Structured question Description This is a photo of part of the Right

Structured question
Description
This is a photo of part of the Right foot. There is a well-demarcated deeply red coloured plaque affecting the third and fourth toes, there is some extension more proximally up the foot and possible extension into the toe web spaces. There are two small satellite lesions medially on the third toe.
There is overlying surface scale and the skin appears lichenified.
There are associated nail changes consisting of yellowing and thickening of the fourth and fifth toenails.
The skin of the foot appears pale.
Differentials
Psoriasis – The well demarcated rash with overlying scale makes this a possibility. Psoriasis is known to have an underlying genetic predisposition and is also known to be more common in smokers. Psoriasis can be associated with nail changes, which are present in this patient.
Tinea Pedis – This can also present as a scaly well demarcated rash more commonly between the lateral toe-web spaces. Itch can be an associated feature as can associated thickening, discoloured and brittle nails.
Discoid Eczema – Can also present as a well demarcated red scaly plaque, which in older adults tends to affect the lower legs more commonly.
Investigations
Skin scrapings
I would explain to the patient that I would use a scalpel blade to scrape at the surface of the rash attempting to collect a sample of the surface scale. This would then be sent for microscopy and culture. The aim would be to try and identify a fungal cause for her rash.
Nail clippings
These could either be taken by myself or collected by the patient. These should be a sample of the thickened affected portion of the nail and any associated debris, which may have collected beneath the nail. These would again be sent for to the lab for microscopy and culture looking for a dermatophytic, candidal or mould cause for the patients’ rash.
Other skin signs
If the rash was due to Psoriasis I would be looking for manifestations elsewhere on the body. I may find well-demarcated plaques, which may exhibit overlying surface scale. Within the flexures, psoriasis can take on a smooth glazed appearance without scale. I would examine the nails as they can be affected in
25-50% of cases with pitting and onycholysis being the commonest features.
If Tinea Pedis was the cause of the rash, again there may be other areas of skin affected, most commonly the groin, Tinea Cruris, although this is less common in females. The axillae and sub-mammary folds can also be sites of tinea involvement.
With Discoid Eczema there may be coin-shaped lesions of eczema over the limbs which can take on a vesicular or lichenified appearance. There may been a history of atopic eczema as a child.
History
Starting with the onset of the rash, I would want to know what it looked like when it first appeared, how it evolved and areas of spread. Are there any exacerbating or relieving factors e.g. sunlight which can help with psoriasis in the majority of cases.
I would want to know about any previous dermatological problems in particular eczema in earlier life, is there a history of atopy?. I would want to know a bit more about the rash her father suffered from as in the case of psoriasis, they may be a genetic predisposition. A more detailed drug history is needed, her GP may need to be contacted to enquire about her medication for hypertension, in particular beta-blockers, which are known to be a trigger for psoriasis. Over-thecounter medications should also be noted.
I would enquire about her usual footwear as if she has a tendency to wear closed shoes, which encourage a warm humid environment, this could make Tinea more likely.
I would want to know about any close contacts that had also been had a similar recent rash, this would raise the possibility of an infective or infestational cause.
Diagnosis
From my list of differentials I think the most likely diagnosis would be Psoriasis.
I have chosen this taking into account the appearance with associated nail changes, the history with possible family history.
Herbal Cream
The problem with using ‘herbal’ creams:
Such products do not have to satisfy the same research, development and manufacturing processes as prescribed medications.
It is difficult to know the exact nature of the ingredients
It is difficult to know what response it may have on the rash and the response may not be reproducible if the cream is not regularly batchtested.
May increase the risk of an irritant or allergic contact dermatitis
If these products are used prior to presenting to medical staff, the appearance of the rash may have changed which could make the diagnosis less clear.
I would advise her to bring in the cream so we could try and establish its ingredient base, if this was difficult to establish, I would advise against the use of such creams.
Two possible triggering factors
Drugs – Beta-Blockers, litium and anti-malarials can make psoriasis worse or precipitate it.
Koebner Phenomenon – Psoriasis can appear in areas of damaged skin such as superficial scratches or scars.
Treatments
Treatment of psoriasis can be split into topical and systemic treatments. Topical treatments are the usual first-line treatment:
Topical Vitamin D Analogues: These are useful in mild to moderate chronic plaque psoriasis and counter the epidermal cell proliferation which is responsible for the thickened plaques often seen. Apart from irritation, hypercalcaemia can be a problem if recommended doses are exceeded.
Topical Steroids: particularly useful for face and flexural psoriasis, the main problems relate to long-term use, namely skin atrophy, tachyphylaxis, systemic absorption and development of acne or peri-oral dermatitis.
Coal Tar preperations: These have been used for many years and work by inhibiting DNA synthesis. It is often disliked due to its smell and staining properties.
Systemic treatments:
Methotrexate: Is used in more severe psoriasis. It is a folate antagonist and has anti-inflammatory and immune modulatory effects. Disadvantages of its use are regular blood tests to monitor bone marrow and liver function and the long term of risk of liver cirrhosis.
Retinoids: Vitamin A derivatives such as acitretin can be used with topical therapies and with UVB or PUVA. Side effects include dry mucous membranes and peeling skin, more significantly, its use can cause hyperostosis and abnormal liver function.
Ciclosporin: This is an immunosuppressant which can be used in severe psoriasis with the most significant potential risk-factors are the development of skin-cancers and lymphoma. Nephrotoxicity can also be a hazard during use.
Advice about condition an treatment
It is important to explain that the underlying cause of psoriasis is not fully and although there are effective treatments, these are aimed at keeping the condition in remission rather than cure. The treatments as discussed above, can have sideeffects and it may be a matter of finding a combination which works well for the individual.
Given her localised area of involvement, treatment with a moderate potency topical steroid or a combination treatment containing steroid plus vitamin D analogue may be appropriate in her case.
If we opted for calcipotriol ointment, this could be applied initially once daily increasing to twice daily depending on response, I would warn of potential skin irritation.
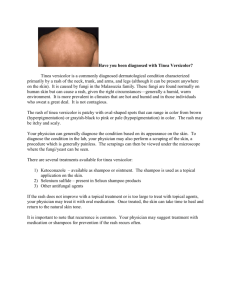
Describe the rash
The photo shows well demarcated pink plaques in both sub-mammary creases and between the breasts. The skin appears shiny and smooth but there presence of surface scale. There appears to be some areas of surface scale although not as extensive as that affecting the foot. There are satellite lesions around the larger areas of plaque.
Management
I think the appearance are of flexural psoriasis but it would be worthwhile sending some skin-scrapings for microscopy and culture to rule out a possible dermatophyte infection.
Flexural psoriasis usually responds well to mild-moderate topical steroids. Give use in flexures, the potency of steroids is magnified somewhat so I would start
with a mild steroid, hydrocortisone 1% cream, applied initially once a day after washing and drying the skin thoroughly. This could be increased to twice daily after 2-3 days if there was little response. I would expect to see a response within the first week and so would advise the patient to come back for review in approximately ten-days after which I would aim to stop using the steroid if there had been a good response.
Main differential
The main differential diagnosis would be intertrigo which could possibly be complicated with candida.
Clinical signs on the nails
There is:
Pitting
Vertical ridging
Yellow discolouration
Onycholysis –