CF - University of Nairobi

COMPASSION FATIGUE AMONG MEDICAL WORKERS AT KENYATTA
NATIONAL HOSPITAL (KNH), NAIROBI
Authors
1. Donald A. Kokonya, MBChB (Nairobi)
2. John M. Mburu, MBChB (Nairobi), MMed (Nairobi)
3. Dammas M. Kathuku, MBChB (Makerere), MMed (Nairobi), Av. Medicine (USA)
4. D.M. Ndetei, MBChB (Nairobi), MD (Nairobi), MRCPsych, FRCPsych. (UK)
Particulars
1. Senior House Officer, Department of Psychiatry, College of Health Sciences, University of
Nairobi, P.O. Box 72300, 00200 City Square, Nairobi.
2. Lecturer, Department of Psychiatry, College of Health Sciences, University of Nairobi.
3. Senior Lecturer, Department of Psychiatry, College of Health Sciences, University of Nairobi.
4. Professor of Psychiatry, Department of Psychiatry, College of Health Sciences, University of
Nairobi.
Requests for reprints to: Dr. D.A. Kokonya, P.O. Box 72300, 00200 City Square, Nairobi or dkokonya@yahoo.com
1
ABSTRACT
Background: Compassion fatigue continues to take toll on the health and outputs of the medical practitioners as attested by the outcomes of the studies conducted mainly in Europe and the United
States of America. Little is known about its impact on the health and performance of the Kenyan medical workers. Not much in Kenya is known about the adaptability of the Kenyan medical workers to compassion fatigue and their hardiness in coping with it.
Objective: To establish the prevalence of and factors associated with compassion fatigue among medical practitioners and nurses at the Kenyatta National Hospital, Nairobi.
Setting: Kenyatta National Hospital, Nairobi.
Design: Descriptive cross-sectional.
Subjects: Three hundred and forty five (345) medical practitioners and nurses with six or more months of work experience at Kenyatta National Hospital.
Outcome measures: Prevalence rates, socio-demographic characteristics, factors associated with and influencing compassion fatigue among the medical practitioners and nurses.
Methods: Proportionate Probability Sampling (PPS) method was used to recruit the medical practitioners and nurses on the basis of qualifications, departments and deployment.
Results: The crude prevalence rates of compassion fatigue were 29.6%. The prevalence rate of compassion fatigue for medical practitioners was 12.9% and 33.1% for the nurses. The risk factors for compassion fatigue were found to be nursing (p=0.002) and middle level college (p=0.03). In regression analysis, 93.0% of compassion fatigue among the medical practitioners and 91.0% among nurses were attributed to a combination of ‘self;’ ‘patients and their relatives’, and the ‘practitioner’s work environment’ factors. The remaining 7.0% among the medical practitioners and 9.0% among nurses were attributed to unexplained factors, not captured by the questionnaire. Individually, factors pertaining to self contributed 83.0% among medical practitioners and 73.0% among nurses and patients’ and their relatives contributed to 26.0% of compassion fatigue among the medical practitioners and 33.0% among the nurses. Work environment did not contribute to compassion fatigue among the medical workers (Table 1, Charts 1 & 2).
Conclusion: Compassion fatigue affected both medical practitioners and nurses at the KNH but the nurses were about three times (33.1%) more affected than the medical practitioners (12.9%). The sources of compassion fatigue were multifactorial (93.0%), led by ‘self-related’ factors (83.0% among the medical practitioners and 73.0% among the nurses).
INTRODUCTION
Compassion Fatigue is the combined effects of the caregiver’s visualisation of the clients’ or patients’ traumatic images added to the effects of burnout to create a condition of progressive debilitation to the caregiver 1 . Compassion Fatigue has many symptoms and they often parallel to the symptoms of the traumatized patients for whom caregivers are working 2 . While compassion fatigue has been often defined in the literature of psychotherapy as emotional contagion passed on from clients or patients to the clinician, there is growing evidence to support the trans-generational and societal transmission of this condition 1, 3, 4, 5 . Some of the symptoms of compassion fatigue include: increased negative arousal, intrusive thoughts and images of clients’ situations or trauma (or clinicians own historical trauma), difficult separating work from personal lives, lowered frustration tolerance and outbursts of anger or rage.
2
Others include dread of working with certain clients, marked or increasing transference and countertransference issues with certain clients, depression, perceptive and ‘assumptive world’ disturbances
(i.e. seeing the world in terms of victims and perpetrators, decreasing in subjective sense of safety), increase in ineffective, self-destructive and self-soothing behaviours , hyper vigilance, feelings of therapeutic impotence or deskilled with certain clients, diminished sense of purpose and enjoyment in the career, diminished ego functioning (time, identity, volition), decreased functioning in nonprofessional situations, loss of hope. Psychiatric workers’ quest for high work standards leads to secondary trauma with subsequent negative effects on themselves because they undertake much more responsibilities than they can cope with and become indifferent. This leads to the feeling of fatigue, apathy and loss of motivation. Lack of support and a need for recognition in the work environment lead to emotional fatigue. Too heavy workload, staff shortage and uncertainty regarding role description in the work environment leads to feelings of fatigue, negativity,
“stuckness”, anger and apathy 6 .The health care giving process and providing therapy to patients who have survived a traumatic event can be quite stressful. Such findings described how therapists who worked with traumatized clients often showed signs of psychological distress as a result of these interactions 7,8,9 .More specifically, compassion fatigue appeared to be the consequences of working with traumatized individuals, if the medical worker was exposed to significant numbers of traumatized patients and had a strong empathic orientation. Empathic engagement with traumatized clients often requires the medical professional to discuss details of the traumatic experience, including role play and dramatic re-enactment of the events, which are thought vital to the therapeutic process, but can have an adverse emotional impact on the health caregiver 7.10.11
. This type of vicarious trauma has often been referred to as secondary traumatic stress in the literature. When doctors and nurses report symptoms related to re-experiencing the client’s traumatic event, wishing to avoid both the client and reminders of the client’s trauma, and persistent arousal due to intimate knowledge about the client’s traumatic experiences, they are most likely to be suffering from secondary trauma 7, 9, 10, 12 . Compassion fatigue researchers also suggest that other aspects of the
7, 10, 13 . For formal caregiver’s life can influence the likelihood of developing compassion fatigue example, a history of trauma, lower social support, and an inability to cope with the demands of care giving, are thought to increase the likelihood of developing compassion fatigue. Previous research tended to support the hypothesized relationships between these risk factors, compassion fatigue, and psychological distress. Female psychologists and violence counselors with a higher percentage of sexual violence victims as clients, reported more vicarious trauma and that this was related to greater psychological problems 7, 9, 11 . A history of personal trauma is also related to poor psychological health among child welfare workers and psychotherapists 31, 36 . More evidence for the vulnerability of the medical workers to compassion fatigue and secondary trauma came from the findings from those who were involved in the 11 th September, 2001 attack on the World Trade Center, New York, recovery and counselling programmes for the injured among whom compassion fatigue was strongly present (p<0.001) 14 . In this study, an attempt was made to establish the presence of, similarity with other countries and parallel in health care giving of compassion fatigue among the medical workers at KNH
3
METHODS
This study was conducted over an eight week period from the last week of May to the first week of
July 2003, at outpatient clinics, theatres and wards at the Kenyatta National Hospital (KNH),
Nairobi. The study site was the national referral hospital and the oldest school of medicine in Kenya and was manned by 1002 medical practitioners and 1400 nurses in the year 2002. Systematic recruitment of the respondents was done by Proportionate Probability Sampling (PPS) by departments, qualifications and distribution of 345 medical workers. Seventy per cent (70.0%) medical practitioners were employees of the University of Nairobi while 99.6% were nurses employed by the KNH. About 72.0% of the medical workers carried out bedside medicine and nursing, about 27.0% worked in theatres and 1.5% worked at the emergency/casualty department.
The cut off duration of work at KNH for the study inclusion criteria was 6 months. A standard
Compassion Fatigue Self Test whose alpha reliabilities ranged from 0.94 to 0.86 and a Tucker’s
Coefficient of Congruence of 0.91 was used to measure the levels of compassion fatigue in each of the medical workers. The administration of the questionnaire was done by an experienced mental health professional. The data was analysed using the Statistical Package for Social Sciences (SPSS) version 10.0. The level of statistical significance was held at p<0.05.
RESULTS
A total of 345 medical were recruited from 67 centres, of whom 62/345 (18.0%) were medical practitioners while the nurses accounted for 283/345 (82.0%). There were 94/345(27.2%) male medical workers of whom 47/345(13.6%) were medical practitioners and another 47/345(13.6%) were nurses. The female medical workers constituted 249/345(72.2%) of whom 15/345(4.3%) were medical practitioners and 234/345(67.8%) were nurses. The participants’ age range was 23-53 years with the youngest (23 years) and oldest (53 years) being nurses in both cases. The mean age was 35.0 years (SD 7.6) and the median age of 33 years. Of the study population, the medical practitioners constituted 62/1002 (6.2%) while the nurses were 283/1400 (20.2%).
4
Table 1: Compassion Fatigue: Socio-demographic factors n CF
1 Sex
Male
Female
2 Age
94
251
23.4
31.1
<30
31-35
36-40
41-45
>45
3 Marital status
Ever married
Single
97
60
45
39
32
274
70
27.8
26.7
33.3
30.8
34.4
29.9
25.2
4 Religion
Catholics
Protestants
Muslims
Other
5 Profession
Medical practitioner
Nurse practitioner
6 Education
College
University
7 Years as practitioner
0-5
6-10
11-15
16-20
8
21-25
26-30
>30
Duration
(years)
0-5
6-10
11-15
16-20
21-25
26-30
9 Employer
KNH at KNH
99
229
7
8
62
283
273
72
99
89
47
34
44
21
10
133
67
31
30
20
12
300
33.1
16.7
24.2
30.3
25.5
38.2
28.3
29.3
42.9
0.0
12.9
32.5
25.0
33.3
50.0
23.3
32.8
48.4
16.7
35.0
25.0
30.7 p=0.16 p=0.89 p=0.48 x 2 not valid p=0.002
P=0.03 p=0.47 p=0.052 x 2 not valid
5
UON
MOH
6
30
16.7
16.7 p=0.06
Self & Others 6 16.7
Prevalence rate
Based on the Compassion Fatigue Self Test (CFST) scale for compassion fatigue, this study considered moderate compassion fatigue as the reference point. High and extremely high compassion fatigue were considered pathological, giving a prevalence rate of 103/348(29.6%) among the medical workers. The prevalence rate of compassion fatigue for the medical practitioners was 8/62(12.9%) while that for the nurses was 94/284(33.1%) (Table 1).
Sex
Both male 94/345 (27.2%) and female 251/345 (72.8%) medical workers experienced compassion fatigue albeit low levels, though it was slightly higher among the females compared to males. The differences in the levels of compassion fatigue by gender did not have statistical significance (p=0.16) (Table 1).
Age
Compassion fatigue was low among young doctors (26.7-27.8%) and high among the older generation medical workers (34.4%) above the age of 45 years. About 58.0% of the medical workers were less than 36 years of age and had compassion fatigue levels below 28.0%. The compassion fatigue levels had a small range (26.7-34.4 or 7.7%) which did not have a statistical significance (p=0.78) (table 1).
Marital status
The majority of the medical workers 274/345 (79.4%) were married and their level of compassion fatigue was found to be 29.9% compared to the single 70/345 (20.6%) whose level of compassion fatigue was 25.2%. There was no statistical significance in the marital status
(p=0.48) (Table 1).
Religion
The medical workers at KNH were predominantly Christian 328/345 (95.1%). Among the
Christians, the level of compassion fatigue was low and the difference between the Catholics
(28.3%) and Protestants (29.3%) was negligible (x 2 not valid). The were only 7/345 (2.0%)
Muslims in the study whose compassion fatigue level was 7.0% and members of other religious groups 8/345 (2.3%) did not have any compassion fatigue (Table 1).
Profession
The majority of the medical workers283/345 (82.0%) in this study were nurses compared to the doctors 62/345 (18.0%). The nurses suffered compassion fatigue almost three times (32.5%) as much as the medical practitioners (12.9%). The differences in the levels of compassion fatigue among the two categories of professionals were statistically significant (p=0.02) (Table 1).
6
Education
The majority of the medical workers in this study, 273/345 (79.1%) had pursued education up to college level while 72/345 (20.9%) attained University education. The level of compassion fatigue among those who attained college level of education (33.1%) most of whom were nurses was approximately double that among the university graduates (16.7%) most of whom were medical practitioners and the difference was statistically significant (p=0.03) (Table 1).
Years as a practitioner
Majority of the medical workers 235/345 (68.1%) had been in employment for up to 15 years and experienced compassion fatigue in the range of 24.2-30.3%. The practice duration of 6-10 years was only second to the over ten years in being high risk for compassion fatigue. A small proportion of the medical workers 10/345 (2.9%) had been in the practice for more than 30 years and experienced the highest level of compassion fatigue (50.0%). The differences in the levels of compassion fatigue were not statistically significant (p=0.47) (table 1).
Duration at KNH
The largest number of the medical workers 231/345 (67.0%) had worked for up to 15 years at
KNH, with a peak work duration of 0-5 years (38.6%). The highest level of compassion fatigue
(48.4%) was experienced by the medical workers who had worked at KNH for 11-15 years followed by the work duration of 21-25 years whose level of compassion fatigue was 35.0%. The least compassion fatigue (16.7%) was experienced by those in the work duration of 16-20 years.
The differences in the work duration at KNH did not have statistical significance (p=0.052)
(table) 1.
Employer
The majority of the medical workers 300/345 (87.0%) were employees of KNH followed by the
Ministry of Health (6.7%). The employees of KNH suffered the highest level of compassion fatigue (30.7%) while employees of the University of Nairobi, Ministry of Health and others all experienced 16.7% compassion fatigue. These differences in the levels of compassion fatigue however, had no statistical significance (p=0.06) (table 1).
7
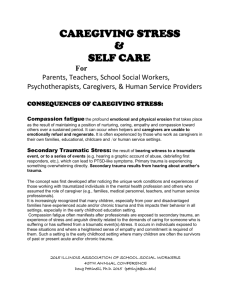
CHART 1: Regression Analysis by Profession & Influencing Factors
0.7
0.6
0.5
0.4
0.3
0.2
Medical Practitioners
Nurses
0.1
0
Self Patients & Relatives Work Environment
Influencing Factors
Regression analysis showed that 93.0% of compassion fatigue among the medical practitioners and
91.0% among nurses at KNH could be explained by a combination of factors attributable to ‘self;’
‘patients and their relatives’, and the ‘practitioners’ work environment’. This implied that 7.0% of compassion fatigue among the medical practitioners and 9.0% among the nurses could only be attributable to unexplained factors, not captured by the questionnaire. Thirty six point one percent
(36.1%) of compassion fatigue among the medical practitioners and 53.1% among the nurses were attributable to self factors. Patients and their relatives contributed 33.5% of compassion fatigue among the medical practitioners 32.1% among the nurses. Work environment affected medical practitioners (23.2%) more than eight times more than the nurses (2.7%). The contribution of self, patients and their relatives and work environment to the medical practitioners’ compassion fatigue were statistically significant (p=0.00, p=0.00 & p=0.004 respectively). Among the nurses, the contributions of self and patients and their relatives to their compassion fatigue were statistically significant (p=0.00 & p=0.00 respectively) while the work environment was not statistically significant (p=0.477). Self factors exposed nurses to compassion fatigue while work environment exposed medical practitioners to compassion fatigue. (Chart 1).
8
DISCUSSION
Prior to this study, no other study had ever been conducted in Kenya to determine the levels of compassion fatigue among medical workers or any other population in the care-givers’ industry.
About 87.0% of the study sample comprised employees of the Kenyatta national referral and teaching hospital (KNH) which also handled many emergencies on a daily basis. It is on the premise that the medical workers at KNH had been vulnerable to compassion fatigue for a long time and there was need to produce evidence for it. The assumption by Figley et al that there existed a causal relationship between exposure to trauma and development of psychological distress and compassion fatigue therefore, held water among the medical workers at KNH 7 . The key predictors of compassion fatigue among those who were involved in the recovery and counselling of the victims of the September 11, 2001 attack on the World Trade Center (WTC),
New York, were identified to be the degree of exposure to trauma, previous personal history of trauma, the care givers’ social support systems and environmental factors. In the study on those who were involved in the recovery and counselling of the victims of the September 11, 2001 attack on the World Trade Center (WTC), 81.8% of the study sample had at least had a lifetime exposure to traumatic events 14 . The presence of compassion fatigue among medical workers
(29.6%) at the KNH, Nairobi, was found to be higher among nurses (32.5%) compared to the medical practitioners (12.9%) and with a statistically significant difference (p=0.002). High educational levels and by extension, largely being a medical practitioners (16.7%) cushioned medical workers (p=0.003) from compassion fatigue compared to middle level colleges whose membership predominantly comprised nurses and below (31.4% and 34.3% respectively). There were progression trends in which compassion fatigue increased with the medical workers’ ages and years of practice, though both did not have statistical significance, similar and comparable to the findings among those who were involved in the recovery and counselling of the September
11, 2001 victims of the WTC attack 14 . These findings were comparable with those of other studies conducted in other countries on similar population samples 1, 2, 3, 4, 5.
The males experienced slightly lower levels of compassion fatigue than the females, though the sex differences had no statistical significance (p=0.16), a finding also established among those who were involved in the recovery and counselling of the September 11, 2001 attack on the World Trade Center (WTC),
New York. The married (30.0%) medical workers experienced higher compassion fatigue compared to the singles (21.0%). Similar findings was established among the medical workers who were involved in the recovery and counselling of the victims of the September 11, 2001 attack on the World Trade Center (WTC) in New York City in the study conducted in the year
2004 14 . In the Kenyan study, regression analysis showed that environmental factors were found not to have made any contribution to the compassion fatigue among the medical workers compared to that for the medical workers involved in the recovery and counselling of the victims of WTC attack among whom, favourable environmental working conditions were found to lessen compassion fatigue significantly (p<0.001) 14. About 93.0% of compassion fatigue among the medical practitioners and 91.0% among the nurses were found to be caused by a combination of factors including self, patients’ relatives and work environment. The instrument did not capture the causes of compassion fatigue among the medical practitioners (7.0%) and nurses (9.0%) respectively. The uncaptured sources of compassion fatigue among medical workers could be explained by the fact that the instrument was not developed with the local communities specifically. This variation may call for modification of the instrument for future studies. Thirty six point one percent (36.1%) of compassion fatigue among the medical practitioners and 53.1% among the nurses were attributable to self factors. Patients and their relatives contributed 33.5% of compassion fatigue among the medical practitioners 32.1% among the nurses. Work environment affected medical practitioners (23.2%) more than eight times more than the nurses (2.7%).
9
The contribution of self, patients and their relatives and work environment factors to the medical practitioners’ compassion fatigue were statistically significant (p=0.00, p=0.00 & p=0.004 respectively). Among the nurses, the contributions of self and patients’ relatives factors to their compassion fatigue was statistically significant (p=0.00 & p=0.00 respectively) while the work environment was not statistically significant (p=0.477). Self factors exposed nurses to compassion fatigue while work environment exposed medical practitioners to compassion fatigue while the risk factors for patients though statistically significant among the two populations, affected the two professionals almost equally (chart 1). The medical workers at
KNH were found to suffer from compassion fatigue in this study. Like other countries world wide, medical workers at KNH experienced compassion fatigue pattern similar to that found in other studies, particularly that on those who provided recovery and counselling services to the victims of the World trade Center attack victims on 11 th September, 2001 in New York 14 . In conclusion, the Kenyan medical workers as care-givers are no exception to the debilitating effects of compassion fatigue. The nursing career and middle college level of education were found to be risk factors. The sources of compassion fatigue were inherent self factors, parents and their relatives and their work environments for the medical practitioners and self factors and patients and their relatives for nurses. It therefore, means that the medical workers were progressively becoming less caring through loss of empathy for the patients. These findings therefore, justify a large scale study and the establishment of a rescue programme in Kenya to provide services for the medical workers suffering from compassion fatigue to the medical workers and other care-givers for the sustenance of better quality medical services in the country.
ACKNOWLEDGEMENTS
To the participants (medical workers at KNH), my co-authors, Professor C.R Figley, staff at
Mathari and Kenyatta National Hospitals, the Ministry of Health, Republic of Kenya, teaching staff at the Department of Psychiatry, University of Nairobi and my family.
10
REFERENCES
1. Schwab, L., (1996). Individual hardiness and staff satisfaction. Nursing economics, 14(3), May-June, pp 353-359.
2. Lee, R.T & Ashforth, B.E. (1990). On the meaning of Maslach’s Three Dimensions of
Burnout syndrome. J Appl Psychol 1990 Dec; 75(6): 743-7 (ISSN: 0021-9010).
3. Baranowsky, A.B. (In Press) (1997). The Silencing Response in Clinical Practice. On the road to dialogue. In C.R. Figley (Ed.), Compassion Fatigue: Volume II. New York:
Brunner/Mazel. Thirteenth Annual International Society For traumatic Stress studies
Conference, Queen Elizabeth Hotel, Montreal, QB, CAN, November 9, 1997.
4. Araki, Y; Muto, T & Asakura, T. (1999). Psychosomatic symptoms of Japanese working
Women and their need for stress management . Industrial Health (Japan) April 1999, 37; (2); p253-62.
5. Figley, C. R. (1995). Compassion fatigue as secondary traumatic stress disorder: An overview.
In C.R. Figley (Ed.) Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those
Who Treat the Traumatized (Pp. 1-20). New York: Brunner-Routledge.
6. Erasmus L.; Poggenpoel M. & Gmeiner A. (1998). Burnout Syndrome among Psychiatric
Nurses in a Private, Psychiatric Hospital. Curationis (South Africa) Jun 1998 21; p. 9-16.
7. Figley, C. R. (1995). Compassion fatigue as secondary traumatic stress disorder: An overview.
In C.R. Figley (Ed.) Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those
Who Treat the Traumatized (Pp. 1-20). New York: Brunner-Routledge.
8. Nelson-Gardell, D. & Harris, D. (2003). Childhood abuse history, secondary traumatic stress, and child welfare workers. Child Welfare, 82, 5-26.
9. Schauben, L. J., & Frazier, P. A. (1995). Vicarious trauma: the effects on female counselors working with sexual violence survivors. Psychology of Women Quarterly, 19, 49-64.
10. Figley, C. R. (2002a). Treating Compassion Fatigue. New York: Brunner-Routledge.
11. Figley, C. R. (2002b). Compassion fatigue: psychotherapists’ chronic lack of self care. Journal
of Clinical Psychology, 58, 1433-1441. Compassion Fatigue 18
12. Jenkins, S. R. & Baird, S. (2002). Secondary traumatic stress and vicarious trauma: a validation study. Journal of Traumatic Stress, 15, 423-432.
13. Kassam-Adams, N. (1999). The risks of treating sexual trauma: stress and secondary trauma in psychotherapists. In B.H. Stamm (Ed.) Secondary Traumatic Stress: Self-Care Issues for
Clinicians, Researchers, and Educators (pp. 37-48). Towson, MD: Sidran Institute.
14. Boscarino, J.A., Figley, C.R & Adams, R.E. (2004). Compassion Fatigue following the
September 11 Terrorist Attacks: A Study of Secondary Trauma among New York City Social
Workers. IJEMH • Vol. 6, No. 2 • 2004 1
11