Likely Finals Cases - Medics Without A Paddle
advertisement

Likely Finals Cases – based upon portfolio cases
1.1
1.2
1.3
1.4
1.5
1.6
1.7
A neonatal problem
Developmental delay
A congenital problem
Wheezy breathlessness
A gastrointestinal problem
Fits
Cerebral palsy
2.1
2.2
2.3
2.4
2.5
2.6
2.7
2.8
A normal pregnancy delivery and puerperium
Bleeding in pregnancy
An abnormality of fetal growth and development V
Pre-eclampsia
Medical disease complicating pregnancy V
Multiple pregnancy
Abnormal labour
A third stage abnormality V
3.1
3.2
3.3
3.4
3.5
3.6
3.7
3.8
3.9
3.10
3.11
3.12
3.13
3.14
3.15
3.17
Dysphagia
Chronic epigastric pain
Acute gastrointestinal haemorrhage
Jaundice
Hepatomegaly
Ascites
Chronic diarrhoea
Acute alteration in bowel habit / chronic constipation
Rectal bleeding
Acute generalised abdominal pain
Pain in the right iliac fossa
Lump in the groin
Insulin-dependent diabetes mellitus
Insulin-independent diabetes mellitus
A lump in the neck
Weight loss
4.1
4.2
4.3
4.4
4.5
4.6
4.7
4.8
4.9
4.10
4.11
Hip fracture
Colles' fracture
Multiple trauma
Open fracture
Bone or joint infection
Soft tissue injury
Burns requiring hospital admission
Chronic symmetrical polyarthritis
Acute monoarthritis
Low back pain
Chronic painful hip or knee V
5.1
Pre-operative assessment and post-operative management of a patient
undergoing a major surgical procedure with significant underlying disease.
Cardiopulmonary resuscitation V
A patient with shock. V
Acute poisoning
A patient with a pain control problem
5.2
5.3
5.4
5.5
6.1
6.2
6.3
6.4
Purpura V
Anaemia V
Haematological malignancy
Swollen painful leg (covered in 7.12)
7.1
7.2
7.3
7.4
7.5
7.6
7.7
7.8
7.9
7.10
7.11
7.12
Acute central chest pain
Chronic recurrent central chest pain
Left ventricular failure
Hypertension
Leg claudication
Recurrent wheezy breathlessness
Chronic cough
Progressive breathlessness
Acute pleuritic chest pain and fever
Weight loss and progressive breathlessness
Haemoptysis
Painful swollen leg
8.1
8.2
8.3
8.4
8.5
8.6
8.7
8.8
8.9
8.10
8.11
8.12
8.13
8.14
8.15
Haematuria or renal colic V
Chronic voiding difficulty or incontinence V
Proteinuria V
Recurrent urinary infection
Chronic renal failure V
Acute renal failure V
Testicular lump A
Abnormal menstruation V
Chronic pelvic pain in a woman V
Post menopausal bleeding V
Breast lump on routine screening V
Infertility A
Urogenital discharge A
Abnormal cervical smear A
Contraceptive needs A
9.1
9.2
9.3
Eczema
Psoriasis
Chronic lower leg ulceration
10.1
10.2
10.3
10.4
10.5
10.6
10.7
10.8
10.9
10.10
10.11
10.12
10.13
10.14
10.15
10.16
10.17
Chronic headache
Fits V
Sudden unilateral weakness V
Chronic movement disorder V
Sensory loss V
Chronic visual loss
Visual problems in a diabetic
Painful red eye
Progressive bilateral deafness A
Chronic nasal blockage V
Bleeding from the nose
Hoarse voice
Pain in the throat
Visual problems in childhood
Squint or amblyopia
Confusion
Disturbance of consciousness
11.1
11.2
11.3
11.4
Acute severe headache
Pyrexia of unknown origin
Jaundice
Acute diarrhoea
12.1
12.2
12.3
12.4
12.5
12.6
12.7
12.8
Depression
Anxiety state
Schizophrenia
Dementia
Substance abuse
A psychological reaction to a physical illness
A child with: A behavioural problem V
A child with: Learning difficulties A
13.1
13.2
13.3
13.4
13.5
13.6
13.7
An elderly person who has recurrent falls
An elderly person: Who has mobility difficulties
An elderly person: Who is incontinent V
An elderly person: Who needs to move into residential care
An elderly person: Who is confused
A younger person: with chronic disability
A patient who has incurable cancer
118 Cases – 8 per day = 15 days!!!
Action plan:
Read each entry in medicine at a glance and in MWAP – notes
List basic pathophysiology, investigations and management for each
List focussed history questions
List differentials where relevant
1.3 Congenital abnormality
Cardiac – non cyanotic
Innocent murmus
Ventricular septal defect
Atrial septal defect
Patent ductus arteriosus
Coarctation of the aorta
Cardiac - cyanotic
Tetralogy of Fallot
Great artery transposition
Non-cardiac
Left to right cardiac shunt
These can be caused by one of several factors
Congenital or acquired defect in the interatrial septum
Congenital or acquired defect in the interventricular septum
Patent ductus arteriosus
Blood follows the path of least resistance from left to right
Instead of both sides of the heart having an identical output, the right has to cope with extra that
the left would normally pump. A two-to-one shunt means the right side is pumping twice what the
left side is. Results include
Heart failure through increased workload
Pulmonary hypertension secondary to damage to lung blood vessel and high blood flow
through the lungs.
Atrial septal defects (ASD)
This is a persistant opening in the interatrial septum after birth. Occur about 1 in 1500 live births.
Most common site is the ostium secondum – caused by excessive absorption or incomplte
formation of septum primum.
Less common is a defect at the ostium primum caused by failure of septum primum to fuse
with the endocardial cushions – usually associated with abnormal A/V valve dev.
A sinus venosus ASD occurs when the sinus venosus is incompletely absorbed into the right
atrium.
Finally there is a patent foramen ovale – this is thought to occur in ~20% of people and is due to
failure of fibrosis – it is silent in most cases as the higher pressure in the left atrium keeps it
closed.
Ventricular septal defects (VSD)
This is an abnormal opening in the interventricular septum – it has an incidence of 1.5-3.5 per
1000 live births
70% are in the membranous part of the septum
20% are in the muscular part
The rest occur just below the aortic or adjacent to the A/V valves
If the shunt is large enough the RV, LV and pulmonary circulation experience a relative volume
overload – this may eventually lead to chamber dilatation, systolic dysfunction and symptoms of
heart failure.
Patent ductus arteriosus
This is the vessel that connects the left pulmonary artery to the ascending aorta during foetal life.
This ducta may fail to close after birth about once per 2500-5000 live births. Risk factors include
1st trimester rubella and birth at high altitudes.
Results in a leftright shunt (see above). The Pulmonary circulation, LA, LV and RA become
volume overloaded and left sided heart failure may follow.
Congenital aortic valve stenosis
Usually due to abnormal development of the aortic valve – it has two semilunar cusps instead of
three – it is 4x as common in males and 20% of patients have an additional abnormality, most
often coarctation of the aorta.
This is a common abnormality (2% live births) uncommonly causing morbidity in children
but commonly causing aortic stenosis in adults due to fibrosis and calcification of the leaflets.
The valvular orifice is narrowed resulting in a left ventricular pressure rise and left
ventricular hypertrophy with a possible result of left-sided heart failure.
Congenital pulmonary valve stenosis
This may occur at the level of the valve (>90% usually from fused valve commisures), within the
body of the RV (obstruction) or in pulmonary artery itself.
This results in increased pressure within the right ventricle and chamber hypertrophy with
a possible result of right-sided heart failure.
Coartctation of the aorta
This is typically a discrete narrowing of the aortic lumen
occurring 1 in 6000 live births, often with patients of the
Turner genotype (45, XO)
- 98% are post ductal – coarctation occurs after the
join between aorta and ductus arteriosus – possibly
due to ductus material infiltrating the aorta and
causing a stricture when the ductus closes in
response to a rise in O2.
- 2% are in which narrowing occurs proximal to the
ductus
As a result of either the LV faces an increased pressure
load. Left ventricular hypertrophy may develop dilatation
of compensating collateral arteries bypassing the
coarctation may develop – these may erode undersurface
of the ribs.
Cyanotic Lesions – these are abnormalities that result in
cyanosis (>4g/L deoxygenated blood, O2 saturation
~85%)
Tetralogy of Fallot
This arises from a single developmental defect – an
abnormal anterior and cephalad displacement of the
ventricular outflow part of septum. four anomalies are
characteristic.
- Ventricular septal defect (hollow arrow)
- Obstruction to right ventricular outflow from
infundibular septum (solid arrow)
- An overriding aorta – receives blood from both
ventricles
- Right ventricular hypertrophy due to high pressure
load on RV via pulmonary stenosis.
- The most common cyanotic congenital
abnormality seen after infancy.
- Ideally corrected by elective surgery at the age of
1 year.
Cyanotic spells:
placing the child with the knees against the chest
oxygen
morphine for analgesia
Beta-blockers may be used to reduce infundibular spasm
bicarbonate may be used to correct the acidosis
avoid agitating the child
Early surgery is indicated if there are hypercyanotic
attacks
Transposition of the great arteries
In this disorder the pulmonary artery and aorta arise from
the wrong sides: pulmonary artery from the left ventricle
and aorta from the right ventricle. This accounts for about
7% of congenital heart defects and is the most common
neonatal cyanotic heart disorder.
This disorder results in two systems (right and left)
running in parallel rather than one in series – deoxygenated
blood is pumped around the systemic circulation while
oxygenated blood goes round the pulmonary system –
without intervention this is incompatible with life post birth.
This is a medical emergency – immediate
treatment is by way of prostaglandins to maintain ductus
arteriosus and creation of an interatrial communication
using balloon catheter – this allows adequate mixing of the
circulations until elective surgery can be performed. The
latter involves transection and ‘swapping over’ of the great
arteries.
2.1
A pregnant woman
Possible differentials
Normal pregnancy
Multiple births
Breech presentation
Pre-eclampsia
Other medical problem
Assisted reproduction
(e.g. as a result of IVF)
Investigations:
Management:
Routine tests
Bloods:
Blood type and antibodies
FBC (for anaemia)
Hgb electrophoresis
(haemoglobinopathy
screen)
Rubella antibodies
Syphillis, HBV and HIV
antibodies
Imaging
12 week dating scan
20 week anomaly scan
Urinalysis + MSU
BP
Urine dipstick
Questions
Mnemonic: LEOPPARDS
Last menstrual period
Estimated due date
Obstetric history (this pregnancy)
Past pregnancies
Plans for this pregnancy
Assisted reproduction?
Rubella vaccination
Anti-D requirements (blood type)
Scans / tests
Blood pressure
Thyroid
Diabetes
Non-routine tests
Nuchal lucency
Amniocentesis
Chorionic villus sampling
Triple test
Quad test
AFP / triple / quad results
Result
Implication
AFP ? neural tube def
AFP ? Trisomy 21 /18
or other
hCG
chromosomal
Estriol
defect
Inh. A
Doppler / pinard
CTG
O/E remember:
Hands: swelling, pulse, BP
Face: Jaundice, anaemia, periorbital
oedema
Ankle oedema
Urine dipstick
Examination of the ‘gravid uterus’
Inspection: general distension, striae
gravidarum (white or red); linea nigra,
scars (esp LSCS), masses
Measure symphysio-fundal height
Palpation: No. of fetuses, lie, presentation,
engagement
Auscultation: with pinard or doppler
2.2
A bleed during pregnancy
<24 weeks
Cervix open
Inevitable miscarriage
(either complete or
incomplete)
Cervix closed
Ectopic pregnancy
Threatened miscarriage
Missed miscarriage
Investigations:
Management of miscarriage
ABC as needed
Psychological support and
reassurance / advice
Removal of retained
products as needed
Anti-D if >12 weeks
gestation and Rhesus +ve
in Rhesus –Ve mum
Antepartum haemorrhage 24 weeks +
Placental problems (50%):
Lower genital tract:
Placenta praevia
Cervical ectropion
Placental abruption
Cervical polyp
Vasa praevia
Cervical cancer
Cervicitis
Can also be ‘show’ marking
Vaginitis
the onset of labour
Vulval varicosities
CTG
Transvaginal ultrasound
Managemnt placenta praevia
ABC as needed
Admit for bed rest / IV
fluids if mild
LSCS if maternal risk or
fetal compromise
Usually LSCS at week 37
– dependent upon risk
Questions
Features of the History:
HPC
Onset: When did it start? Did anything
precipitate it (e.g. sex in cervical lesions,
RTA in placental abruption)
Character: How much blood? What colour
was it? Was there any mucus with it (think
of a show)?
Associated symptoms: the key symptom is
pain as PV bleeding + Abdominal pain in
second/third think placental abruption –
earlier may indicate ectopic preg. Ask
about fetal movements and symptoms of
hypovoaemia (faintness on standing, poor
urine output, palpitation, dizziness).
Past gynaecological History
Risk factors for praevia / abruption (see below)
Cervical smears
Mnemonic: LEOPARD
Last menstrual period
Estimated due date
Other pregnancies
Especially miscarriages & gest ages
Plans for this pregnancy
Rubella vaccination
Anti-D requirements (blood type)
Full blood count
Group & save / XM
Management of abruption
ABC as needed
Admit for bed rest / IV
fluids if mild
LSCS if maternal risk or
fetal compromise
O/E remember:
Hands: swelling, pulse, BP
Face: Jaundice, anaemia, periorbital
oedema
Ankle oedema
Urine dipstick
Examination of the ‘gravid uterus’
Inspection: general distension, striae
gravidarum (white or red); linea nigra,
scars (esp LSCS), masses
Measure symphysio-fundal height
Palpation: No. of fetuses, lie, presentation,
engagement
Auscultation: with pinard or Doppler
Speculum and vaginal
Once placenta praevia has been
excluded
Blood pressure / Thyroid / DM
Comparison of placenta praevia and abruption:
Placenta Praevia
Pain
Painless
Blood loss
Uterus
Fetal presentation
Risk factors
In proportion to vaginal loss
Soft, non-tender
May be malpresentation
Increased maternal age
Previous placenta praevia
Previous abortion
Previous LSCS
Multiparous
Multiple pregnancy
Uterine abnormalities (e.g. fibroids)
Smoking
Placental abruption
Painful (constant abdo pain /
contractions)
May be greater than vaginal loss
Tense, tender
Normal presentation
Increased maternal age
Previous placenta abruption
Maternal HTN
External cephalic version (ECV)
Multiparous
Multiple pregnancy
Uterine abnormalities (e.g. fibroids)
Smoking
Abdominal trauma
2.4
Pre-eclampsia
Risk factors
Increased maternal age
Afro-Caribbean
Primiparous
Multiple pregnancy
Obesity
Essential HTN
Chronic renal disease
DM
Collagen vascular disease
Previous PET
FH of PET
Investigations:
Symptoms
Can be asymptomatic
Symptoms may include:
Headache
Visual disturbance
(flashing lights)
RUQ/epigastric pain (due
to liver capsule swelling)
Facial swelling
Rarely the first
presentation is with fitting
Differentials
Chronic hypertension
Chronic renal disease
Gallbladder and
pancreatic disease
Immune or thrombotic
thrombocytopenic purpura
Haemolytic uraemic
syndrome
Ultrasound fetus
CTG / Doppler
Management:
Monitor fetal health (CTG /
fetal movement chart)
Admit as necessary
Delivery (± steroids as
required)
Blood pressure
Dipstick / 24 hr protein
FBC / U+E / LFTs /
clotting factors
Treat hypertension
(methyldopa or CCB /
labetalol) ACE I contraind.
Monitor maternal health
(as in diagnosis box)
Diagnosis is based on: BURPP
BP>160/110mmHg on 2 occasions
U+E’s: raised creatinine
Raised ALT/AST, deranged clotting factors
(hepatitic picture)
Protein (urinary) >300mg/24hours
Platelets low
Differential for eclampsia
primary seizure disorders
O/E remember:
High BP
Facial oedema
Confusion (severe PET)
Hyperreflexia and clonus
Papilloedema
SFD uterine size/fundal symphysis height.
Foetal Doppler / Cardiotocography (CTG)
Pathogenesis:
Not fully understood yet.
What is known is that problem is fundamentally poor placental perfusion. It is thought this poor placental
perfusion may either be due to a problem with trophoblast implantation and/or due to maternal microvascular
disease, but whatever the cause, the blueprint for pre-eclampsia is set early in pregnancy.
The lack of placental perfusion leads to the release of vasoconstrictors such as thromboxane, a relative lack
of vasodilators such as prostacyclin and women with PET sem to be more sensitive to vasoconstrictors in
general.
This creates a high pressure system and in the placenta this damages the endothelium to cause
microthrombi of trophoblastic tissue, which in turn leads to increased coagulation and also precipitate endorgan damage.
This end organ damage includes:
CVS: High TPR leads eventually to LVF, which in turn causes pulmonary oedema and ARDS.
Kidneys: There is swelling of glomerular endothelial cells which blocks the capillaries and leads to leakiness
of the kidneys which manifests as proteinuria and reduced renal function
Liver: Fibrin deposits accumulate in the liver and this causes hepatocellular damage, which can result in
DIC. The liver becomes distended and sub-capsular hemorrhage can also occur.
Increased cerebral vascular resistance leads to visual disturbance, headache, eclampsia and increased risk
of CVA.
Placenta: High resistance and poor perfusion leads to oligohydramnios and IUGR.
-
Eclampsia:
This is defined as 1 or more generalized seizures or coma in the setting of pre-eclampsia and in
the absence of any other neurological condition.
The seizures are grand mal in nature and are self-limiting
Management involves:
Place the woman in the recovery position
Secure the airway
Treat the fit with magnesium sulphate
Continue magnesium suphate as prophylaxis against further fits and used iv hydralazine to
reduce bp.
CTG to assess baby.
Once mum and baby stable, deliver.
2.6
Multiple pregnancy
Definition: A pregnancy where 2 or more fetuses are present.
Normally diagnosed at the booking scan, but consider it any patient presenting with hyperemesis
gravidarum (more fetuses more HCG more emesis)
Examination reveals LFD uterus and in later pregnancy, multiple foetal parts/poles.
Differentials for multiple pregnancy:
Big baby
Poorly baby
Elevated gestational age:
Polyhydramnios: e.g. DM,
Foetus may be larger than
foetal abnormality of
expected rather than
swallowing
multiple
Macrosomy: e.g. DM
Investigations:
(for diagnosis)
Management:
Not a baby
Tumours / fibromas:
Causes distension without
other signs of pregnancy
Molar pregnancy: Also
causes hyperemesis
gravidarum but without
distension
Fasting blood glucose
-HGG pregnancy test
Ultrasound scan
Early diagnosis. Consider selective foetal reduction in
higher-order multiple pregnancies. Statistically, benefit
outweighs risk with quadruplets and above. The situation
with triplets is controversial.
Shared care between hospital and community.
Hb should be regularly monitored and a low threshold for
iron and folic acid supplementation should be held as
women with multiple pregnancies are more at risk of
anaemia.
16 week AFP available for twins and 20 week anomaly scan
+ detailed cardiac scan at 22-24 weeks
Weekly CTG monitoring from 24 weeks
Serial growth scans every 2-4 weeks after 28 weeks
gestation.
Questions:
LEOPARD (see 2.1)
Risk factors include
FH (non-identical only – monozygous
twins do not run in families)
ART (artificial reproductive technologies –
e.g. IVF)
Multiparity
Race (black > white > Asian)
Increasing maternal age
Maternal complications
Anaemia
Hyperemesis gravidarum
Gestational diabetes
PET/Pregnancy induced hypertension
Polyhydaramnios
APH / PPH
O/E remember:
Hands: swelling, pulse, BP
Face: Jaundice, anaemia, periorbital oedema
Ankle oedema
Urine dipstick
Examination of the ‘gravid uterus’
Inspection: general distension, striae
gravidarum (white or red); linea nigra, scars
(esp LSCS), masses
Measure symphysio-fundal height
Palpation: No. of fetuses, lie, presentation,
engagement
Auscultation: with pinard or doppler
Foetal complications
Weakening of contraction after first birth;
abnormal position of 2nd twin.
IUD/Perinatal death
Preterm labour (30%)
IUGR / growth discordance
Congenital abnormalities (2x risk)
PROM
Twin-twin transfusion syndrome.
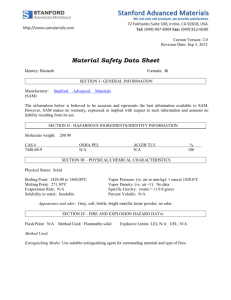
Background Box:
The most common multiple pregnancy is twin (98% of multiple pregnancy), which has an incidence of 1
in 80 pregnancies. Triplets occurs ~1 in 802 pregnancies and quadruplets/higher is ~1 in 80 3
pregnancies. The incidence of multiple pregnancy has increased over the last 20 year due to ART.
The majority of twins are dizygotic (75-80%), where there is fertilization of two ova by two sperm. 2025% are monozygotic where there is fertilization of a single ovum by a single sperm which then
completely divides to give identical twins.
Clinically, it is actually the chorionicity of the
pregnancy which is important – this refers to
arrangement of membranes in multiple
pregnancies. It is determined by the timing of
cell division after fertilization.
Dizygotic twins have dichorionic diamniotic
placentation i.e. each fetus has its own chorion,
amnion and placenta and thus each fetus has its
own blood supply (top).
Monozygotic twins can have a variety of
chorionicity. Most are monochrorionic
diamniotic (i.e. a single placenta, but separate
amnions – middle), approximately 1/3 are
dichorionic, diamniotic, and very few are
monochrorionic, monoamniotic (shared placenta
and membranes - bottom). With monochorionic
diamnitoic and monochorionic monoamniotic
twins there is a risk that there is uneven
distribution of blood (twin-twin transfusion)
between fetuses and thus discordant growth.
This can be treated by laser photocoagulation of
the abnormal vessels.
Chorionicity can be diagnosed by USS usually
at the 12 week scan, at the same time twin
pregnancies are usually diagnosed. It can also
be diagnosed antenatally by examination of
membranes (macro and microscopic)
NB: a familial history of dizygotic twins
predisposes to further dizygotic twins – FH
of monozygotic twins is irrelevant.
3.1
Dysphagia
Common
Oesophagitis and peptic
stricture
Neuro e.g. post CVA
Oesophageal ca.
Gastric ca at cardia
Globus
Investigations:
Management:
Occasional
Diffuse oesophageal
spasm
Extrinsic compression e.g.
LN, lymphoma, lung ca.
Plummer Vinson syndr
Chest X-ray
Barium swallow
Balloon dilatatation of
stricture
Physiotherapy ± thickened
fluids (CVA)
Questions:
Weight loss / anorexia
Solids or liquids and if both, which is worse
Reflux: bad taste in mornings, epigast pain
Reynauds (scleroderma)
Globus (stress)
Rare
Achalasia
Neuro e.g. motor neurone
/ progressive supranuclear
palsy
Scleroderma /
dermatomyositis
Endoscopy ± biopsy
Manometry + pH
Botulinum into LOS
(achalasia)
Parenteral feeding
Surgery
O/E remember:
Supraclavicular LN
Signs of iron deficiency (Plummer Vinson)
Neck lumps (?thyroid)
Fatiguability, double vision (MG)
Causes of obstruction:
Inside oesophageal lumen: Foreign body (e.g. false teeth!), tumour, scleroderma
Within wall: stricture, achalasia
Outside oesophagus: lymphoma, Lung cancer
An alternative way of remembering them
Motor causes: achalasia
Mechanical causes: tumour, stricture or foreign body.
Neurological: bulbar palsy, myasthenia gravis, MND, PD, CVA
Achalasia is a disease in which there is a loss of peristalsis in the oesophagus and a loss of
the ability of the lower oesophageal sphincter to relax to let food into the stomach. It is
diagnosed by a barium swallow.
The cause of achalasia is damage to the myenteric plexus – a nerve plexus running between the
longitudinal and circular layers of muscle in the oesophagus.
Plummer Vinson syndrome is the formation of an oesophageal web above the aortic arch in
association with concomitant iron deficiency in women. Sometimes there may be chronic atrophic
glossitis, koilonychia, angular stomatitis and achlorhydria. The main complaint is of dysphagia.
The phases of Swallowing:
Oral
Bolus molding
Pharyngeal
Glottis closes
Larynx elevates
Food is deposited into the
oesophagus
The nerves involved in swallowing are:
CN IX (glossopharyngeal)
Oesophageal
Peristaltic wave takes
bolus downward
Glottis opens
CN X (vagus)
CN XII (hypoglossal)
Brief anatomy of the oesophagus:
There are four layers from lumen outwards
Mucosa – stratified squamous epithelium
Submucosa
Muscle: the upper third is skeletal muscle, the lower third is smooth muscle and the middle third is
mixed. There are two layers of skeletal muscle – one is arranged circumferentially and one is
longitudinal.
Adventitia
The narrowest part of the oesophagus are as the pharynx becomes the oesophagus and as the
oesophagus enters the stomach.
Anteriorly lie the left bronchus, trachea and arch of the aorta.
Another cause of dysphagia is oesophageal atresia – failure of the oesophagus to recanalise in
foetal development.
3.4
Jaundice
LFT Results
Bilirubin (total)
ALT
AST
ALP
GT
Albumin
Total protein
Acute
Chronic
Investigations:
Management:
Hepatitic
N/
N/
N
N/
N/
Cholestatic
N/
N/
N/
N/
Hepatitic
Viral: HBAV, HBV, HCV,
EBV
Drug reaction
Budd-Chiari syndrome
Alcoholic liver disease
Hepatitis B / C
Autoimmune hepatitis
Haemochromatosis
LFTs + gamma GT
Viral Hepatitis serology
Ultrasound abdomen
Of cause
Questions:
Weight loss / anorexia
Stool / urine colour
Bleeding / bruising / itching
Has there been preceding illness
Alcohol
Infection risk factors: IVDU, sexual history,
tattoos, transfusions, foreign travel
Mixed
/
N/
N/
/N
/N
N/
N/
Cholestatic
Gallstones
Ca. head of pancreas
Pancreatitis
Secondary biliary disease
Primary biliary cirrhosis
Primary sclerosing
cholangitis
ERCP / MRCP (for
cholestatic)
Biopsy (hepatitic)
O/E remember:
Features of hepatic failure
Palmar erythema / dupuytren’s
Spider naevae / gynaecomastia
Encephalopathy
Features of portal hypertension
Ascites
Splenomegaly
3.5
Associated pain (gall stone)
PMH: IBD (assoc PBC); DM (NASH)
FH wilsons, 1 antitrypsin
Caput medusa / dilated superficial veins
Hepatomegaly
Cirrhosis
Early
Generally regular surface
No jaundice
Late
Generally irregular surface
With jaundice
Investigations:
Remember jaundice
Management:
Cardiac failure
Generally regular
No jaundice
Tense, tender liver
Peripheral oedema
Increased JVP
Secondary metastases
Generally irregular
No jaundice
LFTs + Gamma GT & PT
Abdominal ultrasound
AXR / CXR
Of cause
CT / MRI abdo / pelvis
AFP (hepatoma) / CA125
(ovarian ca)
Laparoscopy
Other causes: hepatitis, other infection, sarcoid, haemochromatosis, fatty liver, (NASH), Riedels
lobe, biliary tract disease, abscess
Questions:
Weight loss / anorexia
Risk factors for liver disease (alcohol,
IVDU, transfusions, tattoos)
Risk factors for heart failure
Family history ca.
3.6
O/E remember:
Signs of heart failure
Signs of portal hypertension (3.6)
Jaundice
Axillary / inguinal LN
Smooth / knobbly; tender / pulsatile (TR) /
bruit
Ascites
Ascites is the accumulation of excess free fluid in the peritoneal cavity
Transudate vs Exudate: A transudate contains <25 g/L protein while an exudate contains >25
g/L protein. The distinction is clinically useful as the two have largely different causes (see
below).
Transudate
Hepatic failure (alcohol,
viral)
Renal failure
Cardiac failure
Investigations:
Remember splenomegaly and
signs of CCF in examination
Portal Hypertension (Clinical
features)
Hepato/speno megaly
Caput medusae
Dilated superficial veins
LFTs + Gamma GT & PT
Paracentesis protein,
WCC, cytology, culture.
Abdominal ultrasound
U+E / urine dipstick
Exudate
malignant disease
pyogenic infection
pancreatitis
lymphoedema
Hypothyroid
tuberculosis
Biopsy
AXR / CXR
Amylase
AFP (hepatoma) / CA125
(ovarian ca)
Management:
Shunt if portal HTN
Transudate: diuretics, fluid
/ salt restriction,
therapeutic paracentesis
Questions:
Weight loss / anorexia
Risk factors for liver disease (alcohol,
transfusions, tattoos)
Shortness of breath (affect on lungs)
PMH: PBS, PSC,
Exudate: Antibiotics if req,
treat underlying malign,
therapeutic paracentesis
O/E remember:
Lung bases for crackles
Signs of portal hypertension (above)
Leg oedema / JVP
Axillary / inguinal LN
Insert table of normal values for ascitic fluid
Cirrhosis
‘A diffuse process characterised by fibrosis and nodular regeneration’
Fibrosis interferes with the vascular architecture resulting in a haphazard blood flow – the end
result is an inefficient liver prone to failure.
Causes include: alcohol, hepatitis B & C viruses, gallstones and an overload of iron
(haemochromatosis).
Portal hypertension
A rise in pressure within the portal vein and its tributaries.
Resultant from increased resistance to portal blood flow caused by cirrhosis: perisinusoidal
collagen deposition, perivenular fibrosis, expansion of nodules
Portasystemic anastamoses
Communications between the portal veins and the systemic veins – these become important in
portal hypertension
Between systemic and portal veins
oesophageal vein and left gastric vein
Oesophageal varices*
rectal/inferior rectal veins and superior rectal vein
Haemorroids
small epigastric v of anterior abdo wall and paraumbilical
Caput medusae
*Bleeding from this site may occur through the rupture of delicate engorged vessels by eating –
this may result in haematemesis, melaena or death.
Other results of portal hypertension:
Splenomegaly (via back pressure). Hypersplenism is common resulting in increased erythrocyte
destruction (and macrocytic anaemia)
Encephalopathy (toxins, especially ammonia, are being routed around the liver and so are not
being detoxified before reaching the brain). Symptoms include tremors, behaviour change,
delirium, drowsiness and coma as well as a ‘liver flap’. Can be treated by a low protein diet
(causes kwashoirkow through low production of albumin).
Treatment of portal hyperstension
A portacaval anastomosis or portastsytemic shunt can be created surgically – links the portal
vein to the inferior vena cava where they pass close together behind the liver.
3.7
Chronic diarrhoea
Common
IBS
Diverticulitis
Occasional
IBD (Crohns / UC)
Neoplasia
Rare
Thyrotoxicosis
Coeliac (or other
Overflow (esp elderly)
In children:
Toddlers diarrhoea
Investigations:
Don’t forget the PR exam!
Management:
Lactose intolerance
Chronic infection
Hookworm
Giardiasis
Amoebiasis
Excess alcohol
Abdo X-ray
Stool culture (x3) / micro
TTG (coeliac)
Thyroid function tests
Of cause
ESR / CRP
Colonoscopy ± biopsy
USS abdo (pancreas)
MRI abdo
Of IBS
Questions:
Normal bowel habits and last opening
Weight loss / anorexia
Mouth ulcers
Frequency / urgency / woken at night by
need to defacate?
Tenesmus
Stool consistency / amount / odor / flushing
Blood / mucus
Bloating / relation to stress
Foreign travel
PMH: CF, coeliac, addisons
3.8
malabsorption e.g. sprue)
Laxative misuse
Antispasmodic drugs for
colicky pain e.g. mebeverine
Anticholinergics for
depressive features e.g.
amytriptaline
O/E remember:
Signs of malabsorption: koilonychia,
leukonychia, glossitis, ulcers, bruising
PR exam
JVP – fluid levels
Constipation / change in bowel habits
S
Straining 25%
Common
Diet / lifestyle
Inactivity (esp elderly)
IBS
Painful perianal disease
- Fissure
- Haemorrhoids
- Abscess
- Florid warts
Drugs (e.g. opiates,
antidepressants)
Pregnancy
Investigations:
Remember to check drugs
Investigate if a new
symptom in >40 yr olds
Management:
H
Hard
I
Incomplete evac
T
<two times per week
Occasional
Poor fluid intake
Diverticulosis
Hypothyroidism
Hypercalcaemia
Ca. colon / rectum
Acquired megacolon
- laxative abuse
- scleroderma
- neuro problems
Rare
Crohns + stricture
Acute obstruction
Mass outside bowel
Hirschsprungs disease
Transit studies
Thyroid function tests
Serum calcium
Of Cause
Faecal occult blood
Abdo X-ray
Barium enema
Colonoscopy ± biopsy
Dietary review
Review of drugs
Questions:
Weight loss / anorexia
Nocturnal diarrhoea / pain
Rectal bleeding
3.9
O/E remember:
PR examination
Organomegaly
Masses
Lymphadenopathy
Rectal bleeding
Common
Haemmorrhoids
Anal fissure
Gastroenteritis
Rectal carcinoma
Diverticular disease
Investigations:
Remember to do PR exam
Management:
Occasional
IBD
Anticoagulant therapy
Colonic carcinoma
Trauma (inc NAI)
Villous adenoma
Full blood cnt (WCC/Hb)
ESR / CRP
Barium enema
Of cause
In emergency scenario
remember ABC
Questions:
Weight loss / anorexia
Mouth ulcers, rashes
Pain with defacation
Familial history of colonic neoplasia
Alcohol (varices)
3.12
Rare
Blood clotting disorders
Ischaemia
Intussusception (red jelly)
Meckels (in children)
Angiodysplasia
Sigmoid / colonoscopy
Abdo X-ray
Clotting factors
Of Haemorrhoids
Diet / defacation advice
Injection sclerotherapy
Banding
Excision
O/E remember:
PR exam
Organomegaly / masses
telangiectasia
Lump in the groin
Inguinal
Above and medial to pubic tubercle
Direct inguinal hernia
Indirect inguinal hernia
Undescended testis
Cordal hydrocoele
Lipoma
Investigations:
Management:
Questions:
Occupation
Pain
Femoral
Below and lateral to pubic tubercle
Lymphadenopathy
Femoral hernia
Saphena varix
Femoral artery aneurysm
Psoas abscess
Femoral neuroma
FBC (WCC for LN)
CT (psoas abscess)
Ultrasound of area
Herniography
Of cause
Usually surgical
O/E remember:
Standing and lying
Locate the mass relative to the pubic
Congenital
Fever / temp (infective)
Reducibility
Symptoms of strangulation (flatus)
tubercle – is it above / below; med / lateral
Does the mass extend into the scrotum
Reducibility
Cough impulse
Expansility
Does it transilluminate
Anatomy of Inguinal hernias
The inguinal canal lies parallel to and superior to the medial part
of the inguinal ligament. It contains blood vessels and lymphatic
vessels as well as the ileiolingual nerve and the spermatic cord (in
males) or round ligament (in females).
The deep inguinal ring is the site of an outpouching of
transversalis fascia 1.25 cm superior to middle of inguinal ligament
and lateral to the inferior epigastric artery.
The superficial inguinal ring is a slit-like opening between
diagonal fibres of the external oblique. Superolateral to pubic
tubercle.
The inguinal canal has two walls, a roof and a floor:
Anterior wall: mainly aponeurosis of external oblique. Lateral part
reinforced by fibres of internal oblique.
Posterior wall: Mainly by transversalis fascia – medial part
reinforced by conjoint tendon. This is the merging of the pubic
attachments of internal oblique and tranversus abdominis
aponeurosis into a common tendon
Roof: arching fibres of internal oblique and transversus abdominis.
Floor: superior surface of in-curving inguinal ligament
Anatomy of Femoral hernias
These are protrusion of viscera through the
femoral ring and into the femoral canal – the
canal is the passageway by which femoral
structures exit from the abdomen into the upper
thigh. Its boundaries are:
anteriorly: inguinal ligament
medially: pubic bone and lacunar ligament
laterally: iliopsoas muscle
posteriorly: pubic ramus and pectineus muscle
The femoral canal is divided into two
compartments by the medial border of the femoral vein. The medial compartment is the femoral
ring.
Medial (femoral ring) contents
Cloquet's node
lymphatics.
Lateral compartment contents
femoral vein
femoral nerve
femoral artery
genitofemoral nerve
From the canal, the hernial contents may progress through the sapphenous opening into the
loose connective tissue of the thigh allowing it to become much larger though it cannot travel
downwards due to the fascia lata of the thigh.
3.15
Neck Lump
http://www.med.mun.ca/anatomyts/head/hnl1.htm
There are many differentials for neck lump – these can
be narrowed down by considering the anatomical area
in which they arise (see fig 7) Some lumps such as
sebaceous cysts or lymph nodes are found in many
areas and are considered later.
Posterior triangle borders: posterior sternomastoid,
clavicle, and anterior border of trapezius)
QuickTime™ and a
TIFF (Uncompressed) decompressor
are needed to see this picture.
Anterior triangle borders: anterior sternomastoid, jaw
line, midline.
Sebaceous cysts
Face, trunk, neck and scalp
50% have a central ‘punctum’
Attached to the skin
Lymph nodes
These are the commonest of all neck lumps – the
anatomy of lymph nodes is well characterised and they should be easy to identify.
Posterior triangle
Under sternocleidomastoid
Anterior triangle
Midline
Investigations:
Management:
Questions:
Weight loss / anorexia
Functional thyroid symptoms
Regurgitation of food (pouch)
3.17
Weight Loss
Cervical lymph node: LIST: Lymphoma / Leukaemia,
Infection (e.g. TB), sarcoid, Tumours
Cystic hygroma: more common in paediatrics. Brilliantly
transilluminable, lobulated, soft, fluctuant, compressible.
Pharyngeal pouch
Sebaceous cyst (see above)
Branchial cyst
Sternomastoid tumour
Cervical lymph node: LIST: Lymphoma / Leukaemia,
Infection (e.g. TB), sarcoid, Tumours
Branchial cyst
Sebaceous cyst (see above)
Thyroid goitre: moves upon swallowing
Thyroglossal cyst: moves upon swallowing AND upon
protruding the tongue.
Dermoid cyst
Sebaceous cyst (see above)
Fine needle aspiration
Chest X-ray
Ultrasound neck
Laryngoscopy
Bronchoscopy
Of cause
Usually surgical
O/E remember:
Examine oral cavity
With anorexia
Malignanacy
Psych (dementia /
depression)
Organ failure
Systemic infect. (TB / HIV)
Inflammatory bowel dis
Investigations:
Management:
With or without anorexia
Rheumatoid arthritis
Systemic lupus
erythematosus
Vasculitis
Without anorexia
Malabsorption
Hyperthyroidism
Diabetes
Chest X-ray
Abdo / pelvic ultrasound
Endoscopy ± biopsy
Nutritional assessment
Psychiatric evaluation
Treat underlying cause
?dietary supplements
Questions:
Quantify weight loss and time span
Is the appetite normal or decreased
Mood / anhedonia / sleep loss
Smoking / occupational history
Alcohol use
Change in bowel habit / blood
Fever / night sweats / headache
Symptoms of DM / thyrotoxicosis
HIV risk factors / travel history
Periods (anorexia nervosa)
Attitudes to food
U+E & LFTs for failure
CT / MRI chest / abdo
HIV test (counselling req)
Empirical steroids if
inflamm markers
Empirical anti-TB if
symptoms suggest
O/E remember:
Fever
Signs of organ failure – heart, liver, kidney
Signs of thyroid disease
Signs of malnutrion (koilonychias, angular
stomatitis, glossitis, scurvy, pellagra)
Lymphadenopathy (esp Virchov’s node)
Thyroid examination
Breast examination
Pellagra is a deficiency disease caused by lack of thiamine and protein (especially tryptophan).
The main results of pellagra can easily be remembered as "the four D's": diarrhoea, dermatitis,
dementia, and death.
Scurvy is a disease due to deficiency of ascorbic acid - vitamin C - and is characterised by
anaemia, spongy gums, a tendency to mucocutaneous haemorrhages, and brawny induration of
calf and leg muscles.
3.10
Acute abdominal pain
It is important to differentiate between localised and generalised
Localised peritonitis occurs with all acute inflammatory conditions of the GI tracts (e.g.
appendicitis, cholycystitis). The features are local pain and tenderness. Treatment is for the
underlying condition.
Generalised peritonitis is much more serious and arises from irritation of the peritoneum as a
result of infection (e.g. perforated appendix) or chemical irritation due to leakage of intestinal
contents (e.g. perforated ulcer) In the latter a superadded infection may occur as a sequel.
The peritoneal cavity becomes inflamed with production of an inflammatory exudates that
spreads throughout the peritoneum and leads to intestinal dilatation and paralytic ileus.
In perforation
Sudden onset
General collapse and shock
May be a transient improvement becoming
worse with generalised toxaemia
Secondary to inflammatory disease
Less rapid onset
Initial features are those of underlying
disease
Investigations
CXR (erect) to detect free air under
diaphragm
Serum amlase (acute pancreatitis)
USS or CT for diagnosis
Management
Resuscitation inc good urinary output,
nasogastric tube
IV fluids
antibiotics
Peritoneal lavage of abdo cavity
Treatment of underlying cause
Complications include: toxaemia, septicaemia, local abscess formation. Suspect the latter if
patient remains unwell with swinging fever and WCC + continuing pain.
Localised abdominal Pain
RUQ
Pneumonia
Pancreatitis
Hepatic tumour / abscess
Hepatitis
Pyelonephritis
Renal infarct
Renal colic
Retrocaecal appendicitis
Right iliac fossa
Ectopic pregnancy
Appendicitis
Meckels diverticulitis
Ovarian cyst torsion
Salpingitis
Renal colic
Urinary tract infection
Epigastric
Oesophagitis
Pancreatitis
Gastritis
Gastric ulcer
Peptic ulcer
Umbilical
Aortic aneurysm
Meckels diverticulitis
Bowel obstruction
Intussusception
Bowel infarct
Crohn’s disease
Enteritis
Suprapubic
Pelvic appendicitis
Diverticulitis
Ovarian cyst torsion
Salpingitis
Cystitis
Uterine fibroid
LUQ
Pneumonia
Pancreatitis
Splenic infarct
Pyelonephritis
Renal infarct
Renal colic
Left iliac fossa
Ectopic pregnancy
Diverticulitis
Sigmoid volvulus
Ovarian cyst torsion
Salpingitis
Renal colic
Urinary tract infection
A mnemonic for the organs / systems involved is BLAG PLUS
B
L
A
G
P
Bowel
Liver
Aorta
Gynae
Pancreas
L
Lung
U
Urinary
S
Spleen
Acute pancreatitis
Common Presentation
A steady, ‘boring’ pain, mild – severe, epigastric /
periumbilical radiating through to the back. May affect
chest, flanks and lower abdo.
Pain worse with food, alcohol or when lying supine
N&V, abdominal distension, fever possible
Hypoxaemia possible – dyspnoea
Hypotension / tachycardia - hypovolaemia (fluid in abdo)
Common causes: I GET
SmasHeD (uncommon ones
not listed)
Idiopathic
Gallstones
Alcohol abuse
Trauma
Steroids
Mumps / other viral
Hyperlipidaemia
Diuretics
Investigations
FBC, U+E, LFT (bilirubin)
Serum amylase (ideally within 24 hrs – levels drop over 3-5
days)
Urine amylase (levels elevated longer)
Blood glucose
Arterial blood gas.
AXR, CXR (excludes peptic ulcer perforation)
USS
Contrast enhanced CT
MRCP
Indicating poor prognosis (3 or
more from PANCREAS)
Pa02: <8 kPa
Age > 55
Neutrphils (WBC: >15^9/L)
Calcium <2
Renal (serum urea: >16
mmol/L)
Enzymes (AST: >200 U/L,
LDH: >600 U/L)
Albumin <32 g/L
Sugars (BM> 10)
Management: The most at-risk cases should be transferred to HDU or ITU.
Oxygen
Cannulate for IV access
Catheterise
Fluid balance with fluid replacement as needed.
Nasogastric suction to prevent aspiration
Prophylactic antibiotics: cefuroxime (cehalosporin) or imipenem (carbapenem) (broad spectrum
lactam antibiotics)
Analgesia – tramadol or pethidine (opioids).
Feeding via nasojejunal tube
CT at seven days to assess necrosis
Removal of gallstones if appropriate
Surgical resection of necrotic pancreas as appropriate (CRP, WCC)
Drainage of peripancreatic cysts if required after 6 weeks.
Mnemonic: AEIOU; Analgesia, / antibiotics, ERCP, Investigations, Oxygen, Urine
(catheterise + keep up with fluids)
Bowel obstruction
Intestinal obstruction involves a partial or complete blockage of the bowel that results in the
failure of the intestinal contents to pass through.
Obstruction of the bowel may be caused by ileus -- in which the bowel doesn't function correctly
but there is no "mechanical" (anatomic) problem -- or by mechanical causes. Paralytic ileus, also
called pseudo-obstruction, is one of the major causes of obstruction in infants and children.
The causes of paralytic ileus may include the following:
Intra-abdominal surgery
Medications, especially narcotics
Intraperitoneal infection
Mesenteric ischemia (decreased blood supply to the support structures in the abdomen)
Injury to the abdominal blood supply
Kidney or thoracic disease
Metabolic disturbances (such as decreased potassium levels)
Paralytic ileus may lead to complications causing jaundice and electrolyte imbalances. In the
newborn, paralytic ileus that is associated with destruction of the bowel wall (necrotizing
enterocolitis) is life-threatening and may lead to infection in the infant's blood and lungs.
In older children, gastroenteritis may be a cause of paralytic ileus, which is sometimes associated
with peritonitis and a ruptured appendix. Paralytic ileus is marked by:
Abdominal distention
Absent bowel sounds
Relatively little pain (as compared to mechanical obstruction)
Mechanical obstruction occurs when movement of material through the intestines is physically
blocked. The mechanical causes of obstruction are numerous and may include the following:
In the lumen
Faeces
Meconium
Gallstone
Foreign Body
In the wall
Tumour (common)
Stricture (common)
Diverticulae
Ischaemia
Crohns
Intussusception
Outside the wall
Adhesions (v common)
Hernia (v common)
Volvulus
Lymphoma / nodes
Signs
Dehydration
Oliguria
Distended
Tympanitic
bowel sounds
Visible peristalsis
Septic / toxic
Symptoms
Vomiting
Distension
Bowel wall becomes oedematous – fluids and electrolytes accumulate in
the wall and lumen. This is third space loss of fluids.
Due to dehydration
Swallowed air and accumulating intestinal secretions
(Compare to absent / reduced in paralytic ileus)
Bowel orgs cross the compromised bowel wall into peritoneal space
Tests
ABG (acidosis)
LFT (hypoalbuminaemia)
Complications
Infection
Gangerene of the bowel
Colicky pain
Constipation
U+E (Hypokalaemia)
Gastrograffin enema
Small bowel follow
through
AXR / CT
Perforation
Management
Analgesia: IV morphine 5 - 10 mg or diamorphine 2.5 - 5 mg
IV fluids: Normal saline until electrolyte balance known – 1L stat + 1 L 2˚
Nasogastric tube for decompression
Urinary catheter to measure output
Assess for laparotomy
Ruptured viscus
A patient with perforated viscus looks unwell. S/he will frequently have
generalised peritonitis
"board-like rigidity" on palpation of the abdomen.
Management: FAAANUX
Free air under the diaphragm
Fluids: stat 1˚, 2˚, 4˚
Causes include:
Analgesia
Ulcer
Antibiotics: Cef + Met
Neoplasm
Amylase levels
Bowel obstruction
NG tube + aspiration
Bowel Ischaemia
Urinary catheter
Trauma
X-ray showing diaphragm
The most common organs to perforate are the
Appendix,
Stomach,
Duodenum
Colon
Investigations include
Serum amylase (Rise of ~200 U in perforation, may indicate pancreatitis)
Erect and lateral decubitus CXR
Pregnancy test
The organ that is responsible may be indicated by the original site of the pain and the age of the
patient. The management for all is similar, with resuscitation followed by laparotomy.
3.11
Right Iliac Fossa pain
Any female of reproductive age is pregnant until proven otherwise!
General surgical
Appendicitis
Meckels diverticulum
Perforated caecal
carcinoma
Investigations:
(for diagnosis)
Gynaecologic
ECTOPIC pregnancy
Salpingitis
Ovarian cyst torsion
Management:
Non-surgical
Gastroenteritis
Urinary tract infection
UC / Crohns
Renal colic
Differential WCC
-HGG pregnancy test
Ultrasound scan if req.
Laparoscopy
(transvaginal / ado / pelvic)
Surgery – see box below for options in ectopic pregnancy
Questions:
Any possibility of pregnancy
Last menstrual period
Sexually active / contraception
Shoulder-tip pain / PV bleed
Previous appendicectomy
SOCRATES – especially note:
Movement of pain from central abdo
Anorexia
Nausea
O/E remember:
PREGNANCY TEST
Temperature (>37.3)
Rebound tenderness / tender to percussion
Screening for appendicitis
Ectopic pregnancy
The accurate diagnosis of acute appendicitis can be
extremely challenging - together with the large incidence,
this has prompted many suggestions of tools to improve
diagnostic accuracy. Simple scoring systems are very
attractive, as they require very little in resources.
While the usefulness of scoring systems as sole
identifiers of acute appendicitis has been called into doubt,
it seems reasonable that they can act as a useful aid to
clinical acumen, especially in less experienced clinicians at
the start of their surgical careers. One especially useful
factor is it reminds clinicians of the ‘watchful waiting’
option. Regular re-evaluation is acknowledged as being
useful in doubtful cases.
Any pregnancy that implants outside the uterine cavity.
The Alvarado system (MANTRELS)
Migrating pain
Anorexia
Nausea
Tender RLQ on examination
Rebound / tender to percussion
Elevated temperature (> 37.3)
Leukocytosis
Shift to left (neutrophils >75%)
<5: surgery not recommended
5-6: watchful waiting recommended
>6: Surgery recommended
Score
1
1
1
2
1
1
2
1
Alvarado A. A practical score for the early diagnosis of
acute appendicitis, Ann Emerg Med 1986; 15: 557-564
Benjamin IS, Patel AG. Managing acute appendicitis, Br
Med J 2002; 325: 505-506
Common sites include:
Fallopian tubes (accounts for 95%): Fimbrial, ampullary (most
common), isthmic and corneal.
Ovary
Cervix
Broad ligament
Abdomen
Risk factors include:
Factors making implantation more likely to occur in the wrong place:
Intr-uterine coil device
In-vitro fertilisation
Factors which damage the fallopian tubes and ciliary lining
Tubal surgery (sterilization, previous ectopic)
Previous pelvic surgery/peritonitis (adhesions)
Pelvic inflammatory disease
Endometriosis
Management
Medical:
IM methotrexate + follow-up HCG test
Surgical:
Complete or partial salpingectomy
Salpingotomy/salipingostomy (remove the
ectopic, but leave the tube and let it heal)
Psychological support must be made available
4.1
Fractured Hip (Fractured neck of femur)
Classically, this is a fracture of old age, affecting women in their eighth or ninth decade of life.
Usually the bone has been weakened by underlying disease - most commonly, osteoporosis but
also osteomalacia, diabetes, alcoholism and other conditions associated with osteopenia.
There is usually a history of trauma but in severely weakened bone, direct injury may be trivial or
absent. There is a debate as to whether "patients fall because they fracture or fracture because
they fall".
Rarely, fractures of the femoral neck are seen in children.
Generally the fracture is displaced and unstable. If some of the fragments have been impacted
then the patient may be able to walk with some pain and discomfort.
Causes
Femoral neck fractures most commonly follow a fall or blow on the greater trochanter which
may be quite trivial. In severely osteopenic bone, the femoral neck may fracture on
weightbearing, for example, on rising from a chair. Rarely, a femoral neck fracture follows severe
traumatic injury in a child.
Rotation
Posterior dislocation
Yes
Int
Add
Yes
Anterior dislocation
Neck of femur fracture
No
Yes
Ext
Ext
Abd
Abd
Yes
Yes
Intertrochanteric fracture
Yes
Ext +
Abd
Yes
Subtrochanteric fracture
Yes
Ext
Abd
Yes
Investigations
Flexion
Short
Adduction/
adduction
Differentials and clinical features
X-ray Pelvis
X-ray femoral shaft + knee
Common in drivers /
passengers of head-on
collision
Rare
May be able to stand
Blood supply poor
Mal / non-union common
Avascular necrosis risk
Cannot stand
Cannot raise leg
Blood supply good
Good union
Rare avascular necrosis
Swollen thigh
Intensely painful
CT if doubtful
Scintigram
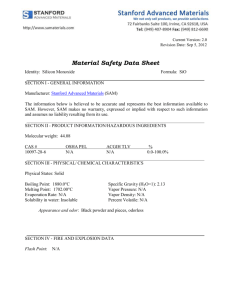
Anatomy
Ligamentum teres: a branch of the obturator
artery (absent in 20% of the population) – this
artery is insufficient to supply the head of the
femur in adults.
Retinacular arteries:
Nutrient artery: This is a branch of profunda
femoris and supplies the shaft of the bone.
Extra
Capsular
In the subcapital fracture the main arterial
supply is lost to the head – this is likely to
result in avascular necrosis of the head.
Management may be via replacement of the
head (hemiarthroplasty).
{
In the intratrochanteric (pertrochanteric)
fracture the main arterial supply to the head
is intact.
Management may be via internal fixation e.g.
with a dynamic hip screw.
Fracture Management
Any fracture is, almost by definition a trauma and there are certain protocols to follow:
Airway
Breathing
Circulation
When these are done the limb itself can be assessed
Blood supply is the most important factor to confirm
Neural function should be next
If the fracture is open then the following need to be considered
Surgical wound debridement (reduces infection risk)
Antibiotic cover (usually augmentin)
Tetanus booster ± tetanus immunoglobulin
There are three principles to fracture management (The 3 R’s)
Reduction: Via traction
Retention (or fixation) – this is the most effective pain relief in fracture.
Rehabilitation (intended to preserve function of joints above and below)
Fracture
Non-operative management
Mnemonic: COT
Cast / backslab
(backslab – plaster of paris or
fibreglass – former is more
moldable while latter is lighter)
Orthotics
(e.g. callipers, knee brace, collar
& cuff, sling, corset)
Traction
(Skin – if <24 hours and little wt;
Skeletal otherwise)
Operative management
Internal Fixation
Nail (through shaft of long bone)
Interlocking nail (a nail fixed by
screws to limit movement)
Screw (brings bone pieces into
tight opposition)
Plate (resists forces of rotation –
often used with screw)
Pin – e.g. K-wire (small bones,
little weight bearing)
External Fixation
A quick procedure performed in
damage control orthopaedics for
polytrauma. SE include poor
cosmesis and infection risk.
Can also be used when increasing
bone length and correcting
deformity
Fine wire frames
Half pins
4.2
Other important fractures
Fracture
Monteggia
Description
Fracture of ulna shaft with
dislocation of proximal
radioulnar joint
Galeazzi
Fracture of radial shaft with
dislocation of distal radioulnar
joint
Picture
Mnemonic: UP My Really Disgusting Gut
Ulna fracture + Prox radioulnar joint dislocation = Monteggia fracture dislocation
Radial fracture + Distal radioulnar joint dislocation = Galleazzi fracture dislocation
Colles’
Transverse fracture of radius
within 2.5 cm of wrist with
dorsal displacement of the
distal fragment
‘Dinner fork’ deformity
Smith’s
Transverse fracture of radius
just above wrist with Anterior
displacement of the distal
fragment
Scaphoid
75% of all carpal fractures
Tenderness in snuffbox
Pos prox avascular necrosis
Request scaphoid x-ray
Nerve damage most commonly associated with fractures
Nerve
Axillary
Mechanism
Badly adjusted crutch in axilla.
Shoulder dislocation.
Fractured surgical neck of
humerus.
Radial (in axilla)
Badly adjusted crutch in axilla.
Falling asleep with arm over
back of chair.
Fracture or dislocation of
proximal humerus.
Fractured shaft of humerus or
involved in the callus during
repair.
Radial (in spiral
groove)
Median (at
elbow)
Supracondylar fracture
Ulnar
Medial condyle fractures
Froment’s sign
Sciatic
Badly placed IM injections.
Penetrating wounds
Fractures of pelvis
Dislocation of hip.
Common
peroneal
Fracture of neck of fibula (e.g.
car bumper)
Pressure from casts or splints.
Rarely injured – deep and
protected under soleus.
Tibial
Obturator
Rare – anterior hip disloc. fetal
head during birth.
Motor
Impairment of abduction of
arm (now done just by
supraspinatus).
Muscle wasting and loss of
shoulder contour.
Unable to extend elbow joint,
wrist joint and fingers.
Wristdrop – disabling as it
prevents a tight grip with the
hand concerned.
If beyond branch to triceps
and anconeus: Unable to
extend wrist joint and fingers.
Wristdrop.
Pronators and long flexors of
forearm (except FCU and
medial FDP). Forearm is kept
supine and wrist flexion is
weak and accompanied by
adduction. No flexion at IP
joints of index and middle
fingers.
Paralysis and wasting of
thenar eminence.
FCU and medial half of FDP
are paralysed. Flexion of wrist
joint results in abduction.
Unable to adduct and abduct
fingers.
Small muscles of hand except
LOAF will be paralysed –
unable to adduct thumb.
Claw’ deformity ‘
Footdrop due to paralysis of
all lower leg muscles.
Hamstrings paralysed but
weak flexion of knee possible
by sartorius and gracilis.
Footdrop due to paralysis of
muscles in anterior and lateral
compartments of leg.
Dorsiflexion and eversion of
foot from paralysis of
muscles in back of leg and
sole of foot
All adductor muscles except
one head add mag.
Sensory
‘Regimental patch’
Lateral dorsal surface of hand
and up to DIP on latera 3½
digits (dorsal)
Dorsal aspect lateral 3½ digits
and lateral half of palmar
aspect
medial 1½ fingers.
All in below knee except as
supplied by femoral nerve.
All in below knee except as
supplied by femoral nerve.
Sole of foot – trophic ulcers
usually develop.
Minimal on medial side of
thigh.
Diseases that may contribute to fractures
Osteoporosis
Definition
Low bone mass and
enhanced fragility.
Mineralisation occurs
as normal
Risk factors
Female, increasing age,
Caucasian or Asian
race,
early menopause, small
frame, lack of
exercise, smoking,
excess alcohol,
low calcium intake.
Fracture is only cause
of symptoms.
Vertebral crush
fractures may lead to
pain, increasing
kyphosis, height loss
and protuberant abdo.
Clinical features
Investigations
Notes
Colle’s fracture and
fractured head of
femur more common
Radiographs for
fractures
DXA scan for bon
density
Prevention vis: diet,
exercise, smoking
cessation, and fall
reduction
Paget’s disease
A focal disorder of bone
remodeling –
excessive absorption
followed by
compensatory
abnormal new bone
formation
Genetic (gene on 18q)
Osteogenesis
Imperfecta
Defects in type I
collagen resulting in
fragile and brittle bones
Genetic – defects in
one of the Type I
collagen genes
Mostly asymptomatic.
Fragile and brittle bones
Pathological fractures
Nerve compression: CN
II, V, VII and VIII
(deafness)
Bone pain (esp spine /
pelvis)
Joint pain
Type I:
Mild bone deformities
blue sclera
Defective dentine
Early-onset deafness
Hypermobility of joints
Heart valve disorder
Alkaline phosphatase
with normal calcium
and phosph.
More severe forms may
present with multiple
fractures and gross
deformities
4.6
Bone or Joint infection
Osteomyelitis – bone infection
Direct inoculation (via trauma)
Foot puncture wounds (pseudomonas)
Haematogenous from systemic illness
Septicaemia via IV cannula (Staph aureus)
Sickle cell disease (Salmonella)
Immunodeficiency
Mainly seen in children: presentation differs
with age
Neonatal presentation
The infant may show deceptively little
constitutional derangement.
The baby fails to thrive, is drowsy but
irritable.
Risks for neonatal osteomyelitis include: a
difficult birth and in utero instrumentation
such as cordocentesis
Pain is localised to a metaphysis or joint.
There may be more than one site of
osteomyelitis.
Adult presentation
The commonest site of infection is in the
thoracolumbar spine.
Local tenderness is not impressive. There
may be mild fever and backache.
Child presentation
pain
malaise
fever
septicaemia, if the presentation is late
There may be a recent history of localised
sepsis, for example a boil.
The child will refuse to use a limb: touching
or moving the adjacent joint is impossible
local redness, warmth and oedema
Investigations:
Blood culture
Does not show on X-ray until
MRI
about day 10
FNA of pus
Management:
Debridement dead bone
Questions:
Fever
Malaise
Local pain esp backache in adults
Bone biopsy + culture
Radioisotope bone scan
Antibiotics
O/E remember:
Tenderness
Sinus if chronic
Signs of complicating septic arthritis
Septic arthritis
This is an orthopaedic emergency – if suspected, IMMEDIATE referral to orthopaedics is
indicated.
The effects of septic arthritis on the joints
Acute synovitis with purulent joint effusion
Articular cartilage is attacked
Articular cartilage is destroyed
Healing leads to bony ankylosis and joint destruction
Clinical features differ with the age of the patient
Newborn infants
Children
Acute pain in a single
Irritability
large joint (usually the hip)
Refusal to feed
Reluctance to move the
Possible pyrexia
Adults
Acute pain – usually of a
superficial joint e.g knee,
wrist, ankle)
Examination
Look for sites of entry –
umbilical cord / inflamed IV
access site.
Tachycardia
Carefully palpate and
move joints looking for:
- Warmth
- Tenderness
- Resistance to movement
Investigations:
X-ray often normal
Management:
limb (pseudoparesis).
Swinging pyrexia
Examination:
Look carefully for site of
infection – e.g. septic toe,
boil, ear discharge
Overlying skin is red
? Superficial joint swelling
Tachycardia
Ultrasound of joint
WCC (infection)
Uric acid level (?gout)
Immediate joint aspiration
Surgical drainage
Analgesia
Pseudoparesis
Ask about gonnococcal
infection or IDU
Examination
Warmth
Marked tenderness
Pseudoparesis
Joint aspiration – send
fluid for WCC count and
Gram Stain
Antibiotics
Splinting
Indications for surgery include
For the very young
Where the hip is involved
Where aspirated pus is very thick
If repeated closed aspiration produces no improvement within 48 hours
The surgical treatment is drainage and washout (normal saline) under anaesthetic. A catheter is
left in place and the wound closed with suction irrigation continuing for 2-3 days.
Questions:
Fever
Malaise
Local pain esp backache in adults
O/E remember:
Redness around joint (crystal or septic)
Signs of complicating osteomyelitis
including a sinus
Decreased range of movement
4.7
Burns requiring hospital admission
Investigations:
Management:
Arterial blood gas and
COHgb
Group and save / XM
? Definitive airway
100% Oxygen
Fluid – amount via
Packland formula
Questions:
Nature of burn – in detail.
U+E (fluid status)
FBC: haemolytic anaemia
LFT
Analgesia - morphine
Fluid chart ± catherisation
Tetanus prohylaxis
X-ray for other injuries
O/E remember:
Assess airway – signs of future airway
compromise needing ET tube include
Facial / upper torso burns
- Blackened sputum
- Dry, red or blistered oropharynx
- Assess extent and depth of burns
Extent using the ‘rule of nines’ and the fact
that the patients palm+fingers = 1%
Depth as per chart below
The Packland formula can be used to work out how much fluid to give:
Fluid loss in burns may be huge but usually occur 6-8 hours post injury. If the burn covers <15%
TBSA then oral fluids are likely to be sufficient. Otherwise IV isotonic fluids such as Ringers
Solutions should be used.
Fluid (ml) = patients wt (Kg) x TBSA affected x 4
Half is given in the first 8 hours. The other half is given over the next 16 hours.
This must be in the first 8 hours after the burn occurred – if itr takes 2 hours post burn time to get
the fluid started then it must be given in 8-2 = 6 hours. This fluid requirement is only to cover burn
losses – the patients normal fluid requirements must be added on top of this!
In the US the depth of a burn is measured in ‘degrees’ (°) e.g first degree to fourth degree. In the
UK a rather simpler system is used:
Superficial burns (erythema)
Partial thickness
Total thickness
DEPTH
Erythema
Partial
thickness
Full thickness
PAIN
+
SENSATION
+
BLISTERS
No
FEEL
Normal
CAPILLARY
+
COLOUR
Pink
+++
+
Yes
Moist
+
Mottled
-
-
No
Dry & Leathery
-
White/Charred
Partial thickness burns have the capacity to heal rapidly because of the presence of viable dermal
components. Re-epithelialization occurs from both the base and the edge of the burn-wound and
healing should be complete within 21 days. Full thickness burns only heal from the edge and
therefore healing is slow in anything but the smallest burns. Delayed healing results in a poor
quality contracted scar which, in the hand, inevitably compromises function.
It is recognised that exposure to flames or electrical current almost always results in a full
thickness burn whereas a scald with water usually produces a partial thickness burn. However, if
the scalding fluid is fat, the burn is almost certainly full-thickness.
Psychological sequelae and treatment after the emergency treatment phase
The acute phase of recovery focuses on restorative care, but patients continue to undergo painful treatments. As patients
become more alert during this phase, they face these procedures with less sedation. Also, patients are more aware of the
physical and psychological impact of their injuries.
Depression and anxiety—Symptoms of depression and anxiety are common and start to appear in the acute phase of
recovery. Acute stress disorder (occurs in the first month) and post-traumatic stress disorder (occurs after one month) are
more common after burns than other forms of injury. Patients with these disorders typically have larger burns and more
severe pain and express more guilt about the precipitating event. The severity of depression is correlated with a patient's
level of resting pain and level of social support.
Sleep disturbance—Central to both anxiety and depression is sleep disturbance. The hospital environment can be loud,
and patients are awakened periodically during the night for analgesia or for checking vital signs. Patients' mood, agitation,
and nightmares can all affect sleep.
Premorbid psychopathology—Compared with the general population, burn patients have a high rate of premorbid
psychopathology. Patients with pre-existing psychopathology typically cope with hospitalisation through previously
established dysfunctional and disruptive strategies. The most common premorbid psychiatric diagnoses are depression,
personality disorders, and substance misuse. Prior psychopathology can have an adverse impact on outcomes, including
longer hospitalisations and the development of more serious psychopathologies after injury.
Grief—Patients may now begin the grieving process as they become more aware of the impact of the burn injuries on their
lives. Family members, friends, or pets may have died in the incident, and patients may have lost their homes or personal
property. In addition to these external losses, patients may also grieve for their former life (such as job, mobility, physical
ability, appearance). Mental health professionals and other staff should help patients to grieve in their own way and at their
own pace.
Treatment
Brief psychological counseling can help both depression and anxiety, but drugs may also be necessary. When offering
counseling, it is often helpful to provide reassurance that symptoms often diminish on their own, particularly if the patient
has no premorbid history of depression or anxiety.
Drugs and relaxation techniques may also be necessary to help patients sleep. Informing patients that nightmares are
common and typically subside in about a month can help allay concerns. Occasionally patients will benefit from being able
to talk through the events of the incident repeatedly, allowing them to confront rather than avoid reminders of the trauma.
Staff often make the mistake of trying to treat premorbid psychopathology during patients' hospitalisation. Referrals to
community treatment programmes should be made once patients are ready for discharge.
The long term (Rehab) stage of recovery typically begins after discharge from hospital, when patients begin to reintegrate
into society. For patients with severe burns, this stage may involve continued outpatient physical rehabilitation, possibly
with continuation of procedures such as dressing changes and surgery. This is a period when patients slowly regain a
sense of competence while simultaneously adjusting to the practical limitations of their injury. The first year after
hospitalisation is a psychologically unique period of high distress.
Physical problems—Patients face a variety of daily hassles during this phase, such as compensating for an inability to use
hands, limited endurance, and severe itching. Severe burn injuries that result in amputations, neuropathies, heterotopic
ossification, and scarring can have an emotional and physical effect on patients.
Psychosocial problems—In addition to the high demands of rehabilitation, patients must deal with social stressors
including family strains, return to work, sexual dysfunction, change in body image, and disruption in daily life. Many people
continue to have vivid memories of the incident, causing distress. Patients may also develop symptoms of depression.
There is evidence that adjustment to burn injuries improves over time independent of the injury size. Social support is an
important buffer against the development of psychological difficulty.
Treatment
It can be helpful to make follow up telephone calls to patients after discharge or to continue to see patients in an outpatient
clinic to screen for symptoms of distress and to provide psychotherapy.
Adjustment difficulties that persist more than a year after discharge usually involve perceptions of a diminished quality of
life and lowered self esteem. Some studies suggest that burn disfigurement in general leads to decreased self esteem in
women and social withdrawal in men. "Changing Faces" is a successful programme for enhancing self esteem. This
includes a hospital based programme for image enhancement and social skills plus a series of publications for patients
dealing with aspects of facial disfigurement.
Many patients face a lengthy period of outpatient recovery before being able to return to work. Some patients go through
vocational challenges. In a recent study of patients hospitalised for burn injury 66% returned to work within six months of
their injury, and 81% had returned by one year. As expected, patients who sustained larger burns took longer to return to
work. About half of the patients required some change in job status.
Ancillary resources such as support groups and peer counselling by burn survivors can also be important services to burn
survivors. Major burn centres ideally have a network of burn survivors who are willing to talk with patients in the hospital.
BMJ 2004;329:391-393
4.9
Acute monoarthritis
Acute monoarthritis is septic until proven otherwise
Common
Septic (staph aureus or
gonococcus usually)
Gout / pseudogout
Trauma
Ligament / meniscal
trauma
Investigations:
X-ray often normal in septic
arthritis
Management:
Less Common
Painful exacerbation of
existing arthritis
Acute haemarthrosis
Osteonecrosis
Ruptured popliteal cyst
DVT
Ultrasound of joint
WCC (infection)
Uric acid level (?gout)
Joint aspiration (above)
Immediate joint aspiration
Surgical drainage
Analgesia
Joint aspirate tests
WCC (<1 x 109 = non
inflam, >100 = septic)
Gram stain + culture
Crystals
X-ray
Blood / urine culture
Swabs for gonnorhoea
Synovial biopsy
Antibiotics
Splinting
Questions:
O/E remember:
Fever / Malaise
Redness around joint (crystal or septic)
Local pain esp backache in adults
Decreased range of movement
History of prior similar events – suggests
Tophi – ears, elbows, fingers, toeas and
crystal arthropathy
joint in question
immunocompromised patients (such as
those taking immunosuppressants / HIV)*
rheumatoid arthritis*
diabetes mellitus*
intravenous drug users*
prosthetic joints*
Anticoagulants (acute haemarthrosis)
Risk factors for gonnorhoea
*Less likelihood of a strong inflammatory response – be doubly aware of septic arthritis even if
little inflammation
Septic arthritis
This is an orthopaedic emergency – if suspected, IMMEDIATE referral to orthopaedics is
indicated.
The effects of septic arthritis on the joints
Acute synovitis with purulent joint effusion
Articular cartilage is attacked
Articular cartilage is destroyed
Healing leads to bony ankylosis and joint destruction
Clinical features differ with the age of the patient
Newborn infants
Children
Acute pain in a single
Irritability
large joint (usually the hip)
Refusal to feed
Reluctance to move the
Possible pyrexia
limb (pseudoparesis).
Examination
Swinging pyrexia
Look for sites of entry –
umbilical cord / inflamed IV Examination:
access site.
Look carefully for site of
infection – e.g. septic toe,
Tachycardia
boil, ear discharge
Carefully palpate and
Overlying skin is red
move joints looking for:
- Warmth
? Superficial joint swelling
- Tenderness
Tachycardia
- Resistance to movement
Investigations:
Ultrasound of joint
X-ray often normal
WCC (infection)
Uric acid level (?gout)
Management:
Immediate joint aspiration
Surgical drainage
Analgesia
Adults
Acute pain – usually of a
superficial joint e.g knee,
wrist, ankle)
Pseudoparesis
Ask about gonnococcal
infection or IDU
Examination
Warmth
Marked tenderness
Pseudoparesis
Joint aspiration – send
fluid for WCC count and
Gram Stain
Antibiotics
Splinting
Indications for surgery include
For the very young
Where the hip is involved
Where aspirated pus is very thick
If repeated closed aspiration produces no improvement within 48 hours
The surgical treatment is drainage and washout (normal saline) under anaesthetic. A catheter is
left in place and the wound closed with suction irrigation continuing for 2-3 days.
Questions:
Fever
Malaise
Local pain esp backache in adults
O/E remember:
Signs of complicating osteomyelitis
including a sinus
Decreased range of movement
4.10
Low Back pain
Common
Muscle strain / sprain
Disk degeneration*
Disc prolapse*
Less Common
Spinal stenosis
Spondylolisthesis
Ankylosing spondylitis
Osteoarthritis
Polymaylgia rheumatica
Osteomyelitis
TB spine
Tumour
Radiating from Abdomen
Radiates through to the back
AAA
Aortic dissection
Pancreatitis
Duodenal ulcer
Radiates round to the back
Cholecystitis
Biliary / Renal colic
The options can be narrowed down by a few simple questions:
Transient following
Sudden, acute pain with
Intermittent after exertion
muscular activity
sciatica
<20 years
Muscle strain / sprain
Disk degeneration*
Osteomyelitis
Osteoarthritis
Spondylolisthesis
Ankylosing spondylitis
20-40 years
Chronic osteomyelitis
Disc prolapse*
TB spine
Elderly
Compression fractures
Severe, constant and
With pseudoclaudication
Radiating from Abdomen
localized to a particular site
Radiates through to the back
Spinal stenosis
Compression fracture
AAA
Paget’s disease
Aortic dissection
Primary / secondary
tumour
Pancreatitis
Osteomyelitis
Duodenal ulcer
Radiates round to the back
Cholecystitis
Biliary / Renal colic
Investigations:
X-ray (lumbar spine /
Facet joint injection of
abdomen)
local anaesthetic (nerve rt)
CT / MRI spine
Amylase
Electromyography
CT/MRI abdomen
Management:
Activity as appropriate
Chemonucleolysis**
Analgesia
Laminectomy / discectomy
Antibiotics as appropriate
spinal fusion
Facet joint inject. (steroid)
*Most commonly L4/5 or L5/S1 **intradisc injection of chymopapain to pain / inflammation
Questions:
Following muscular activity
Sciatica
Pseudoclaudication
Is there associated abdo pain (may be pain
from abdo radiating to back)
Worsened by coughing / straining (disc)
Urinary retention (cauda equina)
Red flags
backache in young (<20 years) or older
patient (> 55 years)
may be history of trauma
backache not mechanical (i.e. not related
to movement)
thoracic pain is more sinister than lumbar
pain
Disk degeneration
Disc prolapse
Spondylolisthesis
Spinal stenosis
O/E remember:
Numbness in affected dermatome (nerve
root compression/
Weakness/ depressed reflexes in muscles
supplied by that root.
Ankle reflex
Knee on affected side may be held in
flexion to reduce sciatic nerve tension
Sensory loss over sacrum ± anal wink
unwell e.g. weight loss, night sweats
widespread neurological signs (not limited
to one nerve root)
progressive neurological deficits
structural deformity associated with
backache
constant and/or progressive pain
severe nocturnal pain
Common, natural part of senescence
Usually fit person aged 25-45
Starts with lifting or stooping – severe pain and unable to
straighten parasthesia / numbness leg / foot
Relapsing and remitting
Worsened by coughing / straining
No pain in children
Pain starts in adolescence or adulthood.
Part of the spine ‘slips’ forward, having lost (or never had)
the anatomical protections against this occurring. Fracture,
degenerative change and congenital malformation are
causes. Usually occurs at L4/5 or L5/S1
Typically male, typically >50
Narrowing of the spinal canal (bilateral symptoms) or the
intervertebral foramina via e.g. disc protrusion, OA, Paget’s,
spondylolisthesis.
Signs and symptoms of lumbar stenosis include
neurogenic claudication (pain in the legs with walking, which
is relieved by bending and sitting), leg weakness, leg
numbness, and loss of deep tendon reflexes.
4.11
knee
Chronic painful hip or
Spinal Stenosis
Common
Osteoarthritis
Investigations:
Management:
*Most commonly L4/5 or L5/S1
Questions:
Seropositive differentials
Rheumatoid arthritis
X-ray
O/E remember:
Seronegative differentials
Secondary OA
Psoriatic arthritis
Reiters syndrome
Rheumatoid factor
Worsened by coughing / straining (disc)
Urinary retention (cauda equina)
5.1
Numbness in affected dermatome (nerve
root compression/
Weakness/ depressed reflexes in muscles
supplied by that root.
Knee on affected side may be held in
flexion to reduce sciatic nerve tension
Sensory loss over sacrum ± anal wink
Pre-operative assessment and post-operative management of a patient
undergoing a major surgical procedure with significant underlying disease.
A patient’s risk from anaesthesia is ranked by the American Society of Anaesthiologists system
ASA Grade
Definition
Mortality (%)
I
Normal healthy individual
0.05
II
Mild systemic disease that does not limit activity
0.4
III
Severe systemic disease that limits activity but is
not incapacitating
4.5
IV
Incapacitating systemic disease which is constantly
25
life-threatening
V
Moribund, not expected to survive 24 hours with
or without surgery
50
Some examples of this are:
ASA Grade 2
ASA Grade 3
Angina
Occasional use of GTN.
Regular use of GTN or unstable angina
Hypertension
Well controlled on single agent
Poorly controlled. Multiple drugs
Diabetes
Well controlled. No
complications
Poorly controlled or complications
COPD
Cough or wheeze. Well
controlled
Breathless on minimal exertion
Asthma
Well controlled with inhalers
Poorly controlled. Limiting lifestyle
Preoperative preparation:
The idea here is to improve the patient’s condition as much as possible prior to surgery and to
minimize the risks of surgery itself.
Inpatients and day-cases:
Encourage smoking cessation for as long as possible pre-op. 8 weeks improves the airways, 2
weeks reduces airway irritability, and 24 hours decreases carboxyhaemoglobin levels.
Find the day of last menstrual period.
Ensure appropriate fasting has been observed.
All inpatient cases:
Clexane should be started 20 mg (40 mg in orthopaedic procedures) but see below.
Clexane should be ceased 12hr before (20 mg) dose or 24hrs before (40 mg)
TED stocking should be prescribed
As appropriate (check with seniors):
Current anticoagulant drugs should be stopped (Warfarin should be stopped 3 days prior)
Transfusions to raise Hb
Legal issues
It is not the house officers job to gain consent but it is worthwhile checking that all is in order here
– draw to your seniors attention any problems
Ensure DNR issues are discussed with the patient and relatives as appropriate AND
RECORDED. The anaesthetist should be made aware of DNR decisions.
Fluid Management
Fluid distribution throughout the body:
The 2/3rds rule: approximately 2/3rds of the body is water and 2/3rds of this is intracellular.
Total: 45 L
Intracellular: 30 L
Extra cellular: 15 L
Extravascular: 12 L
Intravascular: 3 L
The 1,2,3,4,5 rule: extra vascular = 12, intravascular = 3, total = 45 L (for 70 Kg man).
The aim of giving fluids is to replace what is used for basic requirements (passed out in urine,
faeces, breath and perspiration) and also any deficit. Deficit may be caused by:
Past dehydration e.g. not drinking (i.e. NBM before surgery…)
Vomiting
Diarrhoea
Bleeding
Basic requirements are:
Water: 30-40 ml / Kg / day (2-3 L for a 70 kg person)
Na+: 1-2 mg / Kg / day (70-140 mg for a 70 kg person)
K+: 1 mg / Kg / day (70 mg for a 70 kg person)
Glucose: 100 g to allow protein sparing.
In a 70 Kg person this is approximately 2800 ml water, 140 mg Na+ and 70 mg K+. This is the
minimum that must be given. Any deficit should ideally be made up within one day but in patients
with heart problems this may be stretched over two days.
A fluid balance chart should be used to account for fluid intake and loss – remember to allow for
insensible losses (at least 700 ml) and oral intake.
Fluid
Crystalloids
0.45% saline
0.9% saline
Dextrose saline
5% dextrose
10% dextrose
Hartmanns / Ringers
Na+
79
154
30
130
Fluid Choices
K+
Ca+
(mmol / L)
- / 20 / 40
- / 20 / 40
- / 20 / 40
4
30
Cl-
Lactate
Dex (g / L)
79
154
30
109
28
40
50
100
-
Note that most of these do not contain K+ - this must be added. 0.45, 0.9% and dextrose saline
are available with either 20 mg or 40 mg added per litre.
It is easy to give too much Na+ - this is not a problem normally as it will be excreted in patients
with normal renal function. It should be avoided where this is not the case.
Losses to diarrhea / vomiting should be replaced with 0.9% saline or Hartmanns solution.
Prescribing IV fluids
Ensure adequate access – a ‘green’ Venflon is the smallest that blood may be given through. A
local anaesthetic may make it easier to put in a large (e.g. 14 gauge) cannula.
Do not write up fluids for more than 24 hours – conditions change rapidly.
Writing up less than 3 litres will dehydrate most patients.
If fluid needs are urgent then start with a fast or ‘stat’ dose and decrease the rate through the day.
The fastest rate at which fluids may be given is dependent upon the gauge of cannula used – the
widest (‘white’ Venflon) allows 1L to be given over about 20 mins ‘stat’.
Rates are written up using the ° symbol. e.g. 8° means ‘over 8 hours’.
Fluids are drugs – be careful what you prescribe!
Replacing blood loss
Colloids can be used if Hb levels are normal or if blood products are unavailable. examples are
gelofusin or albumin.
Emergency ‘O neg’ blood can be used if bleeding is extreme.
Cross matched blood is better than ‘O neg’ but takes about 45 mins to source.
If large volumes are given, clotting factors will become depleted – think about giving clotting
factors and FFP.
Correcting Electrolyte imbalance
Hypokalaemia (<3.5): causes include diarrhoea, vomiting, inadequate replacement, alkalosis,
diuretic therapy, bicarbonate, salbutamol, glucose-insulin, hyperventilation.
Give additional K+
Hyperkalaemia (>5): causes include renal failure, acidosis, K+ sparing diuretics
Dextrose 50 ml, 50% Stat
Insulin 10-20 units, Stat
Salbutamol nebs
10 ml calcium gluconate slowly IV (to protect heart)
Correct acidosis (see below)
Hyponataemia (<135): May be due to excess water (dilutional) or sodium rich losses.
For acute dilutional hyponatraemia: Water restriction – omit 5% dextrose or dextrose-saline
from the regimen
For acute salt-losing hyponatraemia: 0.9% saline + appropriate K+
Hypernatraemia (>145): Usually a sign of true dehydration
Give 5% dextrose or dextrose-saline.
Correcting acidosis: give X ml 8.4% sodium bicarbonate. X = base excess x Kg x 0.3
Post operative nausea and vomiting
These may be normal parts of post-op recovery for some patients irrespective of other
medications but opioids do tend to aggravate this problem.
Causes:
Anaesthetic drugs
Other Drugs
Undiagnosed illness: e.g. bowel obstruction
Dehydration / fasting
Inadequate analgesia
Lack of sleep
Anxiety
There are several phases to treating N&V – start at step one and move down if needed.
1
2
3
4
A.
B.
C.
D.
E.
F.
Review anaesthetic chart
Review medications
Oxygen
Adequate analgesia
Rest and sleep
Nil by mouth & nasogastric
tube
G. Fluids
H. Catheterisation
I. Treat infections
J. Consider ileus or other
complications
K. Cyclizine + wait 30 mins
L. If ineffective give
Ondansetron
M. Get senior help if no
improvement after 8 hours
N. Dexamethasone
O. Sedations
P. ITU
B: do not neglect to try drugs from several
classes instead of simply increasing dose.
B: Contact pain team for advice
D: Cut out unnecessary medications
D: Look for alternatives less likely to
induce nausea
E: Consider moving to a darker, quieter
part of the ward – especially if confused.
K: Cyclizine hydrochloride 50 mg i.m. This
is an antihistamine and an antimuscarinic
and inhibits vomiting at the vomiting centre
pathways and in the GI pathways. The few
side effects are mainly antimuscarinic (e.g.
dry mouth)
L: Ondansetron is a serotonin antagonist
and inhibits vomiting at the chemoreceptor
trigger zone, small bowel and vagus nerve.
They are effective but expensive and may
cause asymptomatic ECG changes.
N: Dexamethasone is a steroid and may
be given pre-op or as a last line rescue
treatment.
Post-operative confusion
A mnemonic to help remember the common causes of delirium is HIDEMAP. The likeliest
postoperative causes are listed in bold.
H
I
Hypoxia
Infection
Investigations
O2 SATS; Blood gas
FBC for WCC; ESR; Urine dipstick; cultures: urine as a
routine, sputum if available, blood if febrile or clearly ill for
no obvious reason
D
E
M
A
P
Drugs (incl. withdrawal)
Endocrine (e.g. diabetes)
Metabolic (e.g. Ca2+)
Alcohol
Psychosis
Drug screen
BM, serum glucose, TSH, T4
Serum calcium, U+E
LFT & Gamma GT
Mental state examination ± psychiatric referral
Pre-op continuation of antidepressants: A Canadian study found that continuing antidepressant
therapy pre-op decreased the chances of post-op confusion and had no adverse effects.
Akira Kudoh, MD*, Hiroshi Katagai, MD and Tomoko Takazawa, MD. Canadian Journal of Anesthesia 49:132-136 (2002)
Management of post-operative confusion consists of:
Reassurance may help to reduce fear – this in turn may reduce confusion as will having familiar
faces (relatives, known nursing staff) around. The ideal is a quiet side room with low lighting but
this is rarely achievable!
Do not forget to reassure the relatives – they may be upset by this change otherwise.
Ensure that the patient has their glasses / hearing aid! Being unable to perceive the environment
can increase or precipitate confusion.
Provision of a clock and calendar with the date marked may help orientation.
Doctors can help by introducing themselves whenever they meet the patient ‘Hi, do you
remember me, I’m Dr…’ and using a reassuring tone of voice.
If disturbance is extreme then consider sedation with Haloperidol or Chlorpromazine. These
doses need to be heavily modified in the elderly and it is suggested that Haloperidol 0.5 mg +
diazepam 0.5 mg or lorazepam 0.5 mg on its own.
Finding the source of the problem and remedying it (see investigations above).
Older patients (>70-80) are more susceptible to postoperative confusion – this may last many
days and may include symptoms of psychosis.
Post-operative respiratory failure
Causes of respiratory failure include
Type 1 resp failure
PaO2 <8 kPa; PaCO2
normal/
Pneumonia
Pulm oedema
PE
Asthma
Emphysema
Fibrosing alveolitis
Right left shunt
Cyanotic congenital heart
disease
Type 2 respiratory failure: PaO2 <8 kPa; PaCO2 >6 kPa
Pulmonary disease:
Asthma
COPD
Pneumonia
Pulm fibrosis
Obstructive sleep apnoea
Reduced Respir. drive
Sedative drugs
CNS tumour
Trauma
Neuromuscular:
Cervical cord lesion
Poliomyelitis
Gullaine Barré
Myasthenia gravis
Muscular dystrophies
Diaphragmatic paralysis
Thoracic wall disease
Flail chest
Kyphoscoliosis
As well as the clinical features of the underlying cause of the respiratory failure, the following are
signs and symptoms:
Hypoxia: PaO2 <8 kPa
If long standing:
Dyspnoea
Polycythaemia
Restlessness
Pulmonary
agitation
hypertension
confusion
Central cyanosis Cor pulmonale
Initial patient assessment:
Assess the patient's previous disability
Are there signs of deterioration?
Screening investigations:
Chest radiology
Blood gases
Peak expiratory flow rate
ECG
Full blood count
Biochemistry
Sputum and blood culture
Store a blood sample for serology
Hypercapnia: PaCO2 >6 kPa
Headache
Tremor / flap
Peripheral
Papilloedema
vasodilatation
Confusion
Tachycardia
Drowsiness
Bounding pulse
Coma
Background Box: Bounding pulse
With the patient reclining, the examiner raises
the patient's arm vertically upwards. The
examiner grasps the muscular part of the
patient's forearm. A waterhammer pulse is felt
as a tapping impulse which is transmitted
through the bulk of the muscles.
Give oxygen:
In cardiac or respiratory arrest, 100% O2 is required – use a rebreathing / anaesthetic mask.
In hypoxaemia with PaCO2 <5.3 kPa, 40-60% O2 is required – use a low flow mask
In hypoxaemia with PaCO2 >5.3 kPa, 24% O2 is required (initially) – use a high flow mask.
Adjust the oxygen supplied carefully upwards (e.g. to 28%) if repeat ABG shows little or no
increase in PaCO2
If ABG shows >1.5 kPa increase in PaCO2, consider a respiratory stimulant (e.g. doxapram
1.5 – 4 mg / min IV) or assisted ventilation (e.g. NIPPV – non-invasive positive pressure
ventilation).
Post-operative analgesia
Some important modalities of analgesia include
Reassurance – that the pain will go away and is not indicative of something ‘serious’.
Advice – telling the patient about pain and what analgesia is available both pre and post-op
will help to remove worries and this in itself decreases pain.
Sedatives e.g. diazepam
Non-opioids (level 1 of the WHO analgesic ladder)
An example is paracetamol 1g qds
A good non-opioid for moderate pain is acupan (nefopam hydrochloride).
NSAIDS are best used only where their anti-inflammatory role is required – use paracetamol
as an alternative.
Weak opioids (level 2 of the WHO analgesic ladder – given with or without adjuvants)
An example is cocodamol – 8mg codeine phosphate + 500 mg paracetamol x2 qds
Strong opioids (level 3 of the WHO analgesic ladder – given with or without adjuvants)
An example is diamorphine 2.5 –5 mg
Drug
Cautions
Contraindications
Side effects
Aspirin
Asthma
Age <16 (Reys syndr)
GI irritation
300-900 mg
Allergy
Breast feeding
bleeding time
every 4-6hrs
Hepatic impairment
Peptic ulceration
Bronchospasm
Max 4g / d
Renal impairment
Haemophilia
Interactions with warfarin
Paracetamol
Rare: Rashes, BP
Alcohol dependence
0.5 – 1g
Rare: blood disorders**
Hepatic impairment
None listed in BNF 50
every 4-6hrs
Severe hepatic damage in
Renal impairment
Max 4g / d
overdose
Acupan
Elderly
May colour urine pink
30-90 mg tds
Pregnant / breastfeeding
Convulsive disorders
Blurred vision
Max dose 270
Hepatic impairment
Not suitable for MI
Headache
mg /d
Renal impairment
Confusion / hallucination
Codeine
Nausea and vomiting
Hypotension
30-60 mg every
Constipation
Hypothyoidism
4 hrs
Drowsiness
Pregnant / breastfeeding
Acute respiratory depression
Max dose 240
Headache
Hepatic impairment
Acute alcoholism
mg / d
Facial flushing
Prostatic hypertrophy
Raised ICP / head injury
Hallucinations
Morphine*
Mood changes
10-15 mg every
Decrease dose in elderly
Decreased libido / impotency
2-4 hrs
* Dose listed is for postoperative pain. Dose may differ for other uses and for children. May be given PO, IM, IV, SC but
IM / SC is the usual for postoperative pain.
**thrombocytopaenia, neutropaenia, leucopaenia
Combination agents
Co-codamol 8/500
Co-codamol 15/500
Co-codamol 30/500
Co-dydramol 10/500
Co-dydramol 20/500
Co-dydramol 30/500
Content
Codeine phosphate 8 mg; Paracetamol 500 mg
Codeine phosphate 15 mg; Paracetamol 500 mg
Codeine phosphate 30 mg; Paracetamol 500 mg
Di-hydrocodeine tartrate 10 mg, Paracetamol 500 mg
Di-hydrocodeine tartrate 20 mg, Paracetamol 500 mg
Di-hydrocodeine tartrate 30 mg, Paracetamol 500 mg
Dose
T-TT t/qds
T-TT t/qds
T-TT t/qds
TT qds
TT qds
TT qds
IV Patient controlled analgesia:
It is important when starting IV PCA that an appropriate loading dose is given – if this does not
occur then PCA is unlikely to ever achieve adequate pain control and certainly will not do this for
some time.
Haematologic maligignancy
Child
ALL
Hodgkins lymphoma
Investigations:
Management:
Adult
ALL
AML
CML
CLL
Hodgekins lymphoma
Non-hodgekin’s lymphoma
Myelofibrosis
Myeloma
Full blood count
Blood film
Bone marrow aspiration
Elderly
CLL
Non-hodgkin’s
lymphoma
Myelofibrosis
Myeloma
Lymph node biopsy
CXR (mediastianal)
MRI chest / abdo / pelvis
Questions:
Constitutional upset: fatigue, tiredness
Bleeding
Infection
Bone pain
Gout
Hypercatabolic: wt loss, fever, night sweats
O/E remember:
Lymphadenopathy
Splenomegaly
Hepatomegaly
Gum hypertrophy
Testicular enlargement
Tumours of bone marrow (haematopoietic
stem cells)
Acute: symptoms for days-weeks
Acute lymphoblastic leukaemia
Acute myeloloid leukaemia
Chronic: often presents incidentally or with
months years of SOB, malaise, tiredness
Chronic lymphocytic leukaemia:
Chronic myeloid leukaemia:
Common features
Anaemia
Neutropenia infections
Thrombocytopenia bleeding
WCC is not always elevated
Infiltration of other tissues with leukaemic
cells
Increase in basal metabolic rate
excessive sweating and weight loss
Tumours of lymphoid tissues
Hodgkin’s lymphoma
Non-hodgkin’s lymphoma
Classic questions:
Philadelphia chromasome: 95% of patients with CML
have the Philadelphia Chromosome: this is a
translocations between the long arms of chroms 9 and
22 and is written as: t(9;22).
Reed-Sternberg cells: ‘giant transformed Blymphocytes containing 2 mirror image nuclei with
prominent owls eye nucleoli’ found in Hodgkin’s
lymphoma. See left.
Myelofibrosis
Myeloma
7.6 & 7.8
Breathlessness
Wheezy (ABCDEF)
Asthma
Adult onset-asthma
Bronchiectasis
COPD
Cardiac ‘asthma’ (rare)
Doomy: Large airway
obstruction e.g. bronchial
carcinoma
Oedema (pulmonary)
Foreign body: large airway
obstruction
Investigations:
Peak flow
Chest X-ray
Spirometry
Management:
Acute onset
Pulmonary
Acute severe asthma
Exacerbation COPD
Pneumonia
Pneumothorax
ARDS
Anaphylaxis
Cardiac
Left ventricular failure
Acute PE
Mitral stenosis
Other
Panic attack
Fever
Metabolic acidosis
Investigations:
Peak flow (if asthmatic)
Arterial blood gas
Chest X-ray
D-Dimers
Blood cultures
ECG
Spirometry
Questions:
Onset, progression
Exacerbating / relieving factors
Esp. is it relieved by rest
Sputum production
Exercise tolerance
Recent temperature
Heart disease
Intermittant claudication
Angina
FULL occupational history
Any pets / animals (inc pigeons etc)
Chronic on effort
Pulmonary
COPD
Bronchial cancer
Pleural effusion
Interstitial lung disease
Cardiac
Chronic heart failure
Angina equivalent
Chronic PE
Other
Physical deconditioning
Obesity
Anaemia
Investigations:
Full blood count (anaemia)
Chest X-ray
D-Dimers
Spirometry
Exercise tolerence test
O/E remember:
Pallor
Cyanosis (peripheral / central)
Wheeze?: polyphonic or monophonic
7.9
Acute pleuritic chest pain ± fever
With fever
Pneumonia
Tuberculosis
Bornholm disease
(Coxsackie B virus)
Sometimes with fever
Pulmonary infarction
Investigations
Chest X-ray
U+E (urea may be in
pneumonia)
D-dimers
Usually without fever
Fractured ribs
Muscle strains
Herpes zoster in early
stages
Pericarditis
Blood cultures ± acid fast
bacilli
Management:
Questions:
Dizziness / syncope
O/E remember:
BP
JVP
Signs of pericarditis
Pneumonia
Pulmonary Embolism
Symptoms
Onset
Dyspnoea
Cough
Heamoptysis
Pleuritic chest pain
Dizziness
Syncope
Gradual (over days)
Potentially present
Potentially present
Potentially present
Potentially present
Usually absent
Usually absent
Sudden
Potentially present
Usually absent
Potentially present
Potentially present
Potentially present
Potentially present
Signs
Fever
Confusion
Tachypnoea
Cyanosis
Tactile vocal fremitus
Percussion note
Bronchial breathing
Crackles
Whispering pectoriloquy
Pleural friction rub
Tachycardia
Hypotension
Raised JVP
Potentially present
Potentially present
Potentially present
Potentially present
Usually
Usually
Potentially present
Potentially present
Potentially present
Potentially present
Potentially present
Potentially present
Usually absent
Potentially present
Usually absent
Potentially present
Potentially present
(unreliable)
Stony dull
Potentially present
Usually absent
Usually absent
Potentially present
Potentially present
Potentially present
Potentially present
Smokers, COPD,
Heart failure / Cystic fibrosis
CXR, ABG, Blood/sputum cult.
Surgery, Immobility
Hypercoagulability
CXR, ABG, D-dimers
Risk factors
Investigations
The more useful distinguishing characteristics are in bold.
Tachypnoea + cyanosis are signs of respiratory failure
Pyrexia, rigors or prostration are signs of systemic disease – always take blood culture.
Community acquired pneumonia
Organisms enter lungs from external environment or nasopharynx - usually Gram +ve organisms
that are split into typical and atypical categories.
Typical
Usually caused by Strep pneumoniae,
moraxella catarhalis or Staph. aureus.
Atypical
Usually caused by Mycoplasma pneumoniae,
Chlamidia psitacci, legionella pneumophilla or
Coxiella burnetti.
Usually treated by amoxicillin 500g tds.
Usually treated by amoxicillin 500g tds +
erythromycin 1g qds
An abrupt onset suggests a bacterial agent. The gradual development of cough and fever in the
absence of pleuritic chest pain and respiratory distress suggests viral or mycoplasma pneumonia.
Management of community acquired pneumonia
Supportive: Oxygen, IV fluids and analgesia if required.
Investigations: Blood culture and sputum culture + MC&S before antibiotics
Immediate treatment with antibiotics (see above) before test results come back. Normally
combined oral antibiotics are sufficient. In severe cases (CURB positive) IV combination of
broad-spectrum antibiotic + macrolide e.g. cefuroxime 1.5g tds + clarithromycin 500mg bds
Background: The CURB system is a checklist for especially severe pneumonias
C: is confusion present where it was not before?
U: is there a urea >7 mmol.L-1
R: is the respiratory rate 30 or above?
B: is the systolic BP < 90 or diastolic <60?
7.7
If 1+ present: Admit
If 2+ present: IV antibiotics
If 3+ present: ITU
Chronic cough
Acute
Viral URTI
Pneumonia
COPD exacerbation
Foreign body
Investigations
Management:
Chronic
Asthma
Bronchitis
Bronchiectasis
Carcinoma
Diffuse parenchymal lung
disease
Drugs
Smoking
Rhinosinusitis
Gastro oesophageal reflux
Chest X-ray
Spirometry
CT
Haemoptysis
Bronchitis
Pneumonia
Bronchial ca
Bronchiectasis
Pulmonary embolus
False: epistaxis,
haemetemesis etc.
+ other rare causes e.g
Wegeners granulomatosis
Bronchoscopy
Oesophageal pH (GOR)
FBC if haemoptysis
Questions:
Onset, progression
Exacerbating / relieving factors
Esp. is it relieved by rest
Sputum production
Exercise tolerance
Recent temperature
Heart disease
Intermittant claudication
Angina
FULL occupational history
Any pets / animals (inc pigeons etc)
O/E remember:
Pallor
Cyanosis (peripheral / central)
Wheeze?: polyphonic or monophonic
Weight loss and progressive shortness of breath
Metastatic cancer from…
Breast
Stomach
Large bowel
Pancreas
Kidney
Female genital tract
Skin (melanoma)
Investigations
Management:
Primary cancer
Bronchial carcinoma
Squamous cell
Adenocarcinoma
Large cell
Small cell
Mesothelioma
Metastatic is more common
Chest X-ray
Sputum cytology / culture
Bronchoscopy
General
Oxygen
Analgesia
Nutritional supplements
Questions:
HPC
Classic lung ca. Symptoms:
Haemoptysis, cough, pain, anorexia
Sputum production
Night sweats (TB)
Symptoms of heart failure: PND,
orthopnoea, swollen ankles
PMH
Cardiac history
Any treatments for cancer
SH
Foriegn travel or visitors (TB)
FULL occupational history: asbestos,
chemicals, dyes, animals, farm work, coal
Any pets / animals (inc pigeons etc)
Smoking
Exercise tolerance
FH
Breast cancer
Non-Malignant
Congestive cardiac failure
Tuberculosis
COPD
Extrinsic allergic alveolitis
Percutaneous biopsy
CT/MRI chest / abdo /
pelvis
Specific
According to cause – see
below
O/E remember:
Respiratory examination plus
Horners syndrome
Signs of SVC obstruction: Swollen face
and arm; Engorged veins on chest;
Plethora; Cyanosis
JVP
Sacral and leg oedema
Bronchial carcinoma
The male:female ratio is 7:1; this ratio is decreasing as the incidence of bronchial carcinoma
in females is increasing.
The peak incidence of bronchial carcinoma is in the sixth decade in males and in the seventh
decade in females. It is rare before the age of 25 years.
Local effects
Horners syndrome from interference with the sympathetic nerve supply at the lung apex.
Partial ptosis, miosis (pupillary constriction) and anhydrosis (lack of sweating) on one side of
the face.
Hoarseness from interference with the recurrent laryngeal nerve.
Interference with the phrenic nerve causing paralysis of diaphragm with elevation of
diaphragm causing signs similar to effusion.
SVC obstruction from pressure on the superior vena cava (details later).
Systemic effects (non metastatic)
Cachexia
Anorexia
Fever
Anaemia
General Malaise
Paraneoplastic
Signs of metastasis:
Lymphadenopathy of supraclavicular
lymph nodes.
Hepatomegaly implying spread to liver.
Pathological fractures or tender spots
implying spread to bone.
Hemiparesis implying spread to brain
In many cases the cause of systemic effects is unknown but probably due to TNF and IL-1 from
inflammatory cells within the tumour.
Paraneoplastic effects are syndromes that are not directly the effect of the tumour concerned – it
is thought that they may arise due to autoantibodies to the tumour cells that cross-react with
normal tissues causing damage. Those associated with small cell carcinoma are:
Eaton-Lambert myasthenic syndrome: Muscle fatiguability with hyporeflexia; repeated muscle
contractions may lead to increased strength and reflexes; especially affects proximal limbs
and trunks; rarely affects eyes; autonomic involvement is common (e.g. dry eyes).
Syndrome of inappropriate ADH secretion (SIADH): hyponatraemia - potentially resulting in
confusion, seizures, hypotension, cardiac failure, anorexia, nausea, and muscle weakness.
Importantly there will be no oedema and urine osmolality will be >500 mmol / Kg.
Cushing's syndrome due to excess ACTH: Wt , anorexia, amennorhoea, hirsutism,
impotence, depression, weakness, fractures (osteoporosis), thin skin, purple striae, ‘buffalo
hump’, ‘moon face’.
Carcinoid syndrome from biogenic amines: paroxysmal flushing, D&V, abdo pain, CCF
(tricuspid incompetence and pulmonary stenosis).
All of these syndromes may have other causes.
Staging:
CT scan - useful for showing changes in the mediastinum, e.g. local spread of the tumour,
enlarged lymph nodes, and for showing secondary spread to the opposite lung which may be
too small to see on chest radiograph
PET – allows lymph node scanning – shows active lesions but can suffers from false
positives with e.g. TB
Barium swallow - may show oesophageal compression by enlarged mediastinal nodes
Bone scan
Histological classification of lung cancer
Small cell carcinoma
This is a highly aggressive, undifferentiated carcinoma, which grows rapidly and
metastasizes early. It accounts for about 20 - 30% of lung tumours.
Squamous cell carcinoma
This is the most common form of lung tumour accounting for 40 - 60% of cases. It is more
common in males and is the lung tumour most closely associated with cigarette smoking.
Adenocarcinoma.
Adenocarcinomata tend to occur more peripherally than squamous cell carcinomata (SCC).
Adenocarcinoma accounts for approximately 20% of lung tumours - though this may be
increasing - and with equal incidence in both sexes. The association with smoking is less
strong than for SCC.
Adenocarinoma is the most common lung tumour in non-smokers and the lung tumour most
frequently associated with asbestos.
Large cell
These account for some 10 - 15% of lung tumours and consist of sheets of large, round to
polygonal cells with large nuclei and prominent nucleoli. They frequently arise centrally and
are too poorly differentiated to be more precisely defined by light microscopy, and may be
squamous cell carcinomas and adenocarcinomas which are no longer recognisable.
Management
Non-small cell lung carcinoma (NSCLC): Curative treatment is surgical excision - lobectomy or
pneumonectomy. NICE recommend (Feb 2005):
Surgical treatment
Stages I and II
Surgical resection is recommended for patients with no medical contraindications and
adequate lung function
Lobectomy is the procedure of choice for patients who can tolerate it.
Limited resection or radical radiotherapy should be considered for patients who would not
tolerate lobectomy because of comorbid disease or pulmonary compromise.
Stages II and III
Complete resection is aimed for in patients with T3 NSCLC with chest wall involvement who
are undergoing surgery, by either extrapleural or en bloc chest wall resection.
Radiotherapy alone (stages I to III)
Radical radiotherapy is indicated for patients with stage I, II or III NSCLC who have good
performance status (WHO 0, 1) and whose disease can be encompassed in a radiotherapy
treatment volume without undue risk of normal tissue damage
All patients should undergo pulmonary function tests (including lung volumes and transfer
factor) before having radical radiotherapy
Chemotherapy for patients with NSCLC (stages III and IV)
Chemotherapy should be offered to patients with stage III or IV NSCLC and good
performance status to improve survival, disease control and quality of life
Chemotherapy should be a combination of:
A single third-generation drug (docetaxel, gemcitabine, paclitaxel or vinorelbine), plus a
platinum drug – carboplatin or cisplatin, taking account of their toxicities, efficacy and
convenience
Single-agent chemotherapy with a third-generation drug can be offered to patients who
cannot tolerate a platinum combination
Small cell lung carcinomas (SCLC) metastasise early so surgical treatment is not indicated. In
this case radiotherapy and combination chemotherapy is indicated. NICE recommend (Feb
2005):
Offer all SCLC patients multidrug platinum-based chemotherapy
If the disease responds, offer four to six cycles of chemotherapy. Maintenance treatment is
not recommended
If limited-stage SCLC then offer thoracic irradiation concurrently with the first or second cycle
of chemotherapy or after completion of chemotherapy if there has been at least a good partial
response within the thorax
If extensive disease then consider thoracic irradiation after chemotherapy if there has been a
complete response at distant sites and at least a good partial response within the thorax.
Prophylactic cranial irradiation should be considered for patients with limited disease and
complete or good partial response after primary treatment
For most cases treatment is palliative
Radiotherapy may be used to ease pain or bronchial obstruction and pleurodesis may be
indicated for recurrent pleural effusions
Palliative endoscopic laser therapy of obstructive lesions of large airways may also be
effective.
Superior vena caval obstruction
Symptoms:
Dyspnoea
Orthopnoea
Cough
Headache
Signs:
Swollen face and arm
Engorged veins on chest
Plethora
Cyanosis
Pembertons test: holding arm raised for >1min produces
JVP (non pulsatile), plethora / cyanosis, inspiratory stridor.
Management:
Sputum cytology, CXR,
CT, venography
Dexamethasone 4mg
QDS
Consider balloon
venoplasty / SVC stent
Palliative chemo / radio
COPD (by Ali)
Chronic Obstructive Pulmonary Disease
‘ A disease state characterised by airflow limitation that is not fully reversible.
The limitation is usually progressive and associated with abnormal inflammatory
response of the lungs to noxious gasses or particles’ 1
It may also be defined as the co-existence of Emphysema and chronic bronchitis, which
have their own definitions
COPD
Chronic Bronchitis:
Daily cough with sputum
For at least 3 m per year
For at least 3 consecutive
yrs
1
World health organization. www.who.int
Emphysema:
Enlargement of airspaces
distal to terminal
bronchioles with
destructive changes to
alveolar walls
Panacinar or centrilobar
Consider COPD in patients with:
COUGH
SPUTUM PRODUCTION
DYSPNOEA
SMOKERS
THE SCIENCE BIT (PATHOGENESIS)
2
There is chronic inflammation throughout the airways. In the larger airways (trachea, bronchi)
there is inflammatory cell infiltration of the surface epithelium. There is also increased mucus
secretion from enlarged mucus glands and increased numbers of goblet cells chronic,
productive cough. Tobacco smoke induced damage to cilia also contributes to the cough.
In the smaller airways (bronchioles), chronic inflammation narrows the lumen due to collagen
production and scar tissue formation fixed airways obstruction.
Airflow limitation, hyperinflation and gas exchange problems cause SOB. Pulmonary
hypertension, and cor pulmonale (right) heart failure are late consequences.
AETIOLOGICAL FACTORS
Smoking: Bronchitis mortality increases linearly with number cigarettes per day. Smoke
damages cilia, so ‘muco-ciliary ladder’ fails
Atmospheric pollution: e.g chemical factory workers
Alpha-1 antitrypsin deficiency: Recessive genetic inheritance, increased risk of early onset
emphysema (<40 yrs)
PRESENTATION
Productive cough, worse in mornings
Smoker
40+ years old
Increased frequency LRTI (e.g. H. influenzae)
Progressive dyspnoea +/- wheeze
Hyperinflation of the lungs (large chest)
Respiratory failure and right heart failure (Late complications)
Infections cause acute exacerbations, often requiring hospitalisation
INVESTIGATIONS
Respiratory function tests:
Spirometry: FEV1 <80% expected, FEV1:FVC (forced vital capacity) <70%, reduced peak flow
rate. Bronchodilators only give partial reversibility (if any).
Chest x-ray:
Good to exclude TB, carcinoma, pneumonia, pneumothorax
2
Rubenstein D, Wayne D, Bradley J. Respiratory Disease. In: Lecture notes on Clinical Medicine (6 th
edition). Oxford: Blackwell Science, 2003.
May be normal in COPD or…
May show:
Over-inflation with low, flat diaphragm
Bullae (enlarged small airspaces seen in emphysema)
Signs of pneumonia in acute exacerbations
Arterial Blood Gasses:
May be normal, or…
Reduced pO2 and increased pCO2, especially in acute exacerbations
Sputum:
Culture and sensitivity if suspect infection in acute exacerbation
Management
Drugs
B2 agonists: (salmeterol)
Anticholinergics: (ipratropium)
Theophylline
Inhaled steroids
Home oxygen
Antibiotics for infectious exacerbations
Flu jab annually ± other immunisations
However, medical treatments only provide
some symptomatic relief, as the disease is only
partially reversible
Physiotherapy
Rehabilitation
Exercise
Psychological support
Help giving up smoking
Counselling
Carer support
Assess severity to tailor treatment:
Stage 0: At risk- normal spirometry, cough
+ sputum present
Stage 1: Mild- FEV1:FVC <70%, FEV1=
80% with or without symptoms
Stage 2: Moderate- FEV1:FVC <70%,
FEV1 30-79% with or without symptoms
Stage 3: Severe: FEV1 <30% or <50% plus
respiratory failure or Right heart failure
Assess impact on daily living:
Climbing stairs
Walking on Flat
Dressing
What help is available at home
Tuberculosis
Pulmonary TB should be suspected in anyone with a cough of more than three weeks’ duration
for which there is no other explanation, particularly if it is accompanied by the other symptoms
and a history of travel to an endemic country (e.g. Pakistan, India).
Haemoptysis
Shortness of breath
Loss of appetite
Weight loss
Its incidence is highest in Black African (211 per 100,000), Pakistani (145 per 100,000), and
Indian (104 per 100,000) ethnic groups.
Signs may include any combination of consolidation, effusion, fibrosis and collapse, or none
at all. When lymphadenopathy occurs the lymph nodes may have a characteristically ‘matted’
feel.
Fever and sweating, especially at night
Fatigue and tiredness
Lymphadenopathy
Tuberculosis is suggested by the clinical and radiological features but requires the identification of
the tubercule bacillus. Such patients should be investigated urgently.
Chest radiography:
Look for the features of primary, post-primary or miliary tuberculosis
Always compare with previous radiology if possible
Sputum:
Take at least three samples including 1 early morning sample (NICE, 2006)
Ziehl-Nielsen or auramine staining of a sputum smear may demonstrate the presence of acid
alcohol-fast bacilli (AAFB)
In vitro culture of the sputum may take 4 to 7 weeks to provide a result; a further 3 weeks is
required to identify drug sensitivity
If clinical and radiological features are consistent with active disease, treatment is generally
indicated, even if sputum examination is negative – sensitivity ~50%
Biopsy:
Diagnosis can sometimes be made based on the histological demonstration of a caseating
granuloma
Tuberculin test:
Hypersensitivity to the tubercle bacillus is developed only about 3 weeks post initial infection
<6mm induration is considered negative
>6mm induration is considered positive
>15 mm induration is considered strongly positive
The Mantoux test is usually used
Management
Respiratory TB
2 months Rifampicin, Isoniazid, Pyrazinamide, Ethambutol* (Mnemonic: RIPE)
4 months Rifampicin, Isoniazid
Pyridoxine (Vitamin B6 - used to control the neuropathic side-effects of isoniazid)
TB meningitis (Significant morbidity)
Meningeal inflammation improves CSF penetration of drugs
2 months Rifampicin, Isoniazid, Pyrazinamide, Ethambutol
10 months Rifampicin, Isoniazid
Steroids
*Ethambutol may optionally be omitted in patients with a low risk of isoniazid resistance. Over
90% of new cases of TB are drug-sensitive and can be treated with standard therapy.
Background box: tests required before treatment
Since isoniazid, rifampicin and pyrazinamide are associated with liver toxicity, hepatic
function should be checked before treatment with these drugs. Those with pre-existing liver
disease or alcohol dependence should have frequent checks particularly in the first 2 months.
Side-effects of ethambutol are largely confined to visual disturbances in the form of loss of
acuity, colour blindness, and restriction of visual fields. Visual acuity should be tested by Snellen
chart before treatment with ethambutol.
Patient adherence to treatment for TB is a major determinant of treatment success.
Particularly vulnerable groups include:
The homeless
Those with learning difficulties, dementia or certain psychological illness
Those with a history of non-adherence
DOT (Directly Observed Therapy) may be one answer with the drug given three times per week
under observation – this should rarely be needed. Other mechanisms to increase adherence:
Ensuring the homeless / mentally ill have a known key-worker who is aware of their treatment
Home visits
Health education counseling
Reminder letters (in appropriate language)
As per NICE guidelines Feb 2006: http://www.nice.org.uk/page.aspx?o=CG033quickrefguide
7.12
Painful swollen leg
Commmon
Not common
Deep vein thrombosis
Arterial insufficiency (claudication)
Nerve root compression (sciatica)
Ishaemia
Cauda equina
Ruptured Baker’s cyst
Cellulitis (strep pyogenes)
Malignancy
Arthritis
Investigations:
D-dimers
ABPI if leg cold / absent
pulse
Ultrasound of leg /
Venography
Joint aspiration if ?septic
Clotting screen (pro-coag
ECG
state? Pre-management)
Glucose (DM)
Management:
Of DVT
Of Sciatica
Questions:
Onset, progression
Site, nature, duration
Exacerbating / relieving factors
Esp. is it relieved by rest
Recent temperature / SOB
Problems with joint movement
Recent trauma
Heart disease
Arthritis
Diabetes mellitus
O/E remember:
Temperature (cold = ischaemia - urgent)
Colour, joint swelling
Warmth
Pulses
Measure girth of both legs 15 cm above
and below knee to compare
Calf tenderness (usually +ve in DVT)
Palpate path of saphenous vein
Palpate for Baker’s cyst
Joint mobility
Sciatic N stretch test
Sensibility in feet / ankle jerks (may be lost
in cauda equina) – pain dist is S1-S3
Abbreviated cardiopulmonary exam for
sources of emboli / potential PE
For embolic source:
AF / murmurs
Signs of heart failure
Palpation for abdominal aortic aneurysm
For potential PE:
Heart rate
Resp rate
O2 SATS
Sciatic Nerve Stretch test (straight leg raise):
This used to be known as Lasegue's test. When this test is positive, it is generally suggestive of
an inflammation of the sciatic nerve as it comes out of the low back or lumbar spine. The patient
may experience low back pain or he may experience an "increase in intensity of pain" along the
back of the leg (sciatic nerve route). Low back pain only, may suggest a low back strain or sprain
as compared to a disc lesion.
The patient is lying on his back as pictured. Keep the leg straight, and
passively raise it as far as possible. Most patients can have the leg raised
almost straight up (90 degrees) without major pain. The patient with
"sciatica" will experience pain early in the movement of the leg. It is
important that you document at what level the patient's leg raise
maneuver caused him pain. It is generally recorded as 35 degrees, 65
degrees, or such. Repeat with the ‘normal’ leg
A scheme for determining the likelihood of DVT
The aim of this examination is to determine likelihood of DVT – this diagnosis cannot be excluded
or confirmed on clinical grounds alone but clinical examination forms an important part of the
scoring system.
History
Active cancer (treatment ongoing or within previous 6 mo or palliative)
Paralysis, paresis or recent plaster immobilization of the lower extremities
Recently bedridden >3 d or major surgery within 4 wk
Score
1
1
1
Examination Finding
Localized tenderness along the distribution of the deep venous system
Entire leg swollen
Calf swelling 3 cm asymptomatic side (measured 10 cm below tibial tuberosity)
Pitting edema confined to the symptomatic leg
Collateral superficial veins (nonvaricose)
If an alternative diagnosis as likely or greater than that of DVT (e.g. cellulitis / rupt.
Bakers cyst)
1
1
1
1
1
-2
In patients with symptoms in both legs, the more symptomatic leg is used. Pretest probability
calculated as the total score: high 3+; moderate 1 or 2; low 0.
An exam specific for arterial insufficiency
Peripheral Arterial Disease (PAD) includes disorders that obstruct arterial blood flow, excluding
the coronary and intracranial circulations.
There are several stages in the severity of PAD in the lower limb:
Intermittent claudication: pain, usually in the calf, that is precipitated by walking
Rest pain: pain, usually in the foot, that is worse elevated in bed at night and is relieved by
lowering the leg
Arterial ulceration of the leg and foot
Gangrene of the leg and foot
Rest pain, ulceration or gangrene indicates critical limb ischaemia. Critical limb ischaemia has a
high risk of amputation and death.
Look:
Skin pallor, dryness and discoloration
Loss of hair
Fissuring of nails
Venous guttering (the veins of the limb appear as shallow grooves or gutters, especially in
the elevated limb)
Ulceration
Gangrene
Feel:
Capillary refill time
HR and rhythm
Peripheral pulses
Skin temperature (cool foot in advanced arterial disease)
Abdominal palpation for abdominal aortic aneurysm (AAA) - with flat hand
Move:
Buerger's test
This used to assess the adequacy of the arterial supply to the leg. It is performed in two stages.
With the patient supine, elevate both legs to an angle of 45 degrees and hold for one to two
minutes. Observe the color of the feet. Pallor indicates ischaemia. It occurs when the
peripheral arterial pressure is inadequate to overcome the effects of gravity. The poorer the
arterial supply, the less the angle to which the legs have to be raised for them to become
pale.
Then sit the patient up and ask them to hang their legs down over the side of the bed at an
angle of 90 degrees. Gravity aids blood flow and colour returns in the ischaemic leg. The skin
at first becomes blue, as blood is deoxygenated in its passage through the ischaemic tissue,
and then red, due to reactive hyperaemia from post-hypoxic vasodilatation.
Both legs are examined simultaneously as the changes are most obvious when one leg has a
normal circulation.
Straight leg raise
As detailed above
Auscultation:
Of vessels for bruits
Of the heart for arrythmias, gallops and murmurs
Special Tests:
ABPI - Ankle-Brachial-Pressure-Index
The ABPI is taken with a hand-held Doppler and a blood pressure cuff.
It is the ratio of systolic pressure in the foot vessels (posterior tibial artery/ PT, dorsalis pedis
artery/ DP) to that in the brachial artery (very rarely affected by disease)
ABPI = ankle pressure/ brachial pressure
Normal = 1.0 - 1.2
Claudication < 0.8
Rest pain < 0.4
Note that this test is unreliable in diabetic patients due to calcification of the arteries
Special investigations:
FBC/ Hb - to exclude anaemia/ polycythaemia - anaemia may predispose to claudication
U&E's, ESR
Glucose to exclude diabetes
ECG to exclude associated coronary disease
Doppler ultrasound (to do the ABPI's) - biphasic signal is the norm in elastic arteries, but
becomes monophasic in hardened arteries.
Duplex scanning - combines structural (B-mode ultrasound) and functional (Doppler
ultrasound) information
Arteriography - used to locate the atherosclerotic disease and determine its extent.
9.1 & 2 Red Scaly Rash
Common
Psorriasis
Eczema / dermatitis
Atopic
Seborrhoeic (yeast)
Irritant contact
Allergic contact
Phototoxic
Investigations:
Management:
Less Common
Lichen planus
Lichen sclerosus
Pityriasis rosea
Pityriasis versicolour
Lupus erythematosus
Dermatomyositis
Tinea
Skin biopsy
Emmolients
Steroids
Questions:
Onset, progression, past treatments
Pruritis
Recent illness (guttate psoriasis)
What effect does sunlight have
PMH/FH atopy: asthma, hayfever, eczema,
Occupation
Gardening, crafts, etc.
Skin care routines. Frequency and
temperature of showers and baths; types of
cosmetics, soaps, oils, and products used.
Home remedies
Sun exposure
Stress (psoriasis)
Drugs
Comparison Chart:
Pruritus
Rash
Sites
Other signs
Systemic disease
Mycosis fungoides
Bowens disease
Solar keratosis
Pagets disease
Superficial BCC
Drug eruption
Patch testing (atopy)
UVA
Avoidance of triggers
O/E remember:
Nails for pitting, onycholysis
Eyes for redness
Natal cleft and genital area
Eczema
Yes
Red, ill-defined
Atopic: face, flexor surfaces
Seborr: Scalp, face, chest,
back, groin, axillae
Contact: anywhere – matches
exposure to contact
Psoriasis
Often not
Red, silver scales
Scalp
Extensor surfaces
Genitals
Natal cleft
Onycholysis
Nail pitting
Uveitis
Arthritis
9.3
Chronic lower leg ulceration
Common
Venous insufficiency (95%
of ulcers above malleolus)
Diabetes
Arterial disease
Trauma
Investigations:
Management:
Remember a hypersensitivity
reaction can occur from topical
drugs / dressings
Rare
Pyoderma gangenosum
(Crohns, UC, myeloma)
Vasculitis (RA, SLE, PAN)
Necobiosis lipoidica (DM)
Ca. (BCC, SCC, KS)
Renal failure
Doppler studies (ABPI)
Angiography
Local
Topical cleansing /
debridement
Compression if venous
Elevate limb at rest
Questions:
Onset, progression, past treatments
Fullness, aching, or tiredness in their legs
(venous stasis)
Diabetes
Crohns, UC, myeloma
RA, SLE, PAN
Non-healing
Diabetes
Peripheral artery disease
Malignant transformation
Associated with chronic
illness (as left)
Ultrasound (venous drain)
Skin biopsy
Systemic
Correct anaemia / oedema
Improve arterial supply
Treat malnutrition
Oral antibiotics
O/E remember:
Contact eczema
Venous / arterial insufficiency
Venous stasis
Cellulitis
Inguinal lymphadenopathy
Signs of venous stasis
Oedema of the legs and ankles.
The superficial veins in the legs may be varicosed,
A feeling of fullness, aching, or tiredness in their legs. These symptoms are worse
with standing, and are relieved when the legs are elevated.
Lipodermatosclerosis
Haemosiderin deposition (may be initially a blanching rash)
Eczema
Necrobiosis lipoidica
This is a dermatological condition that is associated with diabetes mellitus in 50% of cases. It
occurs in women three times more frequently than in men, usually in young adults or in early
adult life. It is an unusual complication of diabetes and not necessarily related to other vascular
complications that may occur in a diabetic patient. The pathogenesis is believed to be smallvessel damage.
Histological features include partial necrosis of dermal collagen and connective tissue. Also
there is a histiocytic cellular response.
This condition occurs more often in females. It usually affects young adults or middle-aged
patients.
Clinically, this is a very distinctive lesion that can occur on many parts of the body, but
normally is recognized on the lateral and anterior surfaces of the lower legs and rarely, the arms
and trunk. Over the shins, it may be mistaken for venous incompetence. The lesions may be
single or multiple, unilateral or bilateral.
This lesion may appear before the onset of diabetes, in its early stages, or long after the diabetes
has become a problem. There are three distinct clinical characteristics with these lesions.
The first is significant atrophy or loss of tissue substance with destruction of the hair follicle or
sebaceous glands.
The second characteristic is a thinning of the epidermis so that multiple telangiectatic vessels
(spider veins) can be seen, particularly at the periphery of the lesions.
The third sign is a yellowish or orange color in the central portion of the lesion, which
represents lipid deposits.
Necrobiosis lipoid diabeticorum lesions may become quite extensive and involve almost the
entire cutaneous surface of the pretibial area and can become extensive ulcerated lesions which
are extremely resistant to conventional therapy. Intralesional steroids therapy in the early stages
of this problem can be quite effective. However, as with any lesion associated with diabetes,
careful management of the blood glucose level is essential to create an environment where this
lesion can be effectively treated.
10.7
Visual problems in a diabetic
Causes of loss of vision in diabetic eye disease:
Vitreous haemorrhage (bleeding of extra blood vessels into the vitreous humor)
Tractional retinal detachment
Exudative maculopathy (+/- ischemia)
Neovascular glaucoma (overgrowth of new vessels onto the iris results in decreased
drainage of aqueous humour and so increased intraocular pressure)
Cataracts (cumulative exposure to blood sugar levels)
Investigations:
Slit lamp examination
U+Es
Intraocular pressure
Ultrasound eye / orbit
HbA1C
MRI eye / orbit
Management:
Photocoagulation (laser)
Questions:
Is there a loss of acuity (may be noticed
more in the light than dark with cataract)
Is it bilateral
How quickly did this develop
Does the patient suffer with ‘glare’
(cataract)
Is there any double vision (? Cataract)
Is there any pain
Type and duration of diabetes
Mode of treatment
Control (BMs / HBA1C)
Hypos? Aware before they occur?
Complications
Kidney disease
Foot ulcers / amputations
Infections
Hypertension
Coronary artery disease
Peripheral vascular disease
CVA / TIA
Hyperlipidemia
Background retinopathy
Diabetic maculopathy
Pre-proliferative retinopathy
Proliferative retinopathy
O/E remember:
Fundoscopy (remember red reflex)
Assessment of injection sites
Foot examination (pulses & sensation)
Assessment of cardiovascular risk and renal
function
Blood pressure, pulse
Hands, fingers (brown lines, splinters, nailbed infarcts)
Fluid status (abbreviated cardiorespiratory
exam + exclude pericarditis)
Are they ‘wet’ or ‘dry’
‘Abdomen plus’
Kidneys AND Bladder
Bruits (epig, femoral)
Urine test / BM
Microaneurysms (dot haem.)
Blotch haemorrhages
Hard exudates
Macula oedema
Loss of visual acuity
Cotton wool spots
Venous beading
Venous loops
Venous ‘nipping’ – uneven venous diameter
Vessels crossing in an unusual pattern –
normally tree-like in appearance
New blood vessel formation
Preretinal haemorrhage
Vitreous haemorrhage
Annual
screening
Urgent referral
ophthalmologist
Routine referral
to
ophthalmologist
Urgent referral
ophthalmologist
Advanced retinopathy
Retinal fibrosis
Traction retinal detachment
Urgent referral
ophthalmologist
Proliferation of vessels is a result of ischaemia which leads to release of VEG F which in turn
promotes growth of new vessels. Two main problems occur:
Vessels may grow outward into the vitreous body – these vessels may later suffer damage
through the shearing forces between vitreous body and retina.
Vessels may grow across the iris – called rubeosis iridis – by interfering with drainage of
vitreous through the trabecular network a large rise in intraocular pressure may result. This is
called neovascular glaucoma.
Feature
‘Cotton Wool’ spots
Cause
Axonal swelling
Exudate
Leak of lipid through
vessel wall
Blotch haemorrhages
Leak of blood through
vessel wall
Guidelines to Identify
White
Arranged radially around the optic nerve.
Yellow
May form a rough circle or ‘horseshoe’
with the point of leakage at the centre.
Red, roughly circular lesion.
10.8
Painful Red Eye
Causes: Commoner Rarer
Iritis: pain, moderate photophobia, red around cornea ±
small pupil
Keratitis: sharp pain, photophobia, watering; local redness
Scleritis: pain, may on movement; intense redness
Acute glaucoma: aching pain, vomiting, intensely red ±
large fixed pupil
Investigations:
Slit-lamp examination
Management:
Refer to eye dept.
Topical antiviral for
keratitis
Questions:
One or both eyes
Any discharge (sticky eyes in the
morning?)
Pain – SOCRATES
It it worse on movement
Nausea / vomiting
Photophobia
Loss of vision
History / family history of glaucoma
Systemic disease associated with iritis:
Ankylosing spondylosis
Behçet’s syndrome
Inflammatory bowel disease
Reiters disease
Sarcoidosis
Non-painful red-eye
Conjunctivitis
Bacterial (pusy discarge)
Viral (watery discharge)
Allergic (itchy)
Episcleritis (may be
painful)
Swabs if suspect
chlamidial conjunctivitis
Topical corticosteroid for
iritis / scleritis (CI in
keratisis)
O/E remember:
Should be a slit-lamp exam but you are
unlikely to have one or to be able to use it if
you do!
Intra-ocular pressure
Fluorescein for ulceration
Fundoscopy
Examine the conjunctiva and underneath
the upper lid – a foreign body may be
present.
Infections associated with iritis
Herpes simplex
Herpes Zoster
Lyme disease
Syphilis
Tuberculosis
10.1 & 11.1
Chronic headache; Acute severe headache; other headaches
Acute new
Meningitis* – headache, fever, neck
stiffness, photophobia, N&V
Sub arachnoid haemorrhage* –
‘thunderclap headache’ (very sudden &
very severe)
Encephalitis* – fever, confusion, decreased
level of consciousness
Head injury* – hx trauma, concussion
Acute sinusitis** - tender over sinuses;
usually follows URTI; worse on movement
or bending; ++ nasal discharge; fever
Subacute
Temporal arteritis: Mnemonic JEST
- Jaw claudication (pain worse on eating)
- Raised ESR
- Scalp tenderness
- Trismus due to pain
- >50 years
- Decreased visual acuity (rarely)
- Sudden uniocular visual loss
- Amaurosis fugax permanent blindness
Investigations:
Management: meningitis
ABC & admit immediately
Place head-up
1200 mg benzylpenicillin
by slow IV or IM1 g
Cefotaxime if penicillin
allergic
Dexamethasone
Acute recurrent
Migraine – aura or visual disturbance (not
in all cases); N&V; triggers. Classical
presentation is aura (10-30 mins) followed
by unilateral throbbing +/- N&V and/or
photophobia
Cluster headache – one eye painful, red
and watery. Headaches last 2-3 months
and then may disappear for up to 1yr +
Glaucoma – red eye; patient sees ‘haloes’;
loss of visual acuity.
Trigeminal neuralgia – intense stabbing
pains (seconds) in trigeminal nerve
distribution
Chronic
Tension headache – a constricting ‘band’
around the head; brought on by stress; low
mood.
Raised intracranial pressure – Cushings
triad +/- vomiting; papilloedema (blurred
disc)
Cervicogenic headache – neck to
forehead; unilateral / bilateral; scalp
tenderness.
Analgesia headache – rebound headache
after stopping analgesia
CT/MRI head
Blood cultures
Management: SAH
ABC & admit immediately
Observation / analgesia
Prevention of further
ischaemia: 3L fluids
minimum + nimlodipine
Prevention of re-bleed –
clipping of aneurysm
Questions:
Seizures (abscess / encephalitis / SAH or
possibly febrile in a young child)
ESR
LFTs
Management: migraine
Reassure
Identify and avoid triggers
Acute: sumatripan
Prophylaxis: propranalol
Management: Tension
Reassure
Stress reduction /
relaxation (?CBT)
NSAIDs
Amitryptaline 25-75 mg
O/E remember:
Temperature
Neck stiffness – kernigs test
Petechial rash
BP / Pulse pressure
Bradycardia
Focal signs: e.g. hemiparesis, hemianopia,
aphasia (abscess / encephalitis / SAH)
Neck
Stiffness
Meningitis
Triad
QuickTime™ and a
TIFF (Uncompressed) decompressor
are needed to see this picture.
Fever
Headache
An important physically
demonstrable sign of meningitis
is Kernig's sign. Severe
stiffness of the hamstrings
causes an inability to straighten
the leg when the hip is flexed to
90 degrees. The back of the
thigh muscle can be felt in
spasm.
Cushing’s triad is the triad of signs that may indicate raised intracranial pressure – papilloedema
is often cited but is a very late sign.
Pulse Pressure is the difference between
systolic and diastolic blood pressures
Widening Pulse
Pressure
Monroe-Kelly doctrine
Cushing’s
Triad
Sys BP
Bradycardia
The cranium and the vertebral body, along with
the relatively inelastic dura, form a rigid
container, such that the increase in any of its
contents --- brain, blood, or CSF --- will increase
the ICP. In addition, any increase in one of the
components must be at the expense of the other
two.
11.2
Pyrexia of Unknown Origin
Classically this is a fever >38.3 for 3 weeks including a week of unsuccessful investigations
Infections
Dissemiated
mycobacterial disease
Culture negative
endocarditis
Abscess
Pulmonary emboli
Investigations:
When completing a short
answer paper it may be worth
noting ‘ presuming FBC and
ESR have already been done’
and then list the other tests.
Management:
Neoplasm
Lymphoma
Leukaemia
Other haematologic
Solid (GI, Liver, Renal
cell)
Others
Drugs
FBC
ESR
D-dimer
MRI / CT abdomen
Echocardiography
Connective tissue disease
Temporal arteritis
Polymyalgia rheumatica
Polyarteritis nodosum
SLE
Systemic juvenile arthritis
Reduce drugs to minimum
Trial broad spectrum
antibiotics / anti / TB
Questions:
Patterns of fever: constant vs swinging
Foreign travel / visitors
HIV or other immunosuppression
Phenytoin
Antibiotics
Allopurinol
O/E remember:
Granulomatous dis. liver
Autoantibodies ANA,
ANCA, RF
Heaf test
Biopsy: temporal artery /
skin / liver / kidney / bone
marrow)
Trial corticosteroids if
infection / neoplasm
eliminated as possiblity
Psychiatric cases
The psychiactric history and the mental state examination – these are NOT the same thing –
the history is the story of how the complaint started and progressed the MSE represents what the
situation is NOW.
History
Mental State Examination
Mnemonic: PSP
A: Appearance
Premorbid personality (HARM)
Brainy: Behaviour
Hobbies
Senior: Speech
Attitudes to self and others
Medic: Mood
Reactions to stress
Seriously: suicidal ideation
Moral attitudes
Thought: Thought
Social (Social FROGs house)
Pete: Perceptions
Forensic / friends
Cog: Cognitions / memory
Recreational drugs
Got: General IQ
Occupation / money
It: Insight
God (religion)
Housing
Personal
The Mental Health Act (1983)
Section
2
3
4
5.2
5.4
Applies to
Patient in community, with a
suspected but undiagnosed mental
disorder*
Patient in the community, with a
diagnosed mental disorder*
A non-admitted patient, with
suspected or known mental
disorder* e.g. in A&E or
Outpatients dept.
An admitted patient with
suspected or known mental
disorder* e.g. a voluntary patient
An admitted patient with
suspected or known mental
disorder* e.g. a voluntary patient
Used by
Used For
Duration
Social worker + 2
doctors. One must be
section 12.2 approved
and the other should
ideally be a psychiatrist.
Assessment and
treatment
Up to 28 days
Treatment for 3 months
with further treatment
allowed with patient
consent or after
consultation with an
independent psychiatrist
Up to 6 months
Next of kin must be
informed in section 3.
Social worker + doctor
Doctor
Nurse with mental
health training
135
Person in a private dwelling
Police with a
magistrates order
136
Person in a private dwelling
Police
Detaining a patient who
wishes to leave until
formal assessment under
section 2 or 3. No
treatment can be given
without consent.
72 hours
72 hours
6 hours
Removal of person to a
‘safe place’ to await
formal assessment under
section 2 or 3. No
treatment can be given
without consent.
72 hours
72 hours
*causing such severe problems that they are a risk to their own health or the health and safety of others,
refusing to be hospitalised.
There is a right to appeal against sections 2 and 3, usually taking 1-2 weeks or 4-5 weeks
respectively to resolve.
12.1
Depression
Psychiatric
Depression
Post-natal depression
Bipolar disorder
Dysthymia
Bereavement reaction
Investigations:
Management:
Organic
Drug (esp stimulants)
and/or alcohol misuse
Hypothyroidism
Cushing’s or Addison’s
(inc side effects of
steriods)
B12 or folate deficiency
Tox screen
Serum B12 / folate
TFT’s
CBT
Antidepressant
Mood stabiliser (bipolar)
Questions:
Duration (2+ years may indicate dysthymia)
Periods of mania (delusions of grandeur,
high libido, spending wildly) – even one
such period means the diagnosis is not
depression – rather it is bipolar disorder
Recent childbirth
Previous depression
Family history depression
Recreational drug and alcohol history
Steroid usage
Ideas, concerns and expectations
Organic
Renal or hepatic
impairment
Stroke (cva)
Parkinson’s Disease
Rare: MS, HIV, SLE, RhA
Head injury
LFTs and GGT
U+Es
CT / MRI head
Drug programme
Social issues
Treat organic cause
O/E remember:
Mnemonic: SEWS CLAW
SUICIDAL IDEATION – Forgetting this is
probably an automatic ‘E’ grade
Past attempts
Planned methods
Suicide notes
Energy loss / fatigue
Significant Weight loss or gain
Change in sleep patterns (early waking,
insomnia, hypersomnia)
Concentration poor; indecisive
Low mood
Anhedonia
Feelings of worthlessness
2 or more, most days of the last 2 weeks justify
major depression as a diagnosis – less are
needed for minor depression
Signs of psychosis
Signs of anxiety
Cognitive behavioural therapies emphasise a circular relationship between thoughts,
behaviours and feelings and a persons behaviour is believed to be determined not just by the
situation but how the individual perceives it.
Behavioural techniques are based upon the works of
Skinner: operant conditioning as used in self-reinforcement
Pavlov: classical conditioning e.g. in antabuse therapy
Bandura: modelling. It has been shown that a video of children experiencing slight, short
lived pain can decrease pain in children having injections or blood taken. Alcoholics
anonymous is another example where a new member models behaviour on existing
members.
The thought-behaviour-feeling cycle is:
The goals of CBT are:
Eliminate maladaptive behaviour and
replace this with more healthy behaviour
Modify maladaptive thoughts and develop
more adaptive responses
CBT focuses on the present rather than the
past – the cause of an illness is unimportant
compared to the cure.
Trigger
Thought
Behaviour
CBT can be used for many things - some
common applications are:
Depression – more effective than any other
psychological intervention but not superior to
Feeling
antidepressants.
Anxiety (including phobias but ineffective
with agoraphobia). Systematic desensitisation and exposure reduce symptoms in 25-80%.
Obsessive compulsive disorders: CBT is rarely completely successful but about 75% of
patients show a 30-50% improvement.
Eating disorders – mainly BN (75-80% symptom reduction) but CBT is not superior in this
field (interpersonal therapy, IPT is also good) – there is poor evidence of its effects on AN.
Psychotic symptoms such as hallucination or delusions. The idea is to challenge and
invalidate delusions – argument with the patient is not used but questioning may help the
patient realise the inconsistencies in their beliefs. This works better with isolated beliefs and
is hard to use with complex webs of beliefs, as these are hard to challenge.
CBT techniques
Psychoeducation
Education about thought-behaviour-feeling cycle
Education specific to the disorder suffered to help understand symptoms
Behavioural techniques (these tend to be quicker than cognitive techniques)
Systematic desensitisation: relaxing through deep breathing and muscle relaxation in the
presence of a stimulus that would normally produce stress – starts with slightly stressful
stimuli and move up a hierarchy of stressful situations.
Visual imagery
Distraction
Delaying
Self-reinforcement via goal setting: self reward when a goal is met. For example going to
the movies after a day of non-smoking.
Cognitive techniques
Self monitoring: the identification of target behaviour, its frequency and what stimuli produce
it (people, times, places)
Stimulus control: the identification of stimuli for a maladaptive behaviour and the removal of
that stimuli (e.g. the removal of snack food from the house) or the use of a stimulus to
provoke an adaptive behaviour (a picture of miss piggy on the fridge)
Cognitive restructuring: Guided remodelling if internal dialogue from maladaptive (e.g. I
cannot cope with this) to coping (doing this and this will help).
Limitations of CBT
Limited benefits if problems are diffuse
Rely on cooperation and motivation from the patient – often away from the therapist as in
diaries / homework etc.
May require a degree of ‘psychology-mindedness’ from the patient
Not very useful with very rigid though processes
Antidepressant
Citalopram: SSRI
Dose: 20-60 mg PO OD
S/E: Cardiovascular; ENT; Neuro; Genitourinary; Psych
Palpitation
Coughing,
Polyuria,
Tachycardia
Yawning,
Micturition
confusion,
disorders,
Postural
hypotension
Impaired
Euphoria;
concentration,
taste
Paradoxical
disturbance
increased
Malaise,
anxiety during
Increased
Amnesia,
initial treatment
salivation
Migraine,
of panic
Rhinitis
Paraesthesia,
disorder
Tinnitus
abnormal
(reduce dose)
dreams,
12.2
Anxiety state
Obsessive compulsive disorder
Obsessions and compulsions are:
Intrusive
Senseless
Obsession
Repetitive
Compulsion
A thought or mental image e.g.
Contamination
Sex, violence
Numbers
An action that must be performed e.g.
Handwashing
checking
touching
If the obsession or compulsion is resisted then anxiety mounts until the activity is performed.
Psychiatric
Anankastic personality
Depression
Post-natal illness
(thoughts of syndrome
harming baby)
Tourettes
Psychiatric
Schizophrenia
Generalised anxiety
disorder
Phobia
Investigations:
Management:
Tox screen
Serum B12 / folate
TFT’s
CBT
Antidepressant
Mood stabiliser (bipolar)
Organic
Temporal lobe epilepsy
Hyperthyroid (anxiety)
Hypothyroid (depression)
Dementia
Parkinson’s disease
Head injury
Huntingdons
Encephalitis
LFTs and GGT
U+Es
CT / MRI head
Drug programme
Social issues
Treat organic cause
Anankastic personality disorder is one differential and is characterized by:
Perfectionism
Excessive cleanliness
Rigidity of thinking
Orderliness
Moralistic preoccupation with rules
Tendency to hoard
Other differentials include:
Depression
Puerperal illness (harming
baby)
Questions:
Always ask how often a symptom occurs
and how long it lasts
Do you find that some thoughts come into
your mind even if you try not to have them?
Do you have any thoughts, ideas, words or
pictures that come into your head and you
cannot stop?
O/E remember:
Mnemonic: SEWS CLAW
SUICIDAL IDEATION – Forgetting this is
probably an automatic ‘E’ grade
Past attempts
Planned methods
Suicide notes
Signs of depression (SEWS CLAW)
What is it like?
How do you explain it?
Are there things you have to do even
though you know they seem silly and
unnecessary?
Do you have to keep checking things?
Do you get worried about germs or have to
wash your hands a lot?
Do you ever have to repeat actions?
What happens if you do not do these
things?
Ideas, concerns and expectations
Situational vs general
Signs of anxiety
12.3
Psychosis
The term psychosis has no generally agreed meaning. The psychotic symptoms are generally
perceived as disturbances in perception (hallucinations) and in thought content (delusions).
There is generally a lack of insight – the patient is unaware that they are ill.
Psychiatric
Schizophrenia
Schizoaffective disorder
Major depression
Mania / bipolar
Psychiatric
Recreational drug use
Drug withdrawal
Drug induced psychosis
Delusional disorder
Paranoid disorder
Investigations:
Management:
Full MMSE
Tox screen
Treat organic cause
Antipsychotic
Social worker
Organic
Temporal lobe epilepsy
Space occupying lesion
Dementia
Head injury
Encephalitis
SLE / HIV
LFTs and GGT
CT / MRI head
Assertive case
management
CBT
Schizophrenia is the most common disease in this ‘group’ - Schneider described symptoms that
are each individually sufficient for a diagnosis of schizophrenia to be considered (about 8% will
have another diagnosis – see above).
Incidence: 15-20 / 100k; M=F; peak incidence teensearly adulthood.
Schneider’s first rank symptoms
Chronic phase schizophrenia
Auditory hallucinations in 3rd person or a
running commentary
Somatic hallucinations
Thought beliefs: thought insertion,
withdrawal, broadcast, hears thoughts
spoken aloud
Delusional perception.
Passivity phenomena (feeling of actions
being controlled)
Not first rank but diagnostically useful
Delusions of persecution / grandeur
Ideas of reference
2nd person auditory hallucinations
Mnemonic: APHID PIT
A: Auditory hallucinations (2nd / 3rd person)
P Passivity phenomenon
H Hallucinations of body (somatic)
Insersion / withdrawal of thoughts
I
Those in bold are First Rank
D
P
I
T
Apathy, poor motivation
Social withdrawal
Blunted affect (decreased emotional
expression)
Decline in skills associated with activities of
daily living (ADLs) e.g. hygiene, budgeting,
cooking etc.
Cognitive impairments: concentration and
memory deficits
Frontal lobe deficits: inability to formulate
and execute complex plans
Thought disorder: derailment
Delusional perception
Paranoia
Ideas of reference
Thought: broadcast, spoken aloud
Hypomania / mania:
Primary delusional disorder
can present with psychotic symptoms including 40% who
present with a first rank symptom e.g.: ideas of reference,
3rd person hallucinations, and/or delusions of persecution
(e.g. doctor is jealous of patient’s ‘greatness’). These are
hard to distinguish from schizophrenia but a distinguishing
feature is that the psychotic symptoms rarely persist outside
the overactive phase and change quickly in content. In the
manic phase, pressure of speech is common as are such
behaviour as dramatic indulgence in overspending or sexual
behaviour. Prevalence is 0.1-0.6 / 1000 c.f. 10/1000 for
schizophrenia. In schizophrenia there may be mood
incongruence.
there are five types listed in DSM-IV. Auditory and visual
hallucinations (if present) must not be prominent and symptoms
must have been present for at least 1 month (3 in ICD-10). The
five types are:
Persecutory
Jealous (‘Othello’ syndrome): an abnormal belief that the
partner is being unfaithful – held on irrational grounds
(unsound evidence and reasoning) and unaffected by
rational argument. Often there is no idea who the supposed
lover might be. M>F
Erotomanic (rare): the belief that a (usually inaccessible)
person is in love with the patient. The person is often
famous. F>>M
Somatic: The belief that the patient suffers from a physical
disease or deformity.
Grandiose
Useful Questions to ask in history taking
Always ask how often a symptom occurs and how long it lasts
Mnemonic: APHID PIT
Auditory hallucinations
Have you ever heard anything you believe other
people cannot?
Do you hear voices?
Whose voices are they?
Are they clear?
How many are there?
Do they come from inside or outside your head?
Do they talk to you or about you?
What sorts of things do they say?
Do they give commands?
Do you have to obey them?
Other hallucinations:
Do you ever see, feel or smell something that you cannot
explain?
Passivity
Are you always in control of your thoughts and
actions?
Who else controls these?
How do they do this?
What do they get you to do / think / say?
Hallucinations of body (somatic)
Have you had any strange or unusal feelings in your
body?
Does your body function normally?
Insertion / withdrawal of thoughts
Are thoughts put into your head that you know are not
your own?
Where do they come from?
Do your thoughts disappear or seem to be taken from
your head?
Where do they go?
Delusional perception:
When you saw … how did you know what it meant?
Delusions
Have you experienced anything strange or unusual?
Paranoia
Ideas of reference
Do you get messages that no-one else does from the
TV, radio, or newspapers
Thought block / broadcast
Do your thoughts sometimes stop suddenly so your
mind is blank even though your thoughts were flowing
freely before?
Why does this happen
Do others hear your thoughts or read your mind?
Can you send messages to other people with your
mind?
How do you explain this?
Management
Assertive Case Management (Care Programme Approach)
Aims to prevent people falling through the net
Multidisciplinary care (Dr, CPN/ nurse, SW)
Named care coordinator
Multiple domains: Bio – Psycho – Social
Importance of involving families and carers.
CBT may be used for psychotic symptoms such as hallucination or delusions. The idea is to
challenge and invalidate delusions – argument with the patient is not used but questioning may
help the patient realise the inconsistencies in their beliefs. This works better with isolated beliefs
and is hard to use with complex webs of beliefs, as these are hard to challenge.
Antipsychotic
Risperidone: D2 antagonist
Dose: 4-6 mg PO OD
(max 16 mg) – behaves more
like a typical antipsychotic with
extrapyramidal S/E at higher
doses)
S/E: Antimauscarinic, Extrapayramidal
Antimuscarinic
Dry CHAT
Dry mouth,
eyes, skin
Constipation
Headache
AF / angle
closure
glaucoma
Tachycardia
Extrapyramidal
AdAPT
Acute dystonia
Akathisia
Parkinsonism
Tardive
dyskinesia
Extrapyramidal side effects (mnemonic ADAPT)
Effect
Seen in
Description
Acute Dystonia
Days
Abnormal face and body movements, most common in children
and young adults.
Akathisia
Weeks
Restlessness, with limbs in constant movement. May be
concealed by activity such as walking. Very poorly tolerated by
patients.
Parkinsonism
Weeks
May be suppressed by antimuscarinic drugs
Tardive
dyskinesia
Years
Rhythmic, involuntary movements of tongue, face and jaw. May
decrease upon drug cessation but may not – very socially
disabling.
Neg symptoms
FACTORS
Frontal lobe defects
Apathy
Cognitive / concentration decrease
Thought disorder: derailment / disorganised
ADL go down
Withdrawal
Emotional bluinting
Skills of life down: memory , thinking, planning
Poverty of speech
12.5
Dementia
Global impairment of cognition with normal levels of consciousness
In ACS the level of consciousness is impaired
Causes of dementia
Alzheimer’s disease
Vascular (multi-infact)
Frontotemporal
Late Parkinson’s disease
Lewy body dementia
In a young patient
HIV
Vasculitis
New variant CJD
Similar symptoms
Depression
Uncontrolled epilepsy
Organic problems
Intracranial tumour
Subdural haematoma
Normal pressure
hydrocephalus
Hypothyroidism
Chronic severe Na+
B12 deficiency
Neurosyphilis
Vasculitis
Paraneoplastic syndromes
(rare)
Diagnostic criteria
Investigations:
Management:
CT / MRI head
Syphilis serology
Anticholinesterase
inhibitors (MMSE 12-26)
Memory training
Orientation
Memory loss (amnesia) + one of the
flowing:
Apraxia: problems with
movements as evidenced by the
drawing part of the full MMSE
Agnosia: problems in
recognition e.g. faces, names etc
of friends or relatives
Aphasia: problems in speech or
communication, either fluent or
non-fluent
Associated symptoms: e.g.
problems planning
These are the 5 ‘A’s
In addition, there should be a decline
in function over time and should
cause problems in social or
occupational operation.
B12 / folate levels
TFTs / FBC / U+E / LFT
Home help
Day care / respite
Power of attorney
Reminiscence therapy
Patients should be told about enduring power of attorney in the early stages of dementia. They
can choose a relative to take this power for them over their estate for when they are
incapacitated. If left until later this can be drawn out and expensive in the courts and may not
result in the patient getting who they wanted.
Questions:
Onset
Sudden: infact / subdural haematoma
Stepwise: Vascular
Gradual: alzheimers or other
Focal neurology
Falls: common in Lewy body
Hallucinations: common in Lewy body
Loss of inhibitions: frontotemporal
Poor decision making: frontotemporal
Triggers: CVA/ injury etc.
Past medical history
Thyroid, Vasculitis, Syphilis
Family history of dementia / huntingtons
Dietary variety: B12, folate, sodium
O/E remember:
I would like to perform a full MMSE and
examine for potential organic causes including
focal neurology and gait examination
Gait: Parkinsonian in PD and possibly in
Lewy body. Small steps in vasculitic.
MMSE
Pulse
BP
Anaemia
Cranial Nerves
Jaundice
Thyroid
Abreviated MMSE
Remember these three things: Cat, Ball,
Potplant
What is your full name (1)
Where are you now (1)
What is the year (1)
What is the month (1)
What day is it (1)
How old are you
Who is the prime minister (1)
When did WWII start (1)
Count backwards from 20 (1)
Name the three things I asked you to
remember from earlier (1 each)
8+ Normal, 4-7: mild-mod dementia, <4 severe
10.7
Full MMSE
Space: Country, county, city, building, floor
(1 each)
Time: Year, Season, Month, Date, Day (1
each)
Repeat and remember: Cat, Ball, Potplant
(1 each)
Concentration: Spell ‘world’ backwards
(5)
Recall: Cat, Ball, Potplant (1 each)
Repeat: NO IFS ANDS OR BUTS (1)
What are these two objects (1 each)
Following commands: (1 each)
Take paper in right hand
Fold in half
Place on the floor
Write a sentence (1)
Read a sentence and do what it says
(Close Your Eyes) (1)
Copy the shape (1)
Acute confusional state (ACS)
Global impairment of cognition with impaired levels of consciousness
Differentials for acute confusion
12.5
Substance abuse
Alcohol abuse and dependence
Alcohol abuse and dependence covers 3 main ICD-10 diagnoses (DSM-IV differs slightly in some
regards)
1. Excessive alcohol consumption
2. Harmful use
3. Alcohol dependence
Excessive consumption:
Low risk of problems
Increasing risk – esp in smokers
High risk – esp in smokers
Can of beer = ~1.5 units
Pint of cider = ~3 units
Males (units / week)
0-21
22-50
>50
Pint of beer = ~2 units
Bottle of wine = ~7 units
Females (units / week)
0-14
15-35
>35
Pint of strong beer = ~4 units
Bottle of spirits = ~30 units
Harmful use:
A pattern of use that is causing damage to the health. Actual physical (e.g. cirrhosis / hepatitis) or
psychological (e.g. depression) damage must have occurred. Acute intoxification / hangover is
not sufficient.
Dependence:
There are six ICD-10 elements to dependence – a useful mnemonic is:
D
Drink
Difficulty controlling: starting, stopping, quantity
S
Starts
Strong desire to drink (or a sense of compulsion)
W With
Withdrawal – physiological symptoms. Are these relieved by drinking?
T
Totally
Tolerance – needing more alcohol for the same effect
N
Normal
Neglect of other interests
P
People
Persistant use despite evidence of harm
At least three of these must have been present at the same time within the last year.
A commonly used factor that increases the likelihood of dependence being present (but is not
itself diagnostic) is a narrowing of the drinking repertoire.
Useful questions to ask in history taking: (D, S, W etc. relate to the elements above)
The basics
Do you ever drink?
How often do you drink?
How many drinks do you have on a typical
day? What time do you start drinking?
What do you drink? Where?
The CAGE questionnaire is a screening
tool – two or more positive answers
indicates a good possibility that the patient
has a problem with alcohol abuse.
CAGE
Have you ever though you should Cut down on your drinking?
Have people Annoyed you by criticising your drinking?
Have you ever felt bad or Guilty about your drinking?
Have you ever needed a drink Early in the morning to steady your nerves or get rid of a
hangover.
Should you use CAGE in an exam?
This will depend very much upon your ‘brief’: CAGE is a screening tool. If you have been told
that the patient has alcohol dependence then it may be argued that CAGE should be left out as
you already know this patients problem. The DSWTNP questions below will establish the
diagnosis more accurately anyway.
A more difficult problem is ‘Mr Smith has an alcohol problem, investigate this’. Here the
problem could be excessive use, harmfull use or dependence. Once again I would advocate
using DSWTNP and leaving out CAGE though you must obviously make your own choice.
Establishing the problems
(D) Do you ever have problems with drinking more than you intended?
(S) Do you feel you really need a drink if you go too long without one?
(S) How long is this?
(W) Do you get any physical symptoms if you don’t drink for a few days?
(T) Does it take a lot to get you drunk?
(N) How important compared to other things is drinking?
(P) Has your drinking ever led to problems with work, family, friends or the police?
(P) Have you ever had any money problems due to drink?
(P) Have you ever had any illness due to drink?
(P) Did you continue drinking?
Alcohol abuse questions:
Current use (see above)
History of alcohol use
Consequences of alcohol use (see below)
Complications
Acute intoxication
Slurred speech
Impaired
coordination and
judgement
Labile affect
Acute withdrawal
Medical
Within 1-2 days of Hepatitis
abstinence
Cirrhosis
Malaise
Oesophageal
Nausea
varices
Hyperactivity
Pancreatitis
Tremulousness
Peptic ulcer
If severe
Labile affect
Gastritis
Hypoglycaemia
Insomnia
Cardiomyopathy
Stupor
Transient illusions Hypertension
Coma
or hallucinations
Anaemia
Seizures
Throbocytopaenia
There are also social side effects – may be remembered as the ‘3 Ls’
Livelihood: job loss
Love: problems with relationsips and family
Legal: prostitution, criminal activity, road accidents
Neuropsychiatric
Wernicke’s
2° to thamine
deficiency
Ataxia
Nystagmus
Ophthalmoplegia
Korsakov’s
Profound loss of
short term
memory
Acute confusion
Cerebellar degen.
Depression
Anxiety
Hallucinations
Prognosis:
15%
30%
10%
25%
20%
Suicide
Lifetime complications
Improve
Recover
Lost to follow-up
Management
Pabrinex
Chlordiazepoxide
Support groups
Substance abuse
Substance abuse questions:
Current use
History of drug use
Consequences of drug use
Current use:
Which drugs are being used? Include prescription drugs.
How often?
By what route?
What effect are you seeking? e.g. excitement, calmness, relief of cravings
What happens if you don’t take the drug for a while? (withdrawal, cravings)
Do you take risks? (needle sharing, unsafe sex, sex for money/drugs)
How do you afford your drugs?
History of drug use:
How old were you when you first started to take drugs?
When did you start using them regularly?
How often were you using drugs?
What drugs did you move on to?
Why did you continue / change?
What is your favourite drug?
Where do you get your drugs from?
Have you ever gone without drugs for a long while?
Why did you start again?
Consequences:
Have you ever worried about HIV or hepatitis?
Why? / Why not?
Have you ever had any tests for these?
Have you ever had any injecting problems (DVT, septicaemia, abcess)
Have you ever OD’d by accident?
Have you ever seen or heard things that were not there?
Have you believed strange things?
Have you been drowsy or confused?
Any other problems?
Stages of Change (Transtheoretical model)
Prochasta and DiClemente (1982) after analysis of
18 therapies.
4
3
2
5
1
There are five stages of change
1: precontemplation (no plans to change)
2: contemplation (considering change)
3: Preparation (making small changes)
4: Action (engaging in new behaviour)
5: Maintenance (sustaining change)
Individuals will focus on either the costs of benefits of the behaviour dependent upon which stage
they are at – the first two stages tend to focus on costs involved while the last three on benefits.
Stage
Precontemplation
Contemplation
Preparation
Action
Maintainance
Relapse
Intervention
Harm minimisation (e.g. needle exchange)
Motivational interviewing, leaflets
Practical help in starting their changes e.g. detox, CBT, help finding
work etc.
Ongoing support, regular contact and encouragement
Reassure that is normal and provide help / support to start again
The stages do not always occur in a linear fashion and an individual may ‘slip back’ to an earlier
stage several times.
The model predicts:
- Smoking
- Alcohol use
- exercise
- Screening behaviour
Criticisms of the model
Changes between stages can occur so quickly that the stages are unimportant
Successful interventions may result from the individuals belief that they are receiving ‘special
care’ rather than effectiveness of the model.
It has only been studied with cross sectional studies – experimental or longitudinal studies are
needed to demonstrate causality
13.1
An elderly person who has recurrent falls
Medical
Visual impairment: myopia, cataract,
Cardiovascular: hypotension, arrhythmia, syncope
Nervous system: sciatica
Musculoskeletal: arthritis, leg length discrepancy, joints
Gait / balance: Parkinsons’s disease
Medications which induce sleepiness
Investigations:
Urine dipstick
Acuity / fundoscopy
Walking assessment
Management:
Risk assessment at home
Medications review
Questions:
Mnemonic: CATASTROPHE
C
Caregiver and housing
A
Alcohol (including withdrawal)
Treatment (i.e., medications, including
T
compliance)
A
Affect (depression or lack of initiative)
S
Syncope (any episodes of fainting)
T
Teetering (dizziness)
R
Recent illness
O
Ocular problems
P
Pain with mobility
H
Hearing (necessary to avoid hazards)
Environmental hazards
E
Ideas, concerns and expectations
Exploring mood and social history are vital
Environmental
Slippery surfaces
Uneven flooring
Poor lighting
Tripping obstacles
Unstable furniture
Poor footwear
OT assessment
Nutritional state assesmnt
Physiotherapy
Walking aids
O/E remember:
Mnemonic: I HATE FALLING
I
Inflammation of joints (or joint deformity)
H Hypotension (orthostatic BP changes)
A Auditory and visual abnormalities
T Tremor (PD or other causes of tremor)
E Equilibrium (balance) problem
F Foot problems
A Arrhythmia, heart block or valve disease
L Leg-length discrepancy
Lack of conditioning (generalized
L
weakness)
I
Illness e.g. UTI
N Nutrition (poor; weight loss)
G Gait disturbance
Fall prevention:
Physical activity to improve strength, mobility and flexibility in seniors;
Limiting sleep-inducing medications whenever possible;
Appropriate treatment of underlying medical conditions;
Environmental modifications such as installing grab bars, removing tripping obstacles, and
maintaining sufficient lighting;
Hip protectors do not reduce the risk of falling but can significantly reduce damage