English
advertisement

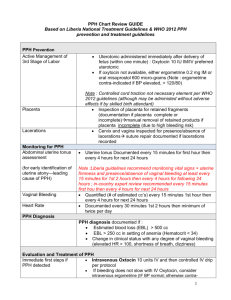
Strategy for the Reduction of Morbidity and Mortality from POSTPARTUM HAEMORRHAGE Reproductive Health Task Force Safe Motherhood Unit Ministry of Public Health Islamic Government of Afghanistan 2005 FOREWARD Intrapartum Working Group Strategy on Prevention and Management of PPH i Intrapartum Working Group Strategy on Prevention and Management of PPH ii Table of Contents FOREWARD .............................................................................................................................. i STRATEGY FOR THE REDUCTION OF MATERNAL MORTALITY FROM POSTPARTUM HEMORRHAGE ............................................................................................ 3 Definition of PPH .................................................................................................................. 3 THE INTERVENTIONS FOR REDUCING MORTALITY FROM PPH ............................... 4 Preventing PPH in Situations WITHOUT a Skilled Birth Attendant ................................... 4 Community Awareness and Behavior Change Communication (BCC) ............................. 4 Birth Planning.................................................................................................................... 5 Promotion of Skilled Attendance At Birth .......................................................................... 5 Detection and Treatment of Anemia .................................................................................. 6 Community Based Distribution and Education on the Use of Misoprostol for Routine Use in the Third Stage of Labor......................................................................................... 6 Family Planning and Birth Spacing .................................................................................. 7 Managing PPH in Situations WITHOUT a Skilled Birth Attendant .................................... 7 Birth Planning.................................................................................................................... 7 Community Emergency Plans ............................................................................................ 8 Referral Strategies ............................................................................................................. 8 Preventing PPH in Situations WITH a Skilled Birth Attendant ........................................... 9 Community Awareness and BCC ....................................................................................... 9 Antenatal Care (to include Birth Planning)....................................................................... 9 Detection and Treatment of Anemia ................................................................................ 10 Family Planning and Birth Spacing ................................................................................ 10 Use of the Partograph to Reduce Prolonged Labor ........................................................ 10 Limiting Episiotomy in Normal Birth .............................................................................. 11 Active Management of the Third Stage of Labor ............................................................. 11 Routine Inspection on the Placenta for Completeness .................................................... 12 Routine Inspection of the Perineum and Lower Vagina for Lacerations ........................ 12 Routine Immediate Postpartum Monitoring .................................................................... 13 Management of PPH in Situations WITH a Skilled Birth Attendant ................................. 13 Active Triage of Emergency Cases .................................................................................. 13 Rapid Assessment and Diagnosis..................................................................................... 13 Emergency Protocols for PPH......................................................................................... 14 Basic and Comprehensive Emergency Obstetric Care .................................................... 14 CONCLUSION ........................................................................................................................ 15 Figure 4. Strategies for Reduction of Mortality from Postpartum Hemorrhage .................. 17 APPENDIX 1: Use Of Oxytocic Drugs In Pregnancy and Childbirth Care ............................ 18 References for information on oxytocic drugs..................................................................... 21 Intrapartum Working Group Strategy on Prevention and Management of PPH 1 Intrapartum Working Group Strategy on Prevention and Management of PPH 2 STRATEGY FOR THE REDUCTION OF MATERNAL MORTALITY FROM POSTPARTUM HEMORRHAGE The Prevention and Management of Postpartum Hemorrhage Maternal mortality in Afghanistan is unacceptably high and the Ministry of Health has taken substantial steps to address this problem. Globally, the most common cause of maternal mortality is postpartum hemorrhage (PPH), accounting for 25% of maternal deaths. However, in Afghanistan, while PPH is still the most common cause of death, it is responsible for 38% of the maternal deaths, much higher than the global average1. This is an urban as well as a rural problem as noted in Table 1. There are various reasons for these terrible statistics, yet there can be a single response: to make the reduction of death from postpartum hemorrhage a focused strategy within the overall framework of reproductive health in Afghanistan. Knowing the burden that PPH puts on the health sector, a targeted strategy can increase the likelihood that appropriate actions can be taken. Table 1. Percentage of Maternal Deaths Due to Postpartum Hemorrage, by Province Province Percent of maternal deaths due to PPH Kabul 50% Laghman 30% Kandahar 36% Badakshan 24% AFGHANISTAN 38% Reduction of PPH must recognize the reality in Afghanistan that more than 90% of people deliver without the assistance of a skilled provider. Any strategy must look at a variety of interventions that can be employed in environments with a skilled attendant, as well as environments without. As well, such a strategy must consider options for prevention as ewll as treatment. Figure 1. shows the basic framework for interventions, while Figure 4 gives the interventions in detail. This paper describes the potential interventions, and suggests strategies for implementing these interventions. Figure 1. Framework for Reduction of PPH Without a Skilled Attendant Prevention Strategies Management Strategies With a Skilled Attendant Potential Interventions Definition of PPH The loss of at least 500 ml of blood following delivery is defined as a PPH. How a particular individual is able to withstand that amount of blood loss determines if that PPH will result in a death or simply a complication. For some women who are very anemic at the start of labor, the loss of even 250 ml of blood puts their lives at risk; whereas a healthy woman who is not anemic may loose 1000 ml of blood or more without serious morbidity. 1 MOH/UNICEF/CDC RAMoS study, 2002. Intrapartum Working Group Strategy on Prevention and Management of PPH 3 Thus, although PPH is defined by this cutoff, those with less blood loss can still experience shock and need aggressive treatment to save their lives. THE INTERVENTIONS FOR REDUCING MORTALITY FROM PPH Figure 4 lists the interventions, by category, that should be a part of a comprehensive strategy for reducing PPH. All these activities and interventions come together in a comprehensive approach to the reduction of death from postpartum hemorrhage. Preventing PPH in Situations WITHOUT a Skilled Birth Attendant In order to have an impact on preventing PPH at the community level, in places where there are typically no skilled birth attendants, the community and family must be supported to take the following actions. Community Awareness and Behavior Change Communication (BCC) While prevention of hemorrhage may be in the hands of the provider and the woman, prevention of mortality from PPH is an issue for the entire community. Communities should be taught regarding the necessity of skilled care at birth, and that their actions are central to making a difference for women. BCC tools, such as the Birth Planning Flip Chart should be used to educate and inform all members of the community and to foster a dialogue around action to prevent mortality and morbidity. In situations where there is no skilled attendant, the Birth Planning Flip Chart can be used by Female CHWs to help pregnant women and their families make concrete plans and know what they can expect of their community Female CHWs to engage TBAs and other female village leaders about the need for planning and the options offered by health services Male CHWs to discuss with mullahs and shuras the importance of preventive action and rapid responses in times of emergencies Male CHWs to help men and husbands know the concrete things that they must do to prepare for a healthy birth TBAs and family diyas to guide families in preparations for birth, and advocate for the use of available, local PPH reduction strategies (such as misoprostol2) Male and female CHWs (as well as some TBAs) to educate communities about danger signs, design community interventions and understand the importance of skilled attendance and health services All members of the community to promote the concepts of birth preparedness and complication readiness. As well, communities must work with health care providers to identify reasons why women do or do not seek delivery services at health facilities. Women, families, communities and 2 The Ministry of Health is ready to undertake a pilot project to understand the mechanism by which misoprostol can be best used in the Afghan context to prevent postpartum hemorrhage. Intrapartum Working Group Strategy on Prevention and Management of PPH 4 health care providers should work together to develop culturally appropriate delivery services that enable women to confidently seek care at health facilities. Birth Planning Women and families, especially decision-makers within families, should develop a specific plan for their birth, including what to do in the event of a complication. Much of what a woman needs for having a healthy birth can be anticipated, such as choosing an appropriate place for birth, having the right supplies and materials, etc. Furthermore, lack of planning can contribute to making a simple problem become a big complication. For example, when a laboring woman does not arrange for someone to care for her other children, she may make decisions to leave the birthing area prematurely to care for other children, thus increasing her risk of complications. A critical component of the birth plan should be the choice of where to deliver and with whom to deliver. Women should consider all the benefits and limitations of delivering at home, and the possibilities of NOT delivering at home. This conclusion should not be reached simply based on tradition, lack of information or the sudden onset of labor prior to the consideration of birth location. The birth plan should also include a list of needed materials for the birth including: perineal pads/cloths, soap, clean bed cloths, placenta receptacle, clean razor blade, waterproof/plastic sheet3 and clean cord ties. Promotion of Skilled Attendance At Birth A key intervention for reducing PPH is the presence, at the birth, of a health care provider who is trained in the necessary interventions to save life. Only a skilled attendant should practice active management of the third stage of labor4 and administer oxytocin, a central part of that intervention. As well, only a trained and skilled provider can determine if the placenta has been delivered completely and how much postpartum bleeding is normal. An experienced provider will know how to help the uterus remain contracted following delivery, to prevent additional blood loss, or repair a laceration that is bleeding. Skilled providers can identify problems early, and intervene early, in order to limit blood loss. For the coming years in Afghanistan, it will be difficult to have a midwife in every community, nor should this be the goal, as skilled providers must have adequate clinical volume to maintain their skills. It will be possible, ultimately, to have a midwife at many facilities that serve these women and communities. Midwives must be facility based, but with a strong outreach program to enable them to move into communities and provide personal care to women as needed. By having midwives posted at basic and comprehensive health 3 Although a plastic sheet is recommended, it should not suggest that women should lie down on this sheet to deliver their baby. Birth in the squatting position is an often used technique that assists with normal birth. 4 Active management of the third stage of labor includes administration of oxytocin (within 1 minute of delivery), early clamping and cutting of the umbilical cord and controlled cord traction. It is not recommended that this combination of interventions be practiced by traditional practitioners (TBAs). Intrapartum Working Group Strategy on Prevention and Management of PPH 5 centers, women and their families know where to go to request the care they need for a healthy birth. Detection and Treatment of Anemia Studies in Afghanistan have demonstrated that approximately 71% of women have some degree of iron-deficiency anemia5. Given this alarmingly high statistic, it is reasonable to assume that ALL pregnant women are in need of iron and folate supplementation during before, during and after pregnancy. Community health workers should distribute iron and folate to all women in the community who are pregnant, and where possible, to all women who are planning pregnancy. CHWs should also be taught, where there is no skilled attendant, how to make a clinical diagnosis of anemia, and when to refer cases that seem to not respond to iron supplementation. CHWs should know: How to make a clinical diagnosis of anemia o Pale palms or fingernail beds; pale conjunctiva or oral mucosa o Fatigue and shortness of breath (from only slight exertion) Which women to refer for evaluation at the health facility o Any woman who is short of breath o Any woman who is so fatigued that she cannot perform her routine household work o Any woman with obvious signs of anemia o Any woman who does not appear to improve after 3 months of iron and folate supplementation While anemia itself does not cause postpartum hemorrhage, the treatment of anemia will help women to be able to withstand serious morbidity and mortality if they do face a hemorrhage. Women who have higher hemoglobin levels will have a greater reserve if they face a hemorrhage during pregnancy and delivery. If a woman is severely anemic at the start of her labor, then she can only lose a small amount of blood during the labor and birth before her health is at risk. Provision of iron and folate to treat anemia and increase hemoglobin levels will help women be more prepared for the possibility of a pregnancy-related hemorrhage. Community Based Distribution and Education on the Use of Misoprostol for Routine Use in the Third Stage of Labor Recent evidence has demonstrated that women who deliver at home may still be able to benefit from selected recent medical advances6. The routine use of 600 mcg of oral misoprostol, immediately following delivery of the baby and before delivery of the placenta, is an effective way to reduce postpartum blood loss. Misoprostol causes uterine contractions similar to oxytocin and ergometrine, but unlike oxytocin and ergometrine, is available as a tablet and is heat-stable, making it uniquely accessible to women who are delivering at home. 5 6 MICS, 2003, UNICEF http://www.mnh.jhpiego.org/resources/PPH.pdf Intrapartum Working Group Strategy on Prevention and Management of PPH 6 A study done in Indonesia demonstrated that a program of community-based education about postpartum hemorrhage and distribution of misoprostol was safe, acceptable, feasible and effective at reducing postpartum hemorrhage and subsequent morbidity and mortality. Further information is needed in order to understand how to best develop a program for reducing postpartum hemorrhage using misoprostol in Afghanistan. Well designed studies have proven that misoprostol is effective in reducing postpartum hemorrhage. Additional effort and resources are not needed to prove what is already known. However, the best method for using misoprostol in the Afghan context has yet to be determined. Therefore, a pilot program to understand the mechanism for successful education of users and families, as well as, distribution and use of misoprostol at the community level in Afghanistan is clearly needed. Family Planning and Birth Spacing Research and global experience have demonstrated that one of the most important initiatives for improving women’s health and reducing mortality is to help them plan their pregnancies and space their births. When a woman’s health is at its best – meaning she is not anemic, she is not suffering from micronutrient deficiencies and she is properly rested with respect to work and other child care responsibilities – she is more likely to have a healthy pregnancy and birth. Indeed, the concept of “too young, too old, too many, too close” suggests increased risk in pregnancies which are too frequent or too close together. Once a family has achieved the number of children that it desires and feels prepared to care for, it should be supported to reduce the chances of unplanned pregnancy. Traditional and modern family planning methods should be made available to women so as to reduce the number of times that an individual woman faces the risk of complications of pregnancy. Birth spacing options – especially postpartum methods – should be made available to women and men. Community health workers should be taught and supported to provide appropriate birth spacing methods according to their job description, including lactational amenorrhea method, condoms, oral pills and injectables. Managing PPH in Situations WITHOUT a Skilled Birth Attendant While the above listed interventions are useful in prevention of PPH, they will not prevent all cases of PPH. Therefore, program planners and implementers must consider additional interventions that allow for the management of PPH when there is no skilled attendant. Birth Planning A woman, her family and her community must be prepared in the event that she develops danger signs during labor and birth at home. Heavy bleeding before, during or after the birth must be responded to immediately with a previously prepared emergency plan. That plan must include Intrapartum Working Group Strategy on Prevention and Management of PPH 7 Decision making – who will make the decision to leave if there is a complication Emergency transport – including who has the vehicle or donkey/cart, and is fuel available or must it be purchased Emergency funds – enough for transport, medications, blood transfusion and medical services. As this amount may be more than any family can afford, communities may consider a community fund, designed for any community member who is in need of it. Walking blood donor – in case a transfusion is necessary when the woman arrives to the facility. As well, women, families, mullahs, community groups and all concerned parties must be educated about the tell-tale signs of danger in pregnancy and during and after birth. The following danger signs indicate the need to enact the complication readiness plan: Vaginal bleeding Difficulty breathing Fever Severe abdominal pain Severe headache/blurred vision Convulsions/loss of consciousness Community Emergency Plans Communities, as well as women and families, need to develop, review and implement emergency plans for addressing the needs of women who develop complications during pregnancy and birth. For those women who chose to deliver at home – then experience excessive bleeding – plans must be in place to mobilize community resources to aid the woman’s access to curative care. Communities should have plans in place to mobilize emergency funds, transport, blood donors and support mechanisms to allow women to get to nearby or far off medical services. As well, communities should consider what means of communication they might use in an emergency. Where radios or telephones are available, members of the community should know how to access them. Where they are not available, communities should consider how to communicate their needs in the shortest time interval possible. In the current security situation in Afghanistan, communities should also work with local police to develop a mechanism to allow safe passage/escort in times of heightened security or curfew. Referral Strategies Given that all clinical services are not available at all levels of the health system, referral strategies must be developed to link women in need with available services. Communities, mullahs and all those consulted in an emergency must know where services are available and how to move women between various levels of the health system. Intrapartum Working Group Strategy on Prevention and Management of PPH 8 Preventing PPH in Situations WITH a Skilled Birth Attendant In order to have an impact on preventing PPH in hospitals, CHCs and BHCs with a skilled attendant, the provider and the staff of the health facility, as well as the woman, the family and the community, must be supported to take appropriate actions. When anemia is detected early in pregnancy, patients should be provided the medical interventions to correct this anemia, and vigilantly followed up. When anemia is severe the woman should be sent to an appropriate facility for treatment, including blood transfusion, if necessary. Providers must also standardize the intrapartum care provided in facilities to include certain critical elements that reduce the likelihood of PPH, including: routine use of the partograph, restriction of episiotomy, routine postpartum inspection of the placenta for completeness routine inspection of the vulva and vagina for lacerations, routine use of active management of the third stage of labor, and routine postpartum monitoring of the woman for a minimum of 6 hours. Community Awareness and BCC Community participation will also play a great role in prevention and management of PPH in the presence of a skilled provider. Without the support of community leaders and mullahs, women will have limited access to skilled attendants and appropriate clinical facilities. Communities must understand and advocate for routine use of skilled birth attendants for every pregnant woman. They must understand the unpredictability of obstetric complications and the natural course of postpartum hemorrhage when a skilled attendant is not present. Communities must actively participate in initiatives to include them and their views in the development and continual improvement of clinical services. Communities must work with clinical facilities to develop culturally appropriate birthing areas where women feel welcome and safe. It is in these facilities that women can get the skilled care needed to prevent and manage postpartum hemorrhage. Antenatal Care (to include Birth Planning) Antenatal care – with a focus on birth planning – can be an important part of a comprehensive effort for reduction of mortality from PPH. An effective antenatal encounter, which allows a skilled provider to impact postpartum hemorrhage includes: History taking to understand if the woman has previously suffered from postpartum hemorrhage History taking for conditions that suggest that the woman needs additional care, including history of prolonged or obstructed labor, previous cesarean section or close interval between pregnancies Physical examination focusing on clinical signs of sever anemia Routine distribution of iron and folate, due to endemic levels of anemia, Intrapartum Working Group Strategy on Prevention and Management of PPH 9 Measurement of hemoglobin levels to assessment for severe anemia, with treatment if detected, Birth planning to help the woman and her family develop a birth preparedness and complication readiness plan Discussion of appropriate options for birth spacing following the delivery Plan for follow up, to evaluate the impact of treatment for anemia or to further the discussion of the birth plan. Detection and Treatment of Anemia As noted above, anemia during pregnancy increases a woman’s risk of morbidity from a postpartum hemorrhage. ANC visits provide an opportunity to identify and treat anemia with sufficient time to impact the health of the woman. If severe anemia is detected, the woman’s name should be put on a list for intensive follow up by the health provider. She should have regular visits, including consultation with an obstetrician or physician, if necessary. She should be provided sufficient iron for the duration of the pregnancy and the postpartum period. Family Planning and Birth Spacing As noted previously, birth spacing plays an important role in the promotion of general health, including healthy subsequent pregnancies. Birth spacing improves the health of the woman by increasing the interval between pregnancies and reduces the chance of unplanned pregnancy and the number of times a woman is exposed to the risks that come with pregnancy. All skilled providers should be very familiar with the various methods of birth spacing and be able to competently provide counseling and services in the following methods: Natural methods, such as the standard days method and lactational amenorrhea method Condoms Oral pills Injectables Intrauterine device When a couple decides that they have achieved their desired family size, the provider should be able to discuss with them various options for limiting the number of pregnancies, including, IUD, vasectomy and tubal ligation. Use of the Partograph to Reduce Prolonged Labor Prolonged labor, as well as intrapartum infection as a result of prolonged labor or prolonged rupture of membranes, are contributing factors to uterine atony, the number one cause of PPH. Routine use of the partograph – for all women in labor – assists the provider to detect prolonged labor and act in a timely manner to limit its impact. Intrapartum Working Group Strategy on Prevention and Management of PPH 10 Limiting the length of labor reduces the chance of infection, as well as postpartum “uterine fatigue”, a situation that can make the uterus less responsive to oxytocic drugs postpartum. When the uterine muscle is fatigued from long labor it requires higher doses and different types of uterotonic agents in order to sustain uterine tone postpartum, and reduce blood loss. Limiting Episiotomy in Normal Birth While uterine atony is the most common cause of PPH, vaginal and vulvar lacerations are also a significant cause. Most women, including primiparous women, can successfully have a vaginal delivery without the need for an episiotomy. Routine or common use of episiotomy increases the chance that a woman will lose an excessive amount of blood. Providers should be trained in techniques to reduce the need for episiotomy. Clear evidence has demonstrated that the majority of episiotomies are not necessary7. Selective rather than routine use of episiotomy results in lower levels of perineal trauma, decreased need to suture while not increasing need for newborn resuscitation or lowering Apgar scores at birth. All institutional deliveries should include routine inspection of the perineum and lower vagina following the delivery, in an effort to reduce undiagnosed vulvovaginal trauma and undetected blood loss. Active Management of the Third Stage of Labor Active management of the third stage of labor is a central intervention in the prevention of postpartum hemorrhage.8 All women who deliver with a skilled provider, whether in a hospital, health center or home, should receive active management of the third stage of labor. As shown in Figure 2, active management of the third stage of labor: Reduces postpartum hemorrhage (≥ 500 mL) by 62% Reduces severe postpartum hemorrhage (≥ 1000 mL) by 67% Reduces the need for postpartum transfusion by 66% Reduces prolonged third stage by 82% In order to successfully implement a strategy of routine active management, health care facilities must: Make active management the standard of care Ensure adequate supplies of oxtocin in the delivery room Train all providers in the technique Put systems in place to facilitate its application (readiness of delivery sets, availability of oxytocin, statistics to track the trends in postpartum hemorrhage, etc.) 7 Carroli G, Belizan J. Episiotomy for vaginal birth (Cochrane Review). In: The Cochrane Library, Issue 3, 2004. Chichester, UK: John Wiley & Sons, Ltd. 8 Neilson JP. 1998. Evidence-based intrapartum care: evidence from the Cochrane Library. Int J Gynecol Obstet. 63 (Suppl 1): S97-102. Intrapartum Working Group Strategy on Prevention and Management of PPH 11 Figure 2. Active vs. Expectant Management of Third Stage of Labor ACTIVE vs. EXPECTANT MANAGEMENT OF THIRD STAGE 6 studies 4850 women 95% CI Postpartum Hemorrhage >500 ml 0.38 (0.32-0.46) Loss of blood >1000 ml 0.33 (0.21-0.51) Maternal hemoglobin 24-48 h postpartum <9 g/l 0.40 (0.29-0.55) Need for transfusion 0.34 (0.22-0.56) Third stage >40 min 0.18 (0.14-0.24) Manual removal of placenta 1.21 (0.82-1.78) Postpartum curettage 0.74 (0.43-1.28) Vomiting 2.19 (1.68-2.86) Nausea 1.83 (1.51-2.23) Apgar<7 at 5º min. 1.00 (0.38-2.66) Newborn admission to ICU 0.82 (0.60-1.11) No breastfeeding at discharge 0.92 (0.82-1.04) .1 .2 1 5 10 A study done in Guatemala, demonstrated that there were substantial financial savings to hospitals when active management was applied routinely. These savings, in need for transfusion, occupancy of hospital beds, need for other uterotonic drugs and volume of linen to be laundered, far outweigh the costs of the 10 IU vial of oxytocin. Routine Inspection on the Placenta for Completeness Following delivery of the placenta, there should be a routine inspection of the placenta to ensure that it is complete. The provider should evaluate the maternal surface of the placenta as well as the membranes to ensure that no portion remains in the uterus, as this can cause postpartum bleeding or infection. Routine Inspection of the Perineum and Lower Vagina for Lacerations In addition to conducting a routine inspection of the placenta, the provider should also inspect the perineum and the lower vagina for lacerations. A careful and gentle inspection may reveal bleeding areas that need to be sutured. All second degree lacerations must be sutured, both to control bleeding and to restore perineal integrity. First degree lacerations should repaired only if they are bleeding or are needed to restore normal anatomy. If the woman is not bleeding, or bleeding lightly, it is rarely necessary to conduct a deep pelvic inspection to evaluate the integrity of the cervix. This frequently causes substantial pain for the woman and rarely demonstrates a laceration in need of repair in the absence of bleeding. Intrapartum Working Group Strategy on Prevention and Management of PPH 12 Routine Immediate Postpartum Monitoring The immediate postpartum period is a time of rapid involution of the uterus and great physiological changes for the woman. It is also a time of great risk as the majority of PPH occurs during this time. While PPH can and does occur after this initial 6 hour period, it is less likely. Therefore, it is essential to monitor women in the first 6 hours post delivery as part of a comprehensive plan to reduce PPH and mortality and morbidity from it. Furthermore, women who deliver in a facility and think that they are fine, may go home early from that facility. If heavy bleeding later develops, they may be less likely to return because they have left the facility and may feel that the most dangerous period is over. Immediate postpartum monitoring should include the following points, demonstrated here in a sample postpartum monitoring flow sheet. Figure 3. Immediate Postpartum Monitoring Sheet Time Blood Pressure (post delivery) Pulse Uterine Tone Vaginal Bleeding (firm or soft) (light, moderate or heavy) 00:30 01:00 02:00 06:00 Management of PPH in Situations WITH a Skilled Birth Attendant Active Triage of Emergency Cases Cases of postpartum bleeding that arrive at the facility should be identified as an emergency and moved rapidly into the evaluation area. All members of the staff – from guards and cleaners to midwives and doctors – should be able to identify women in need of emergency evaluation. Systems can be put in place to move those cases through the common initial delays that families encounter at the entrances to busy hospitals. Guards can be taught to ask some screening questions (“Do you have heavy bleeding?”, “Have you fainted or become very weak?”), referral facilities can be provided with red “Alert!” cards, that help identify emergency referrals, and families can be taught key words (“bleeding”, “fainting”) that capture the attention of providers. Regardless of the strategy, the speed with which people access the assessment areas should be monitored to ensure that the triage system is working properly. Rapid Assessment and Diagnosis Once inside the facility, patients need rapid assessment and diagnosis of PPH. A scheme of rapid initial assessment of all patients should be routine for all presenting patients, so as to Intrapartum Working Group Strategy on Prevention and Management of PPH 13 screen those with a life-threatening emergency. This assessment scheme can be applied by any level of health worker, who then alerts appropriate personnel to further the evaluation. The general approach to a patient who presents with bleeding must include: o Assessment: History – including an assessment for shock General Physical Exam – including an assessment for shock Pelvic Examination Appropriate laboratory tests o Diagnosis o Plan and Intervention, and o Evaluation. In order for this scheme to work, providers must be available at all times in the facility to make rapid diagnostic decisions. Emergency Protocols for PPH A patient who is diagnosed with PPH must receive immediate standardized resuscitation measures regardless of the cause. Initial measures are enacted to treat or prevent shock, while mobilizing other personnel and resources to further identify the specific cause for the hemorrhage. Standardized approaches in diagnosis and treatment of PPH (as outlined in the WHO Manual Management of Complications in Pregnancy and Childbirth) should be posted in the emergency treatment area and delivery room. All staff should be trained in the decisionmaking processes required to manage PPH and should be familiar with the posted protocols. In order to ensure the readiness of services to respond to emergencies such as PPH, emergency drills should be periodically conducted (approximately every 3 months) for staff in the delivery room and emergency treatment areas. The periodic review of these standard protocols should serve as a quality assurance mechanism to ensure that the facility is always ready to respond to a PPH emergency. Basic and Comprehensive Emergency Obstetric Care Once emergency cases are recognized and the cause of PPH is identified, the facility must have the mechanisms – personnel, supplies, drugs and equipment – to properly manage the case. The elements of basic emergency obstetric care related to management of PPH include: Intravenous fluid resuscitation Parenteral oxytocics Parenteral antibiotics Manual removal of placenta Removal of placental fragments Intrapartum Working Group Strategy on Prevention and Management of PPH 14 As well, there are critical measures that all staff should know for managing PPH cases: Uterine massage Bimanual uterine compression Aortic compression Emptying/catheterization of the bladder Placenta inspection Vulvar and vaginal inspection Cervical inspection Suturing of tears Uterine curettage These clinical supervisors should ensure that all staff posted to the labor and delivery area are proficient in the above listed measures. For cases that do not respond to the above basic interventions, the elements of comprehensive emergency obstetric care are necessary, and include: Obstetric surgery – laparotomy, uterine repair, hysterectomy and repair of high vaginal and cervical trauma Anesthesia, and Blood transfusion. Facilities should be classified as providing basic or comprehensive essential/emergency obstetric care, then properly supported to effectively apply these services. CONCLUSION The basic strategies outlined in this paper are meant to provide guidance to all those people helping to manage and implement Essential Obstetric Care services. Program managers and health officers who are working to reduce maternal mortality from postpartum hemorrhage, should implement these interventions and activities, depending on whether they work in situations where they have or do not have skilled providers. Intrapartum Working Group Strategy on Prevention and Management of PPH 15 Figure 4. Strategies for Reduction of Mortality from Postpartum Hemorrhage Management Prevention Without a Skilled Birth Attendant With a Skilled Birth Attendant Community Awareness – BCC/IEC Birth Planning Promotion of skilled attendance at birth Family Planning and Birth Spacing Detection and treatment of anemia (clinical S&S) Community Based Distribution of Misoprostol for Routine Third Stage Use Birth planning Community emergency planning Transport planning Referral strategies Community Awareness – BCC/IEC Antenatal Care (to include Birth Planning) Detection and treatment of anemia Family Planning and Birth Spacing Use of Partograph to reduce prolonged labor Limiting episiotomy in normal birth Active Management of the Third Stage of Labor Routine inspection of placenta for completeness Routine inspection of perineum/vagina for lacerations Routine immediate postpartum monitoring Active triage of emergency cases Rapid assessment and diagnosis Emergency protocols for postpartum hemorrhage management Basic EmOC o intravenous fluid resuscitation o manual removal of placenta o removal of placental fragments o parenteral oxytocics & antibiotics Comprehensive emoc o blood bank/blood transfusion o operating theatre/ surgery Supporting Components: Women’s Empowerment; Respect for Human Rights; Access to Care; Community support & mobilization; Access, utilization and quality of Essential Obstetric Care services. Intrapartum Corking Group Strategy on Prevention and Management of PPH 17 APPENDIX 1: Use Of Oxytocic Drugs In Pregnancy and Childbirth Care Oxytocic drugs, particularly oxytocin, misoprostol, and ergometrine, are beneficial for certain obstetric indications. The, indications, use, availability, misuse, contraindications, side effects, storage, and cost for each of these oxytocic drugs are outlined below. This information should be used to guide the use of these drugs in Afghanistan. Oxytocin Indications Use Availability Misuse Contraindications Side Effects Storage Cost Oxytocin is used for labor induction, labor augmentation, active management of third stage, and management of PPH. Oxytocin should only be used for induction/ augmentation in a facility where Cesarean section is available. Oxytocin should only be used by skilled attendants (midwives, doctors, nurses with midwifery skills). For active management of third stage: 10 units IM. Oxytocin should be available at health facilities providing labor and childbirth care. Oxytocin should also be available from pharmacies but only with a prescription from a doctor or a midwife. Oxytocin should not be used by unskilled persons to speed up labor and delivery, as this may result in ruptured uterus. In countries where oxytocin is available to the general public, there have been maternal and fetal deaths associated with its use. There are no contraindications to oxytocin use for active management of third stage and management of PPH. Labor induction/augmentation is contraindicated for fetal distress, placenta previa, transverse fetal lie, cord prolapse with live fetus, and obstetric hemorrhage. When used during labor, oxytocin may cause uterine hyperstimulation, which may result in fetal distress and possibly uterine rupture. However, in the postpartum period when used in the recommended dose, oxytocin has no known side effects. The total dose of oxytocin for the management of PPH should not exceed 60 units. Oxytocin should be stored at 4 to 8ºC but can be removed from storage up to 48 hours before use. Oxytocin is approximately 2 – 10 Afghanis per vial. Intrapartum Corking Group Strategy on Prevention and Management of PPH 18 Misoprostol Indications Use Availability Misuse Contraindications Side Effects Storage Cost Misoprostol is indicated for the following conditions: missed abortion; induction of labor following intrauterine fetal death; and prevention and treatment of post-partum hemorrhage. For labor induction, misoprostol should only be used in facilities with the ability to provide cesarean section. In general, misoprostol should only be used by skilled attendants (midwives, doctors, nurses with midwifery skills); however, in programs that support birth planning and childbirth, it should be available at the community level through CHWs. For missed abortion: 400-600 mcg by mouth every four hours up to 24 hours. For induction of labor following intrauterine fetal death: 50 mcg per vagina every four hours until delivery. For prevention of PPH: 600 mcg by mouth (one dose). For treatment of PPH: 1000 mcg per rectum (one dose). Misoprostol should be available at health facilities providing labor and childbirth care and through CHWs at the community level, as part of a program for birth planning and reduction of PPH at home births. Misoprostol should not be available to the general public. As misoprostol is a new drug in Afghanistan, efforts should be made by all healthcare providers and policy makers to limit its use to those described above. Widespread misuse of this drug will have a negative impact that may limit its availability and public health impact. Induction of labor (in fetal death) with misoprostol is contraindicated for women with prior cesarean section or other uterine scars. Misoprostol may cause uterine hyperstimulation, which may result in fetal distress and possibly uterine rupture. For this reason its use in induction of labor is not recommended at this time Side-effects to misoprostol are dose-dependant; doses used for labor induction are well-tolerated. Doses used for post partum hemorrhage prevention and treatment have been associated with fever and shaking chills. Misoprostol should be stored at room temperature in a dry area. While the production costs of misoprostol are low (i.e. 5-10 Afghanis per tablet), the market price ranges from 150-700 Afghanis per tablet. Intrapartum Corking Group Strategy on Prevention and Management of PPH 19 Ergometrine Indications Ergometrine is used for the treatment of post-partum hemorrhage. Use Ergometrine should only be used by skilled attendants (midwives, doctors, nurses with midwifery skills). Availability Ergometrine should be available at health facilities providing labor and childbirth care. Ergometrine should not be available to the general public and should not be sold in pharmacies. Misuse Prophylactic use of oral ergometrine after childbirth has no benefit and should be avoided. Contraindications Ergometrine is contraindicated in women with hypertensive disorders (pre-eclampsia, eclampsia, essential hypertension), ischemic cardiac disease, or history of a cerebrovascular accident or myocardial infarction, due to risk of vasoconstriction potentiating an ischemic event. Ergometrine should not be administered by rapid IV infusion due to risks of vasoconstriction. Side Effects The common side effects of ergometrine include nausea, vomiting, rise in blood pressure, and headache. Other side effects, which are rare, include symptomatic myocardial and cerebral ischemia in patients with no contraindications. Patients should therefore be monitored closely after receiving this medication. Storage Ergometrine should be stored from 4 - 8ºC and not exposed to light. Cost Ergometrine is approximately 4 Afghanis per vial. Intrapartum Corking Group Strategy on Prevention and Management of PPH 20 References for information on oxytocic drugs Kwast BE. Maternity care in developing countries. In: Health matters. Public health in NorthSouth perspective. Van der Velden K et al (eds). Houten, Bohn Stafleu Van Loghum 1995. Afghanistan: Country Profile Table. World Bank. Available at: http://devdata.worldbank.org/external/CPProfile.asp?SelectedCountry=AFG&CCODE=AFG &CNAME=Afghanistan&PTYPE=CP. Accessed: February 3, 2004. Fact Sheet: Reproductive Health Indicators in Afghanistan. UNFPA. Available at: http://www.unfpa.org/emergencies/afghanistan/factsheet.html. Accessed: February 24, 2004. Ryden G, Sjoholm I. The metabolism of oxytocin in pregnant and non-pregnant women. Acta Obstet Gynecol Scand 1971, 50:37. American College of Obstetrics and Gynecology. ACOG Practice Bulletin: Induction of Labor. ACOG Practice Bulletin Number 10. Washington, D.C:ACOG, 1999. Egypt Ministry of Health and Population. Egypt: National Maternal Mortality Study 2000. Report of Findings and Conclusions. Egypt: Directorate of Maternal and Child Health Care, Ministry of Health and Population, 2001. Goldberg AB, Greenberg MB, Darney PD. Misoprostol and pregnancy. N Engl J Med 2001;344:38-60. Karkanis SG, Caloia D, Salenieks ME, Kingdom J, Walker M, Meffe F, Windrim R. Randomized controlled trial of rectal misoprostol versus oxytocin in third stage management. Obstet Gynaecol Can. 2002;24(2):149-54. Hofmeyr GJ, Nikodem VC, de Jager M, Gelbart BR. A randomised placebo controlled trial of oral misoprostol in the third stage of labor. Br J Obstet Gynaecol. 1998;105(9):971-5. JHPIEGO. Preventing Post-partum Hemorrhage: A Community-Based Approach Proves Effective in Rural Indonesia. Program Brief, Maternal & Neonatal Health. Baltimore, JHPIEGO, 2004. O'Brien P, El-Refaey H, Gordon A, Geary M, Rodeck CH. Rectally administered misoprostol for the treatment of postpartum hemorrhage unresponsive to oxytocin and ergometrine: a descriptive study. Obstet Gynecol. 1998;92(2):212-4 Intrapartum Corking Group Strategy on Prevention and Management of PPH 21