surfactants
advertisement

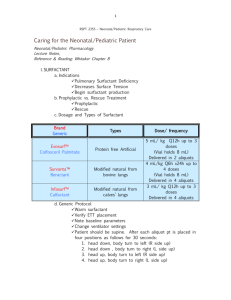
Surfactant Agents I. Definitions a. Surfactant: A surface-active agent that lowers surface tension i. Examples 1. soap 2. detergent b. Surface Tension: Force caused by attraction between like molecules that occurs at liquid-gas interfaces and that holds the liquid surface intact i. Units of Measure: dynes/centimeter (dyn/cm) 1. the force required to cause a 1 cm rupture in the surface film ii. a droplet forms because a liquid’s molecules are more attracted to each other than the surrounding gas c. LaPlace’s Law: Physical principle that describes and quantifies the relationship between the internal pressure, amount of surface tension and the radius of a drop or bubble i. In the alveoli where there is a single air-liquid interface, LaPlace’s Law is: Pressure=(2 x ST)/ r, where 1. ST = surface tension 2. r = radius of the alveoli II. Application to the Lung a. Increased surface tension can cause collapse or difficulty opening the alveoli i. Surfactant lowers the surface tension to decrease the pressure needed to open the alveoli b. In pulmonary edema, the surface tension of the liquid allows the formation of a bubbly froth i. Lowering the surface tension will cause the foam bubbles to collapse and liquefy III. Clinical Indications for Exogenous Surfactants a. Prophylactic Treatment i. Prevention of RDS in very-low-birth-weight infants and infants with higher birth weights who have evidence of immature lungs, at risk for developing RDS b. Rescue Treatment i. Retroactive or “rescue” treatment of infants who have developed RDS 1. the basic problem in RDS is lack of pulmonary surfactant as a result of lung immaturity 2. increased ventilating pressure is required to expand the alveoli during inspiration, which will lead to respiratory failure IV. Previous Surfactant Agents in Respiratory Care a. Ethyl alcohol i. Application 1. used for treating pulmonary edema 2. was given by nebulizer a. 3 - 5 ml. of 30 - 50% solution ii. Mode of Action 1. alcohol lowered the surface tension of the foamy exudate, reducing it to a liquid, clearable state iii. Disadvantages 1. efficacy not proven 2. toxic to membranes 3. better alternatives are available today b. Mucus Wetting Agents (Detergents) i. Examples 1. Alevaire 2. Tergamist ii. Indication 1. to improve water penetration and facilitate transport and expulsion of adhesive mucus iii. Mode of Action 1. these agents may interact with mucus to produce emulsification a. The mucus will dissolve or disperse into smaller molecules iv. Efficacy 1. efficacy in vivo is not proven c. Phospholipids i. Coating of the airway epithelium by phospholipids may serve as a lubricant for mucus transport ii. May offer another alternative to normalizing mucociliary transport and mucus clearing in disease states causing mucus hypersecretion or decreased clearance of secretions iii. There are no agents in general clinical use at this time V. Exogenous Surfactants a. Exogenous i. Originating outside the body 1. other humans 2. animals 3. laboratory synthesis b. Clinical Use i. to replace missing or immature surfactant in premature infants ii. investigated for use in adults with disease processes that have low surfactant (ARDS) c. History and Development of Exogenous Surfactants Year Event 1929 Von Meergaard showed that lungs were more difficult to inflate with air than with fluid 1956 Clements measured the surface tension of lung fluid extracts 1958 Dipalmitoylphosphatidylcholine (DPPC) is identified by Clements and associates as the main surface-active component of pulmonary surfactant 1959 Avery and Mead showed that surface tension is higher in the lungs of infants with hyaline membrane disease than in the lungs of normal infants 1964 Aerosols of synthetic DPPC are attempted in RDS, with little success 1972 Enhorning and Robertson demonstrate the effectiveness of surfactant replacement in premature animals 1980 Fujiwara and associates report success in exogenous surfactant therapy in infants, using “lyophilized artificial surfactant” (bovine extract, Surfactant TA) 1990 Colfosceril palmitate (Exosurf Neonatal, Burroughs Wellcome) approved for general use 1991 Beractant (Survanta, Ross Laboratories) approved for general use 1998 Calfactant (Infasurf, Forest Pharmaceuticals) approved for general use 1999 Poractant alfa (Curosurf, Dey Labs) approved for general use VI. Composition of Surfactant a. Lipids (85-90%) i. Phospholipids (~90%) 1. Phosphatidylcholine a. Dipalmitoylphosphatidylcholine (DPPC) i. most prominent in reducing surface tension 2. phosphotidylglycerol 3. phosphatidylethanolamine 4. phosphatidylserine 5. phosphatidylinositol 6. spingomyelin ii. Neutral Lipids (10%) 1. cholesterol and others b. Proteins (10%) i. Surfactant protein A (SP-A) 1. regulates secretion and reuptake of surfactant to Type II cell ii. Surfactant protein B (SP-B) 1. improves spreading of phospholipids in the alveolus iii. Surfactant protein C (SP-C) 1. improves spreading of phospholipids in the alveolus iv. Surfactant protein D (SP-D) 1. no clear role VII. Production and Regulation of Surfactant a. Production i. Synthesized in the type II alveolar cells ii. Stored in vesicles called lamellar bodies iii. Secreted by exocytosis into the alveolus iv. The major stimulus for secretion is inflation of the lung b. Regulation i. Endocytosis back into the type II cell 1. most surfactant (90-95%) is taken back into the type II cell, reprocessed, and resecreted a. this is the reason that exogenously administered surfactant is successful in replacing missing surfactant with one or two doses ii. Clearance/degradation by alveolar macrophages VIII. Others Benefits of Surfactant a. Contributes to host defense i. Increased bacterial killing ii. Modifies macrophage function iii. Down-regulates the inflammatory response 1. decreases mediator release iv. enhances ciliary beat frequency IX. Types of Exogenous Surfactant Preparations Category Natural Description Surfactant from natural sources (human or animal) with addition or removal of substances) Examples Survanta (bovine) Surfactant TA (bovine Curosurf (porcine) Infasurf (bovine) Alveofact (bovine) Synthetic Synthetic natural X. Surfactant that is prepared by mixing in vitro synthesized substances that may or may not be in natural surfactant Surfactant prepared in vitro with genetic engineering Exosurf ALEC None at present Specific Exogenous Surfactant Preparations a. Colfosceril palmitate (Exosurf Neonatal) i. Indications 1. Prophylactic therapy of infants weighing less than 1350g birth weight 2. Prophylactic therapy of infants with birth weights greater than 1350g with evidence of pulmonary immaturity and at risk for RDS 3. Rescue treatment of infants who have developed RDS ii. Dosage 1. 5 ml/kg of the reconstituted suspension q12° X 2 - 3 doses iii. Preparation 1. available as a dry powder that is reconstituted with 8 ml sterile water prior to use iv. Administration 1. instilled directly into the endotracheal tube through a side port adapter attached to ET tube, in 2 divided aliquots a. 1st half of dose in midline position i. infant rotated to the right and ventilated for 30 seconds nd b. 2 half of dose in midline position i. Infant rotated to the left and ventilated for 30 seconds 2. a single vial can treat up to a 1600 g infant a. 5 ml/kg x 1.6 kg = 8 ml b. Beractant (Survanta) i. Indications 1. Prophylactic therapy of premature infants less than 1250g birth weight or with evidence of surfactant deficiency and risk of RDS 2. Rescue treatment of infants with evidence of RDS ii. Dosage 1. 4 ml/kg (100 mg/kg) of the suspension q6° iii. Preparation 1. available as a vial containing 8 ml of suspension with 200 mg active ingredient (25 mg/ml) iv. Administration 1. instilled directly into the endotracheal tube through a 5French catheter, in 4 divided aliquots 2. the infant is placed in 4 different positions and manually or mechanically ventilated for 30 seconds 3. a single vial can treat up to a 2000 g infant a. 4 ml/kg x 2 kg = 8 ml v. Handling 1. keep refrigerated 2. warm at room air for at least 20 minutes prior to administration 3. unopened vial may be returned for refrigeration within 8 hours 4. used vials should be discarded c. Calfactant (Infasurf) i. Indications 1. The prevention of RDS in premature infants < 29 weeks of gestational age at high risk for RDS 2. Rescue treatment of premature infants less than or equal to 72 hours of age who develop RDS and require endotracheal intubation ii. Dosage 1. 3 mL/kg of the suspension q12 h up to 3 doses iii. Preparation 1. available as a vial containing 6 ml of suspension with 210 mg of active ingredient iv. Administration 1. Side-port adapter a. The dose in given in two aliquots i. Position the infant with either the right or left side dependent ii. Administer half the dose in small bursts to coincide with the inspiratory cycle, over 20 to 30 breaths iii. Reposition and administer the other half of the dose in the opposite position 2. Catheter a. The dose is given in four aliquots, with the catheter removed between each instillation b. Each portion is given with the infant in a different position i. Prone ii. Supine iii. Right lateral iv. Left lateral c. The infant is ventilated for 0.5 to 2 minutes between portions 3. a single vial can treat up to a 2000 g infant a. 3 ml/kg x 2 kg = 6 ml d. Poractant alfa (Curosurf) i. Indications 1. For the treatment or rescue of RDS in premature infants 2. Unlabeled Uses a. Prophylaxis for RDS b. ARDS resulting from viral pneumonia c. HIV-infected infants with Pneumocystis carinii pneumonia (PCP) d. ARDS after near-drowning ii. Dosage 1. 2.5 mL/kg 2. Repeat doses of 1.25 mL/kg birth weight q12h x 2 iii. Preparation 1. two preparations available a. a vial containing 1.5 ml of suspension containing 120 mg of active ingredient b. a vial containing 3.0 ml of suspension containing 240 mg of active ingredient iv. Administration 1. instilled directly into the endotracheal tube through a 5French catheter a. The dose is given in two aliquots i. Each portion is given with the infant in a different position 1. right side dependent 2. left side dependent ii. The catheter is removed between portions and the infant is manually ventilated with 100% O2 for 1 minute 2. a single 3.0 ml vial can treat up to a 1200 g infant a. 2.5 ml/kg x 1.2 kg = 3 ml XI. Mode of Action a. Exogenous surfactants replace and replenish a deficient endogenous surfactant pool in neonatal RDS i. Increased FRC 1. dramatic improvement in oxygenation XII. Hazards and Complications of Surfactant Therapy a. During instillation i. airway occlusion 1. relatively large volumes are instilled into the ETT ii. desaturation 1. impaired diffusion iii. bradycardia 1. heart rate < 100 bpm in a neonate a. normally 120-160 bpm 2. caused by hypoxia and vagal stimulation b. Post-instillation i. high arterial oxygen (PaO2) values 1. wean O2 to maintain PaO2 50-70 torr ii. over-ventilation and hypocarbia 1. decrease ventilating pressures as compliance improves to prevent barotraumas iii. apnea 1. irritation to the airway causes apnea in a neonate iv. pulmonary hemorrhage 1. factors that increase risk a. < 700 g birth weight b. younger c. male d. patent ductus arteriosus (PDA) XIII. Factors in Surfactant Selection Parameter Response time Administration Drug preparation Side effects Synthetic (Colfosceril) Slower in onset (several hours) During mechanic ventilator breath Must reconstitute before use No proteins to stimulate immune response; no infectious agents present Natural (Beractant) Rapid in onset (5-30 min) Removed from ventilator Refrigerated suspension; must warm prior to use Proteins may elicit immune response; concern over sterilization Cost Similar effectiveness Similar XIV. Benefits of Surfactant Therapy a. Improved survival in RDS b. Increased oxygenation c. Decreased days of ventilatory support and supplemental O2