Erythrocyte Sedimentation Rate (ESR) SOP
advertisement
 SOP")
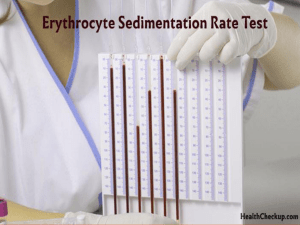
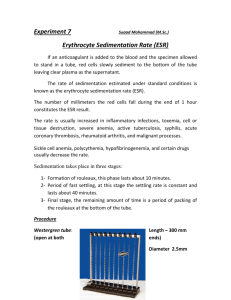
ERYTHROCYTE SEDIMENTATION RATE (ESR) PURPOSE Define a procedure to measure erythrocyte sedimentation rate in patient blood. RESPONSIBILITIES All trained and authorized medical staff at all laboratories and unit can use this SOP. Supervisor must resolve any: Problems with the process Difficulties using SOP Borderline interpretations Restrictions 1. This SOP must not be used by unauthorized laboratory medical staff. 2. An initial check must be made that the report matches the request form. 3. The Medical Director or Supervisor must then ensure that results of examination are: a. technically valid and appropriate to the patients’ clinical condition b. presented accurately and clearly c. reach the user in a timely and secure manner DEFINITIONS Erythrocyte Sedimentation Rate ESR: measures the distance red blood cells will fall along the length of a vertical tube over a given time period. A raised ESR reflects an increased production of acute-phase proteins. Although it is a non-specific phenomenon, it is clinically useful in certain chronic disorders, e.g. rheumatoid arthritis or tuberculosis, as an index of progress of the disease. A normal ESR does not exclude organic disease but, on the other hand, the vast majority of acute or chronic infections and most neoplastic and degenerative diseases are associated with changes in the plasma proteins which lead to an acceleration in sedimentation. PRINCIPLE ESR the rate of fall of RBCs in diluted plasma is influenced by a number of inter-reacting factors. Basically, it depends upon the difference in specific gravity between red cells and plasma, but the actual rate of fall is influenced very greatly by the extent to which the red cells form rouleaux, which sediment more rapidly than single cells. Other factors, which affect sedimentation, include the ratio of red cells to plasma, the plasma viscosity, the verticality of the sedimentation tube, the bore of the tube, and the dilution of the blood. Hematology Laboratory/ United Laboratories SOP No.: ULC-HEMA005TECH Effective Date: 28 FEB 2010 Version 4 Page 1 of 4 CONTROLED DOCUMENT Copy No. Sedimentation can be observed to take place in three stages: 1. Preliminary stage of at least a few minutes during which time rouleaux form. 2. A period in which the sinking of the rouleaux takes place at approximately a constant speed. 3. A phase during which the rate of sedimentation slows as the rouleaux pack at the bottom of the tube. The all important rouleaux formation is mainly controlled by the concentration of fibrinogen and other acute-phase proteins. It is also enhanced by the iimmunoglobulins. Anemia by altering the ratio of red cells to plasma, encourages rouleaux formation and accelerates the sedimentation. Sickle cells and spherocytes do not clump easily so remain suspend in plasma decreasing sedimentation. ITEMS REQUIRED Equipment and Materials Westergren sedimentation tube is made from either glass or plastic, has a length of about 30 cm and a bore of 2.5 mm. Specially made racks with a scale graduated in mm from 0 to 140 are available and these have adjustable leveling screws for holding the tubes in an exactly vertical position. Timer Reagents NA Specimens 2 ml of EDTA blood sample Documents Hospital/ Clinic Requisition form Monthly Quality Control for ESR Erythrocyte Sedimentation Rate (ESR) Log sheet ULC-HEMA005TECH/1F ULC-HEMA005TECH/2F PROCEDURES QUALITY CONTROL 1. Monthly two technologist shall run the same sample and results reviewed by Medical Director or Designee 2. It is conventional to set up sedimentation rates at room temperature (18 - 25oC), sedimentation is normally accelerated as the temperature rises Hematology Laboratory/ United Laboratories SOP No.: ULC-HEMA005TECH Effective Date: 28 FEB 2010 Version 4 Page 2 of 4 CONTROLED DOCUMENT Copy No. 3. It should be carried out within four hours of collecting the blood 4. Blood in EDTA can also be used for up to 24 hours after collection provided that it is kept at 40C. 5. The test should be protected from direct sunlight and draughts 6. It should never be set up near a radiator or on a bench where there is vibration, e.g. from a centrifuge. 7. The test is performed on venous blood diluted accurately with 31.3 g/l trisodium citrate in the proportion of one volume of citrate to four parts of blood. SAFETY Facility safety rules must be followed TECHNICAL PROCEDURE 1. Mix the blood well and draw 1.0 ml of the sample into clean dry Westergren tube. 2. Place the tube into the stand, taking care that the base is firmly positioned on the base pad to prevent leakage. 3. Adjust the rack so that the tube rests in an exactly vertical position. 4. Leave undisturbed for 60 min. 5. At the end of the hour read the height of clear plasma above the upper margin of the column of sediment cells to the nearest millimetre. 6. A poor delineation of the upper layer of red cells, so-called 'stratified' sedimentation, has been attributed to the presence of many reticulocytes. 7. Report this measurement as the ESR (Westergren) in units of mm in 1 hour. Sources of error 1. Specimen older than specified time after collection and before testing 2. Incorrect proportion of anticoagulant 3. Incorrect type of anticoagulant (calcium oxalate cause shrinkage of RBCs and decrease sedimentation. 4. Haemolysed sample 5. Contaminated sedimentation tubes 6. Tubes tilted during sedimentation 7. Test set up near central heating or direct sunshine 8. Test set up adjacent to centrifuge or other instrument causing vibration 9. Failure to read at exactly one hour. Hematology Laboratory/ United Laboratories SOP No.: ULC-HEMA005TECH Effective Date: 28 FEB 2010 Version 4 Page 3 of 4 CONTROLED DOCUMENT Copy No. INTERPRETATIONS AND RESULTS REPORTING The ranges in health are derived from several publications. The values are means ± 2SD. Male Female ESR (mm/1h) 0- 15 0- 20 In childhood and adolescence the ESR is the same as for normal men with no difference between boys and girls. Clinical Significance ESR is a non-specific test Increase ESR Decrease ESR Infection Inflammation Malignancy Leukemia Multiple Myeloma Polycythemia rubra vera Sickle cell anemia Spherocytosis REFERENCES 1. 2. 3. 4. Hematology for Medical Technologists (Charles E. Seiverd), Current Edition Practical Hematology (Sir. John V. Davie, S. M. Lewis), Current Edition WHO Guidelines on Standard Operating Procedures for Haematology. NCCLS Clinical Laboratory Technical Procedure Manual; Approved Guideline- Current Edition. Hematology Laboratory/ United Laboratories SOP No.: ULC-HEMA005TECH Effective Date: 28 FEB 2010 Version 4 Page 4 of 4 CONTROLED DOCUMENT Copy No.