Small_Bowel_Obstruction
advertisement

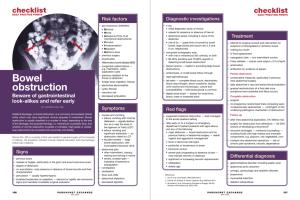
Small Bowel Obstruction This is a mechanical or functional obstruction of the small bowel, preventing normal bowel transit, and is a surgical emergency Epidemiology Accounts for about 5% of all surgical emergencies. Causes Adhesions Hernia Tumour Intussusception IBD Volvulus Foreign bodies – e.g. a gallstone in gallstone ileus Pathophysiology The bowel becomes obstructed for one of the above reasons, and becomes proximally distended. Initially this can cause increased peristalsis on either side of the obstruction and so cause diarrhoea. The intraluminal pressure will continue to rise due to the accumulation of secretions and swallowed air. Increased hydrostatic pressure in the capillary beds will cause third spacing into the intestinal lumen and contribute to dehydration. The degree of vomiting will depend on how proximal the obstruction is. Presentation Pain – usually colicky pain, though if due to strangulation, the progressive ischaemia may give rise to constant pain Nausea Vomiting – if there is bilious vomiting, and a shorter history of pain, the obstruction is more likely to be proximal Diarrhoea – an early finding Absolute constipation – a later finding Fever Ask about previous abdominal surgery Ask about a history of malignancy elsewhere – primary small bowel neoplasm is not common On examination Abdominal distension – more pronounced with distal obstruction Increased bowel sounds initially – high-pitched tinking BS, and then later, absent bowel sounds Look for hernias; stoma if present Check for signs of bowel ischaemia – fever, tachycardia, signs of peritonitis Differentials SBO Gastroenteritis Small bowel ischaemia Perforation Pancreatitis Rule out MI Investigations FBC – raised WCC U&E Group and cross-match PFA – show the valvulae conniventes extending the full width of the lumen; loops of small bowel central on film Erect CXR – air under diaphragm? Barium studies may be useful CT is useful especially if the diagnosis isn’t clear and to assess the exact level of the obstruction Treatment NPO NG IV Fluids Antibiotics to cover gram negative and anaerobes May need an anti-emetic Analgesia Adhesive obstructions often resolve without surgery Surgery may be required