Hospital Standards for Accreditation for Afghanistan:
advertisement

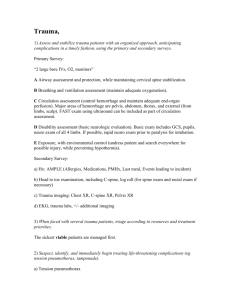
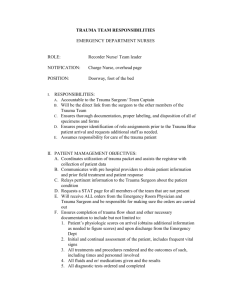
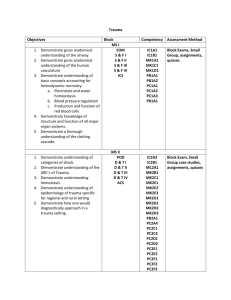
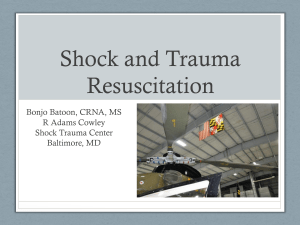
Hospital Standards for Accreditation for Afghanistan: Assessment of Progress in Achieving the Standards Hospital Department or Area: Emergency Department: Shock Management Hospital Facility: ___________________________________ Assessor: __________________________ Standard Number Standard 1 Rapid initial assessment of ABCs is conducted Date of Assessment: ________________ Emergency Department: Shock Management Criteria for Verification of Meeting Standard Compliance in Meeting Standard Full Partial None 2 1 0 Initial assessment by a physician includes: - Trauma: if trauma occurred, place 2 1 0 cervical collar unless absolutely sure it is not required - Airway: eliciting verbal response 2 1 0 - Airway: provides oxygen to all patients 2 1 0 and provides an adjunct airway as needed; Intubates as required - Breathing: notes respiratory rate, 2 1 0 abnormal breath sounds, use of accessory muscles of respiration, oxygen saturation - Circulation: Notes extremity pulses; 2 1 0 rate, strength, rhythm - Circulation: Places 2 large bore 2 1 0 peripheral IVs Basis for Evaluation Score/ Comments/Action Plan - 2 Uses a systematic approach to determining the etiology of the patient’s condition Circulation: Notes blood pressure (in all 4 extremities if indicated) - Circulation: Provides isotonic crystalloid IVFs initially. For unstable patients, 20-40 ml/kg should be given rapidly (over 10-20 minutes). - Neurologic: notes mental status and GCS or AVPU - Motor: notes any specific motor deficits - Disability/Exposure: Performs complete secondary examination when appropriate Shock is tissue hypoperfusion and is associated with decreased venous oxygen content and metabolic (lactic) acidosis. 2 1 0 2 1 0 2 1 0 2 2 1 1 0 0 - 2 1 0 2 1 0 2 1 0 2 2 1 1 0 0 2 1 0 2 1 0 - - Obtains targeted history of presenting symptoms and past medical history, including medications and drug use. Obtains blood pressure and notes pulse pressure (SBP – DBP = PP) Obtains other vital signs, including temperature, respiratory rate, heart rate. Observes mental status. Observes skin for changes including pallor, sweating, bruising, petechiae, cyanosis, decreased capillary refill, etc. Exposes the patient completely to check for occult wounds/skin changes. Orders the following laboratory studies as appropriate or available: Cbc, - - Electrolytes, BUN, creatinine, PTT, PT/inr, lactate, fibrinogen, d-dimer, cortisol, urinalysis, abg, liver function tests, blood/urine/csf cultures Orders the following as appropriate or available: Chest xray, EKG, ultrasound and/or CT scans Notes that respiratory alkalosis is common early in shock states. Notes that lactic/metabolic acidosis occurs later in shock states. Notes that hyper/hypoglycemia and hyperkalemia also occur with shock. TRAUMA/HYPOVOLEMIC: Following isotonic crystalloid resuscitation if patient is still unstable: - provides direct compression to active external bleeding - places surgical consultation for internal bleeding control - provides packed red blood cells; fully cross- matched if available or type O (negative to women of child-bearing age) as needed - Considers use of vasopressors following IVF resuscitation - Treats acidosis with IVF and ventilation - Considers placement of central line SEPTIC: Checks all vital signs: 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 2 1 1 0 0 - - - - - - Considers septic shock in all patients with T <36 or >38, SBP < 90 mm Hg, and inadequate tissue perfusion Notes tachycardia, wide pulse pressure, tachypnea, hypotension as signs of shock Notes mental status changes may occur Orders labs and additional studies as noted above as appropriate Performs aggressive ABC resuscitation with IVFs and oxygen. Provides pressors for patient not responsive to crystalloid infusion (dopamine for sbp 70-100 mm Hg, norepinephrine for sbp <70 mm Hg. Begins empiric antibiotics after obtaining cultures and removing potential infectious sources (e.g. catheters). Treats acidosis with IVF and oxygen. Administers sodium bicarbonate only if very severe. Treats DIC with FFP if available. Treats suspected adrenal insufficiency with glucocorticoids. CARDIOGENIC: Checks all vital signs. - Notes decrease in MAP by 30 mm Hg or narrow pulse pressure (< 20 mm Hg) - Checks for tachypnea, rales, wheezing, confusion, anxiety, cool clammy skin, 2 1 0 2 1 0 2 2 1 1 0 0 2 1 0 2 1 0 2 1 0 2 1 0 2 2 1 1 0 0 2 1 0 2 1 0 - - - - - decreased urine output, heart rate changes. Obtains EKG immediately to evaluate for ischemia, infarction, arrhythmias, electrolyte abnormalities, etc. Obtains chest xray immediately to evaluate for widened mediastinum, pulmonary edema, cardiac silhouette abnormalities. Considers checking CK, CK-mb, troponin levels if available. Obtains transthoracic echocardiogram if available. Aggressively treats ABCs as appropriate. Treats arrhythmias, electrolyte abnormalities, hypoxemia and hypovolemia appropriately. Gives aspirin 325 mg to the patient to chew (unless contraindicated). Provides other analgesics as appropriate (nitroglycerin 0.4 ml sl and/or morphine iv). Considers use of pressors. Consults Cardiology if available. ANAPHYLAXIS: Typically occurs within minutes to one hour following exposure to drugs, foods, stings, etc. Anaphylaxis includes respiratory failure or cardiovascular collapse. 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 2 1 1 0 0 - - - - - Obtains a thorough history if possible Obtains complete set of vital signs. Administers oxygen Considers endotracheal intubation and realizes that this may be difficult due to angioedema. Is prepared for cricothyrotomy. Removes potential contributing exposures such as IV drugs. Airway: gives epinephrine 0.3-0.5 mg IM of 1:1000 (peds 0.01 ml/kg max 0.5 mg) If hypotensive, give 1-2L IV isotonic crystalloid fluids. Consider antihistamines: Diphenhydramine 25-50 mg IV/IM/PO and H2 blocker such as ranitidine IV. Treat bronchospasm with inhaled/nebulized B2 agonist. Control persistent or delayed allergic reactions with corticosteroids (methylprednisolone IV or prednisone PO) Consider glucagons for patients on B Blockers. NEUROGENIC: caused by acute injury to the spinal cord leading to bradycardia and hypotension. - Realize that the higher the spinal cord 2 2 2 2 1 1 1 1 0 0 0 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 - - injury, the more severe symptoms that occur. Perform ABC assessment and trauma evaluation as outlined above. Give IVFs as indicated for hypotension. If refractory, give dopamine or dobutamine as indicated. Treat bradycardia with atropine. Consider high dose methylprednisolone therapy: 30 mg/kg bolus (in 15 minutes, then nothing for 45 minutes) followed by 5.4 mg/kg/h for 23 hours Consult orthopedics, neurosurgery and/or trauma surgery as indicated. 2 1 0 2 2 1 1 0 0 2 2 1 1 0 0 2 1 0