. 95 Coats, S.R., Do, C.T., Karimi-Naser, L.M., Braham, P.H., & Darveau, R.P. (2007). Antagonistic lipopolysaccharides block E. coli lipopolysaccharide function at human TLR4 via interaction with the human MD-2 lipopolysaccharide binding site. Cellular Microbiology, 9(5), 1191-1202. 96 Meredith, T.C., Aggarwal, P., Mamat, U., Lindner, B., & Woodard, R.W. (2006). Redefining the Requisite Lipopolysaccharide Structure in Escherichia coli. ACS Chemical Biology, 1(1), 33-42. 97 Somerville, J.E., Cassiano, L., & Darveau, R.P. (1999). Escherichia coli msbB gene as a virulence factor and a therapeutic target. Infection and immunity, 67(12), 6583-90. 98 Post, D.M.B., Ketterer, M.R., Phillips, N.J., Gibson, B.W., & Apicella, M.A. (2003). The msbB Mutant of Neisseria meningitidis Strain NMB Has a Defect in Lipooligosaccharide Assembly and Transport to the Outer Membrane. Infect. Immun., 71(2), 647-655. 99 Trent, M.S. (2004). Biosynthesis, transport, and modification of lipid A. Biochemistry and cell biology = Biochimie et biologie cellulaire, 82(1), 71-86. 100 Van Amersfoort, E.S., Van Berkel, T.J.C., & Kuiper, J. (2003). Receptors, mediators, and mechanisms involved in bacterial sepsis and septic shock. Clinical microbiology reviews, 16(3), 379-414. 101 Kawasaki, K., Ernst, R.K., & Miller, S.I. (2004). 3-O-deacylation of lipid A by PagL, a PhoP/PhoQ-regulated deacylase of Salmonella typhimurium, modulates signaling through Toll-like receptor 4. The Journal of biological chemistry, 279(19), 20044-8. 102 Somerville, J.E., Cassiano, L., Bainbridge, B., Cunningham, M.D., & Darveau, R.P. (1996). A novel Escherichia coli lipid A mutant that produces an antiinflammatory lipopolysaccharide. The Journal of clinical investigation, 97(2), 359-65. 103 Meredith, T.C., Aggarwal, P., Mamat, U., Lindner, B., & Woodard, R.W. (2006). Redefining the Requisite Lipopolysaccharide Structure in Escherichia coli. ACS Chemical Biology, 1(1), 33-42. 104 Foster, T.J. (2005). Immune evasion by staphylococci. Nature reviews. Microbiology, 3(12), 948-58. 105 Tosi, M.F. (2005). Innate immune responses to infection. The Journal of allergy and clinical immunology, 116(2), 241-9. 106 Foster, T.J. (2005). Immune evasion by staphylococci. Nature reviews. Microbiology, 3(12), 948-58. 107 Finlay, B.B., & McFadden, G. (2006). Anti-immunology: evasion of the host immune system by bacterial and viral pathogens. Cell, 124(4), 767-82. 108 Stevens, P., Young, L.S., & Adamu, S. (1983). Opsonization of various capsular (K) E. coli by the alternative complement pathway. Immunology, 50(3), 497-502. 109 Johnson, J.R. (1991). Virulence factors in Escherichia coli urinary tract infection. Clinical microbiology reviews, 4(1), 80-128. 110 Roberts, I.S. (1996). The biochemistry and genetics of capsular polysaccharide production in bacteria. Annual review of microbiology, 50, 285-315. 111 Roberts, I.S. (1996). The biochemistry and genetics of capsular polysaccharide production in bacteria. Annual review of microbiology, 50, 285-315. 112 Whitfield, C. (2006). Biosynthesis and assembly of capsular polysaccharides in Escherichia coli. Annual review of biochemistry, 75, 39-68. 113 Whitfield, C. (2006). Biosynthesis and assembly of capsular polysaccharides in Escherichia coli. Annual review of biochemistry, 75, 39-68. 114 Rong, R., Slupska, M.M., Chiang, J., & Miller, J.H. (2004). Engineering large fragment insertions into the chromosome of Escherichia coli. Gene, 336(1), 73-80. 115 Burns, S.M., & Hull, S.I. (1998). Comparison of loss of serum resistance by defined lipopolysaccharide mutants and an acapsular mutant of uropathogenic Escherichia coli O75:K5. Infection and immunity, 66(9), 4244-53. 116 Whitfield, C. (2006). Biosynthesis and assembly of capsular polysaccharides in Escherichia coli. Annual review of biochemistry, 75, 39-68. 117 Whitfield, C. (2006). Biosynthesis and assembly of capsular polysaccharides in Escherichia coli. Annual review of biochemistry, 75, 39-68. 118 Ackerman et al. Accumulation of Toxic Concentrations of Methylglyoxal by Wild-Type Escherichia coli K-12. Journal of Bacteriology. 119(2):357, 1974. 119 Zhao et al. Tumor-targeting bacterial therapy with amino acid auxotrophs of GFP-expressing Salmonella typhimurium. PNAS 102(3):755, 2005. 120 Rowe, Summers. The Quiescent-Cell Expression System for Protein Synthesis in Escherichia coli. Applied and Environmental Microbiology 65(6):2710. 1999 121 Jana et al. Amino acid changes in the repressor of bacteriophage lambda due to temperature-sensitive mutations in its cI gene and the structure of a highly temperature-sensitive mutant repressor. Protein Engineering. 12(3):225, 1999 122 Bernard et al. Positive-selection vectors using the F plasmid ccdB killer gene. Gene. 148(1):71, 1994 123 Ham et al. A tightly regulated inducible expression system utilizing the fim inversion recombination switch. Biotechnology and Bioengineering. 94(1), 2006 124 Santivarangkna et al. Alternative Drying Processes for the Industrial Preservation of Lactic Acid Starter Cultures. Biotechnol. Prog. 23(2): 302, 2007. 125 Potts, M. Desiccation Tolerance of Prokaryotes. Microbiological Reviews. 58(4):755, 1994 126 Tullis, JL. Albumin: 1. Background and Use. 2. Guidelines for Clinical Use. JAMA, 237: 355-360, 1977. 127 Sakai et al. Systemic and microvascular responses to hemorrhagic shock and resuscitation with Hb vesicles. Am J Physiol Heart Circ Physio 283, Sept. 2002. 128 Terajima et al. Fluid resuscitation with hemoglobin vesicles in a rabbit model of acute hemorrhagic shock. Shock 25(2):184. 2006.