Hany abdelhamid mohamed elklaf_Mirena-Klaf-5-3
advertisement

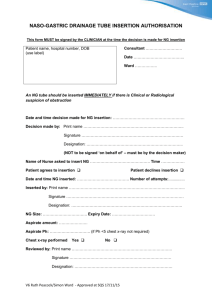
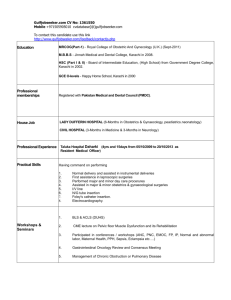
Levonorgestrel-Releasing Intrauterine System For Conservative Management Of Menorrhagia In Women In Childbearing Period Hany Abdelhamid Elkallaf, MD Department of Obstetrics & Gynecology, Faculty of Medicine, Benha University Abstract Objectives: To evaluate short-term outcome of the use of Levonorgestrelreleasing intrauterine system (LNG-IUS) for management of menorrhagia in women in the childbearing period Patients & Methods: The study included 53 multipara women with mean age of 39.4±4 years presenting with menorrhagia. All women had full history taking, clinical examination, transvaginal ultrasonography and endometrial biopsy and cervical smear evaluation prior to LNG-IUS insertion one day after cessation of menstrual bleeding. Patients were evaluated at 6 and 12 months for duration and heaviness of menstrual blood loss and for health-related quality of life was evaluated using the 5Dimensional EuroQol (EQ-5D) scoring system. Results: Nine insertions were difficult; 7 because of pain on sounding and 2 insertions were abandoned because of the presence of cervical adhesions. There were 3 IUS expulsions; two partial and a new IUS was reinserted and one complete expulsion and patient was excluded of the study. LNG-IUS significantly reduced duration and severity of blood loss at 6 and 12 months after insertion compared to baseline data with significant reduction at 12 months compared to at 6 months. At the end of 12 months; 7 women developed amenorrhea, 36 women had mild loss and 7 women had moderate loss. Quality of life scoring significantly improved at 6 and 12 months after LNG-IUS insertion compared to baseline scores. Mood and pain sub-scores showed the significant change, while the changes of the other sub-scores were non-significant. Conclusion: LNG-IUS is a safe, effective and feasible therapeutic modality for menorrhagia and is associated with significant improvement of quality of life with special regard to mood and associated pelvic pain and could be recommended as first line of management for women in childbearing period wishing to retain their power to conceive in future. Introduction By definition, diagnosis of menorrhagia is made when the duration of bleeding is equal to or greater than six days or blood loss is at least 80 ml and other pathological conditions have been excluded. However, many women seek consultation for even milder bleeding episodes, due to the associated stress, discomfort, and quality of life impairment, thus making menorrhagia one of the most frequent reasons for gynecological consultation. Menorrhagia is estimated to occur in 30% of women in their childbearing years (1, 2). Therapeutic options for menorrhagia are variant and ranging from oral medical therapy to hysterectomy. Hysterectomy is highly effective treatment with high satisfaction rates and improved quality of life especially if menorrhagia was secondary to multiple and/or large fibroids. However, the associated complications and costs may be limiting for hysterectomy to be the sole line of treatment. Moreover, hysterectomy could not be the line of management of women in late childbearing or early pre-menopausal period, (3). Hysterectomy alternatives include hysteroscopic resection which is the standard treatment for endometrial polyps and recurrence of bleeding is reduced by combining it with endometrial ablation. Myoma-related menorrhagia can be treated by Gn-RH agonists for 3 months, hysteroscopic resection for submucous myomas. Interstitial myomas can be treated by myomectomy, myolysis, uterine artery embolisation or occlusion, or hysterectomy. Laparoscopic myomectomy and uterine artery embolisation are effective, well tolerated, and the best researched. LNG-IUS is effective and well tolerated to treat adenomyosis-related menorrhagia. The effect of other conservative treatments of the uterus (endometrial ablation, uterine artery embolisation or occlusion) is limited, especially in case of deep and extensive adenomyosis. Uterine artery embolisation is the standard treatment for arteriovenous malformation, (4, 5) . Progesterone is a key hormone in regulating the female reproductive system, interacting at the level of the hypothalamus, the ovary, the uterus and the breast. Progesterone exerts effects on ovulation, endometrial differentiation, cervical mucus, breast differentiation and uterine contractility. Progestins and their analogs and antagonists have many uses in gynecology including contraception, management of miscarriage, medical abortion and treatment of conditions related to endometrial and myometrial growth and development. Beyond providing highly effective contraception, intrauterine delivery is safe and effective in the management of menorrhagia, dysmenorrhea, uterine myomata, and endometrial proliferation, (6, 7, 8). Intrauterine delivery of progestin is an effective way to administer local treatment and bypass systemic side effects. Intrauterine drug delivery has the potential to treat many gynecologic conditions, but is under utilized because clinicians lack knowledge and skills and because the current delivery systems are unavailable or costly in many countries (9) . The present prospective study aimed to evaluate short-term outcome of the use of LNG-IUS for management of menorrhagia in women in the childbearing period Patients & Methods The present prospective study was conducted at Armed Forces Hospital, King Abdul Aziz, Airbase, Dhahran, KSA since Sep 2008 till Jan 2010 to allow 12-month follow-up for the last enrolled case. After obtaining written fully informed patients' and husband' consent, the study included 53 women aged 35 to 49 years who were menstruating, had completed their desired family size, and had menorrhagia. Collected data included age, parity, number of deliveries, history of previous cesarean section, and previous contraceptive methods. Heaviness of menstrual period in the last 6 months was graduated as light, moderate, heavy or very heavy loss and the frequency of bleeding or spotting between cycles was reported. Prior to LNG-IUS insertion endometrial pathology (endometrial carcinoma and/or endometrial atypical hyperplasia) and cervical pathology (cervical cancer and preinvasive intraepithelial lesions) were excluded by D & C or endometrial sampling using Pipelle® (Cooper Surgical, Trumbull, Connecticut, USA) and cervical smear, respectively. Transvaginal ultrasonography was used to exclude possible causes of menorrhagia, including myomas and endometrial polyps, as well as adnexal pathology. Women with uterine or adnexal pathology as well as women desiring preservation of fertility were excluded from the study. Insertion of LNG-IUS was performed as an office procedure one day after cessation of menstrual bleeding. All women must have a negative urine pregnancy test prior to LNG-IUS insertion. The uterine cavity length was measured using uterine sounding, followed by LNGIUS insertion. Feasibility of insertion was defined as difficult if there was moderate or severe pain on uterine sounding or if there was need for cervical dilatation, requirement for local anesthesia or intravenous sedation for accomplishment of dilatation and IUD insertion. Accurate LNG-IUS position was documented with transvaginal ultrasonography immediately after insertion. Health-related quality of life was evaluated using the 5Dimensional EuroQol (EQ-5D) which provides a single numeric score for HRQL, is universally used, and has undergone validation in the Finnish general population. TheEQ-5D consists of five subscales that indicate dimensions of mobility, self-care, usual activities, pain, and mood each was scored as 0 or 1 and the total EQ-5D score index was calculated; better HRQL is indicated by higher scores (10, 11, 12). The EQ-5D scoring was conducted prior to and 6 and 12 months after LNG-IUS insertion Results The study included 53 women with mean age of 39.4±4; range 3549 years. All were multipara with a mean parity of 3.6±0.7; range: 3-5. Twenty-nine women (54.7%) had all their deliveries vaginally, while 24 women (45.3%) had previous cesarean sections. Previous contraception was using pills (22 women; 41.5%) or cupper IUD (24 women; 45.3%); 4 women (7.5%) were acclimatized to use safe period and 3 women (5.7%) used condom, (Table 1). The length of menstrual cycles was varied and ranged between 23 and 32 days with a mean cycle length of 27.8±3 days. Similarly, mean length of menstrual period was 7.4±1.1; range: 6-9 days. Also, the heaviness of menstrual period was variable but 20 women had heavy loss, 16 had moderate, 14 had very heavy loss and only 3 women had mild loss. Moreover, 10 women had additional spotting through the rest of the intermenstrual period, (Table 2). Insertion of LNG-IUS was feasible with no or mild tolerable pain in 17 (32.1%) and 27 (50.9%) women, respectively. Nine insertions were graded as difficult; 7 (13.2%) because of pain on sounding that required intravenous sedation till successful accomplishment of insertion, 2 insertions (3.8%) were abandoned because of the presence of cervical adhesions and were excluded of the study that included 51 women (96.2%) only. The mean uterine sound measurement was 7.3±1.5; range 5–10 cm, (Table 3). Three IUS expulsions (5.9%) occurred during the study; two partial expulsions occurred at 2 weeks and 4 months after insertion and a new IUS was successfully reinserted. One complete expulsion occurred unnoticed during the first 6 months and the subject discontinued the study and follow-up evaluation included 50 women (94.3%), (Table 3). Considering reduction of both duration and severity of blood loss; LNG-IUS significantly (p<0.05) reduced duration of blood loss at both 6 and 12 months after insertion compared to duration of blood loss prior to insertion with significantly reduced duration of loss at 12 months compared to duration of loss at 6 months, (Fig. 1). Moreover, frequency of women with short duration of blood loss was significantly higher at end of 12 months after insertion compared to that recorded at end of 6 months, (Table 4). At the end of 12 months follow-up; 7 women developed amenorrhea, 36 women had mild loss and 7 women had moderate loss, but no women had moderate or severe loss with significant reduction (X2=85.686, p<0.001) of frequency of women had excessive blood loss compared to prior to LNG-IUS. On contrary, 17 women had intermenstrual spotting with significant increase (X 2=6.113, p<0.05) of the frequency of women had spotting at the end of 12-months compared to prior to insertion of LNG-IUS, (Table 5). Quality of life scoring significantly (p<0.05) improved at 6 and 12 months after LNG-IUS insertion compared to baseline scores with nonsignificantly higher scores between 6 and 12 months records. Mood and pain sub-scores showed the significant change, while the changes of the other sub-scores were non-significant, (Table 6, Fig. 2). Table (1): Age and parity data of enrolled women Data Age (years) Findings Mean±SD 39.4±4 (35-49) Strata 35-40 35 (66.1%) >40-45 12 (22.6%) >45-50 6 (11.3%) Parity Mean±SD 3.6±0.7 (3-5) Strata 3 28 (52.7%) 4 17 (32.1%) 5 8 (15.2%) Mode of Vaginal 29 (54.7%) delivery Cesarean section 24 (45.3%) Contraceptive Pills 22 (41.5%) history Cupper IUD 24 (45.3%) Safe period 4 (7.5%) Condom 3 (5.7%) Data are presented as mean±SD & numbers; ranges & percentages are in parenthesis Table (2): Menstrual history data of enrolled women Data Length (days) menstrual cycle Findings 27.8±3 (23-32) 5 (9.4%) 20 (37.7%) 8 (15.2%) 20 (37.7%) 7.4±1.1 (6-9) 13 (24.5%) 14 (26.4%) 16 (30.2%) 10 (18.9%) 3 (5.7%) 16 (30.2%) 20 (37.7%) 14 (26.4%) of Mean±SD Strata <24 24-26 27-29 30-32 Length (days) of Mean±SD menstrual period Strata 6 7 8 9 Heaviness of menstrual Mild loss period Moderate loss Heavy loss Very heavy loss Spotting throughout No 43 (81.1%) period Yes 10 (18.9%) Data are presented as mean±SD & numbers; ranges & percentages are in parenthesis Table (3): LNG-IUS insertion and follow-up data Data Findings Uterine sound Mean±SD 7.3±1.5 (5-10) measurements Strata 5-cm 6 (11.8%) 6-cm 14 (27.5%) 7-cm 5 (9.7%) 8-cm 14 (27.5%) 9-cm 9 (17.6%) 10-cm 3 (5.9%) Insertion No difficulty 44 (83%) difficulty Difficult Pain 7 (13.2%) insertion Cervical 2 (3.8%)* adhesions Insertion pain Strata No 17 (32.1%) Mild 27 (50.9%) Moderate/severe 7 (13.2%) Post-insertion No 48 (94.2%) expulsion Partial 2 (3.8%) Complete 1 (2%)* Data are presented as mean±SD & numbers; ranges & percentages are in parenthesis *: excluded cases Table (4): Blood loss duration recorded throughout follow-up period compared to baseline data Baseline 6-m later 12-m later Mean±SD (days) 7.4±1.1 (6-9) 2.4±0.9 (1-5)* 1.6±1 (0-3)*† Strata 0-day 0 0 7 (14%) 1-day 0 7 (14%) 17 (34%) 2-day 0 23 (26%) 17 (34%) 3-day 0 14 (28%) 9 (18%) 4-day 0 5 (10%) 0 5-day 0 1 (5%) 0 6-day 12 (24%) 0 0 7-day 13 (26%) 0 0 8-day 16 (32%) 0 0 9-day 9 (18%) 0 0 Data are presented as mean±SD & numbers; ranges & percentages are in parenthesis *: significant versus baseline data significant versus 6-m after LNG-IUS insertion †: Table (5): Blood loss heaviness data recorded throughout follow-up period compared to baseline data Data Heaviness menstrual loss Baseline 12-m later of No 0 7 (14%) period Mild 3 (6%) 36 (72%) Moderate 15 (30%) 7 (14%) Heavy 19 (38%) 0 Very heavy 13 (26%) 0 Spotting No 40 (80%) 33 (66%) throughout period Yes 10 (20%) 17 (34%) Data are presented as numbers; percentages are in parenthesis Table (6): Quality of life scores recorded throughout follow-up period compared to baseline scores Baseline 3.54±0.71 1 0.86±0.35 0.94±0.24 6-m later 3.88±0.63* 1 0.88±0.33 0.96±0.20 12-m later 4.3±0.65*† 1 0.9±0.3 0.98±0.14 Total score Strata Mobility Self-care Usual activities Pain 0.3±0.5 0.52±0.5* 0.64±0.53*† Mood 0.44±0.71 0.52±0.5* 0.78±0.42*† Data are presented as mean±SD & numbers; ranges & percentages are in parenthesis *: significant versus baseline data †: significant versus 6-m after LNG-IUS insertion 9 Prior 6-m later 12-m later 8 Duration of blood loss (days) 7 6 5 4 3 2 1 0 Fig. (1): Mean (+SD) duration of blood loss prior to and after LNG-IUS insertion 6 Prior 6-m later 12-m later Quality of life score 5 4 3 2 1 0 Fig. (2): Mean (+SD) total quality of life score determined prior to and after LNG-IUS insertion Discussion The purpose of the study was to evaluate the outcome of LNG-IUS as a therapeutic modality for menorrhagia affecting a group of women in childbearing period who refused other lines as hysterectomy or endometrial ablation, LNG-IUS significantly reduced duration of blood loss and the frequency of women with prolonged duration of blood loss at both 6 and 12 months after insertion compared to duration of blood loss prior to insertion. Moreover, 36 women had mild loss and no women had moderate or severe loss with significant reduction of frequency of women had excessive blood loss compared to prior to LNG-IUS. These data indicated the beneficial effects of LNG-IUS as a sole therapeutic modality for menorrhagia and supported that previously reported in literature; Wildemeersch & Rowe (13) demonstrated the efficacy of the LNG-IUS to significantly reduce the amount of menstrual blood loss in women with menorrhagia and concluded that the therapeutic effect of this contraceptive method is highly desirable, particularly in women with heavy bleeding or anemia, as other treatment modalities are less effective, more costly, more invasive or inaccessible. Kriplani et al., (14) reported that menorrhagia was cured in 77.7% of their patients at 3 months and in all patients at 36 months with a significant decrease in the mean number of bleeding days and pictorial blood loss assessment chart score at one month, and the decrease continued with treatment duration. Moreover, Kriplani et al., (14) reported that the subjective blood loss reduction was considerable as well, and endometrial thickness was significantly decreased at 12 months. Endrikat et al., (15) compared the efficacy of LNG-IUS versus combined oral contraceptives for treatment of menorrhagia and reported that in both treatment groups, menstrual blood loss decreased significantly from baseline to 12 months but the decrease was significantly more in the LNG-IUS group, 80% of subjects had treatment success compared with 36.8 % with oral therapy and significantly consistently lower menorrhagia severity score in the LNG-IUS group at all study time points. Bednarek & Jensen (16) reported that most LNGIUS users for menorrhagia experienced a dramatic reduction in menstrual bleeding. Quality of life scoring significantly improved at 6 and 12 months after LNG-IUS insertion compared to baseline scores with mood and pain sub-scores showed the significant change; the significantly improved pain scores could be improved mood considering such pain is psychogenic in origin in addition to the presence of some sort of pelvic congestive symptoms that are mostly ameliorated with the use of the steady release progesterone. The significantly improved QoL scores despite the nonsignificant change of mobility, self care and usual activity subscores also could be attributed to improved mood while performing these activities. Moreover, the simple design characteristics of the T-shaped LNG-IUS could account for minimizing the occurrence of pain. These data coincided with Bragheto et al., (17) who reported a significant decrease in pain score at 3 and 6 months after LNG-IUS insertion. Lete et al., (18) found LNG-IUS is an effective and well-tolerated treatment modality in idiopathic menorrhagia with markedly improved QoL of women treated causing high levels of patient satisfaction and concluded that LNG-IUS can be regarded as a first-choice therapy in idiopathic menorrhagia. Gorgen et al., (19) who measured the health-related quality of life in LNGIUS and reported significant improvement of QoL scores with significant decrease of scores for pelvic pain, while libido and general feeling of health were increased. Despite these beneficial effects of LNG-IUS, at the end of 12 months follow-up; 7 women (14%) developed amenorrhea, which undesirable for women in childbearing period. The reported figure for amenorrhea goes in hand with Bragheto et al., (17) who reported that at 6 months after LNG-IUS insertion, oligomenorrhea was the most common bleeding pattern observed and Kriplani et al., (14) reported amenorrhea in 28.57% of their studied menorrhagia patients treated by LNG-IUS. Moreover, Bednarek & Jensen (16) reported that about 15% to 20% of women become amenorrheic one-year after LNG-IUS insertion. However, such event was explained prior to enrollment in the study for all women and they informed that their ability to conceive could be regained after IUD removal. Fortunately, none of these women had a desire to get pregnant. In support of the fertility regaining, Bednarek & Jensen (16) reported that for their amenorrheic women after removal of the IUD, there is rapid return to fertility, with 1-year life-table pregnancy rates of 89% for women less than 30 years of age. Intermenstrual spotting showed significantly increased frequency at the end of 12-months compared to prior to insertion of LNG-IUS and was reported in 17 women (34%). The data go in hand with Kriplani et al., (14) found Intermenstrual spotting was the most common side effect for LNG-IUS insertion for menorrhagia treatment. Bragheto et al., (17) who reported that at 3 months of LNG-IUS use, the most common bleeding pattern was spotting, and at 6 months of observation, oligomenorrhea was the most common pattern observed, although spotting was present in one third of the women. Multiple studies tried to explore the molecular mechanisms for improvement and diminution of menstrual blood loss with concomitant short menstrual period with the use of LNG-IUS; Obro et al., (20) histological reported that progesterone receptor A and B in endometrial glands were almost extinguished, reduced estrogen receptors with modulation of apoptosis in glands and stroma in LNG-IUS users compared to the oral group and concluded that the clinical effect of LNGIUS is accompanied by almost extinguished PR-receptors in glands coinciding with modulation of apoptosis and this strongly indicate that progestins activate non-classical initiated signaling pathways. Also, Maruo et al., (21) demonstrated that LNG-IUS acting as progesterone receptor modulator not only inhibits the proliferation and stimulates apoptosis of cultured leiomyoma cells but also suppresses collagen synthesis in a cell-type specific manner. Xu et al., (22) demonstrated that the proliferation rate of uterine leiomyoma cells was suppressed after treatment with LNG at a minimum concentration of 10 μg/ml and the inhibitive effect was positively correlated with the LNG concentration and with the incubation time. Flow cytometry showed that the apoptosis rate was increased with the LNG concentration while the mRNA levels of IGF-1, Bcl-2 and survivin were down-regulated significantly after treatment with 10 mcg/mL LNG and Western blot analysis confirmed that the expression of Bcl-2 and survivin was decreased significantly, and the p38 phosphorylation level was increased and caspase 3 was activated remarkably 72 h after treatment with 10 and 20 mcg/ml LNG It could be concluded that LNG-IUS is a safe, effective and feasible therapeutic modality for menorrhagia and is associated with significant improvement of quality of life with special regard to mood and associated pelvic pain and could be recommended as first line of management for women in childbearing period wishing to retain their power to conceive in future. However, larger scale studies with longer duration of follow-up are mandatory for establishment of obtained results. References 1. O’Flynn N, Britten N. Diagnosing menstrual disorders: a qualitative study of the approach of primary care professionals. Br J Gen Pract 2004; 54(502): 353–8. 2. Istre O, Qvigstad E. 2007. Current treatment options for abnormal uterine bleeding: an evidence-based approach. Best Pract Res Clin Obstet Gynaecol, 21:6:905–13. 3. Brun JL, André G, Descat E, Creux H, Vigier J, Dallay D: Methods and efficacy of medical and surgical treatment of non functional menorrhagia. J Gynecol Obstet Biol Reprod (Paris). 2008; 37 Suppl 8:S368-83. 4. Aberdeen Endometrial Ablation Trials Group. A randomized trial of endometrial ablation versus hysterectomy for the treatment of dysfunctional uterine bleeding. BJOG. 1999; 106:360-366. 5. Kennedy ADM, Sculpher MJ, Coulter A, Dwyer N, Rees M, Abrams KR, Horsley S, Cowley D, Kidson C, Kirwin C et al. (2002) Effects of decision aids for menorrhagia on treatment choices, health outcomes, and costs. JAMA 288, 2701–8. 6. Inki P. Long-term use of the levonorgestrel-releasing intrauterine system. Contraception. 2007; 75:S161–S166. 7. Bahamondes L, Petta CA, Fernandes A, Monteiro I. Use of the levonorgestrel-releasing intrauterine system in women with endometriosis, chronic pelvic pain and dysmenorrhea. Contraception. 2007; 75:S134–S139. 8. Pintiaux A, Chabbert-Buffet N, Foidart JM. Gynaecological uses of a new class of steroids: the selective progesterone receptor modulators. Gynecol Endocrinol. 2009; 25:67–73. 9. Harper CC, Blum M, de Bocanegra HT, et al. Challenges in translating evidence to practice: the provision of intrauterine contraception. Obstet Gynecol. 2008;111:1359–69. 10.EuroQol Group. EuroQol—a new facility for the measurement of health-related quality of life. Health Policy. 1990;16:199-208. 11.Ohinmaa S, Sintonen H. Inconsistencies and modeling of the Finnish EuroQol (EQ-5D) preference values. In: Gainer W, Schulenburg G, Piercy J, eds. Discussion Papers of the 15 th Annual EuroQol Plenary Meeting; October 1-2, 1998; Hannover, Germany. Hannover: Center of Health Economics and Health System Research, University of Hannover; 1998:57-74. 12.Ohinmaa A, Sintonen H. Quality of life of Finnish population as measured by the EuroQol. Presented at: the 12 th Annual EuroQol Plenary Meeting, October 3-6, 1995; Barcelona, Spain. 13.Wildemeersch D, Rowe PJ: Assessment of menstrual blood loss in women with ideopathic menorrhagia using the frameless levonorgestrel-releasing intrauterine system. Contraception. 2004; 70(2):165-8. 14.Kriplani A, Singh BM, Lal S, Agarwal N: Efficacy, acceptability and side effects of the levonorgestrel intrauterine system for menorrhagia. Int J Gynaecol Obstet. 2007; 97(3):190-4. 15.Endrikat J, Shapiro H, Lukkari-Lax E, Kunz M, Schmidt W, Fortier M: A Canadian, multicentre study comparing the efficacy of a levonorgestrel-releasing intrauterine system to an oral contraceptive in women with idiopathic menorrhagia. J Obstet Gynaecol Can. 2009; 31(4):340-7. 16.Bednarek PH, Jensen JT: Safety, efficacy and patient acceptability of the contraceptive and non-contraceptive uses of the LNG-IUS. Int J Womens Health. 2010; 1:45-58. 17.Bragheto AM, Caserta N, Bahamondes L, Petta CA: Effectiveness of the levonorgestrel-releasing intrauterine system in the treatment of adenomyosis diagnosed and monitored by magnetic resonance imaging. Contraception. 2007; 76(3):195-9. 18.Lete I, Obispo C, Izaguirre F, Orte T, Rivero B, Cornellana MJ, Bermejo I; Spanish Society of Gynaecology Obstetrics (SEGO): The levonorgestrel intrauterine system (Mirena) for treatment of idiopathic menorrhagia. Assessment of quality of life and satisfaction. Eur J Contracept Reprod Health Care. 2008; 13(3):231-7. 19.Gorgen H, Api M, Aku A, Cetin A: Use of the Levonorgestrel-IUS in the treatment of menorrhagia: assessment of quality of life in Turkish users. Arch Gynecol Obstet. 2009; 279(6):835-40. 20.Orbo A, Arnes M, Pettersen I, Larsen K, Hanssen K, Moe B: Downregulated progesterone receptor A and B coinciding with successful treatment of endometrial hyperplasia by the levonorgestrel impregnated intrauterine system. Acta Obstet Gynecol Scand. 2010; 89(11):1438-46. 21.Maruo T, Ohara N, Yoshida S, Nakabayashi K, Sasaki H, Xu Q, Chen W, Yamada H: Translational research with progesterone receptor modulator motivated by the use of levonorgestrel-releasing intrauterine system. Contraception. 2010; 82(5):435-41. 22.Xu Q, Qiu L, Zhu L, Luo L, Xu C: Levonorgestrel inhibits proliferation and induces apoptosis in uterine leiomyoma cells. Contraception. 2010; 82(3):301-8.