Public Health Notification to Canadian Blood Services
advertisement

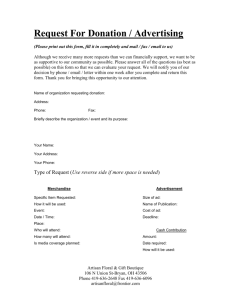
Alberta Health Public Health Notification of West Nile Virus to Canadian Blood Services SECTION 1: DONOR/RECIPIENT INFORMATION Last Name: First Name: Birth Date (yyyy-mm-dd): Address: City: Province/Territory: AB Onset Date: Suspect West Nile Neurological Syndrome (WNNS) Classification: Probable/Confirmed West Nile Non-Neurological Syndrome (WN Non-NS) Test Result Negative Probable/Confirmed WNNS Confirmed West Nile Asymptomatic Infection Date of Test: Positive (Please attach copy of WNv laboratory result) SECTION 2: DONATION HISTORY History of blood DONATION in the 56 days (8 weeks) prior to onset of symptoms? Yes CBS Donor Number (if available): 1. City of Donation: Name at Time of Donation: 2. City of Donation: Name at Time of Donation: No SECTION 3: RECIPIENT HISTORY History of blood/blood component TRANSFUSION in the 56 days (8 weeks) prior to onset of symptoms? Yes No If Yes, please provide dates and location: 1. Hospital: Town/City Transfusion Date: Name at time of transfusion: 2. Hospital: Town/City Transfusion Date: Name at time of transfusion: 3. Hospital: Town/City Transfusion Date: Name at time of transfusion: SECTION 4: ADMINISTRATIVE INFORMATION Date Reported to CBS: Reported by: Zone/Region reporting: Zone - Region Telephone number: - ext COMMENTS: Forward completed information to the CBS by phone and fax: Calgary Edmonton (24 hrs) Mon – Fri, 2100 – 0800 hrs Sat & Sun after 1600 hrs Mon – Fri, 0800 – 2100 hrs Phone: 780-431-0777 Phone: 403-410-2737 Phone: 403-589-3399 Fax: Fax: Fax: 780-433-4478 Surveillance and Assessment Updated August 27, 2012 403-410-2791 403-410-2791