Using Remote Instruction to Improve Knowledge and Skills
advertisement

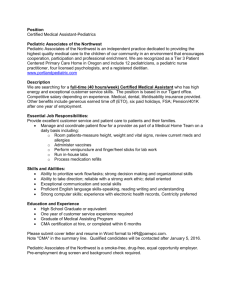
Extended Abstract Using Remote Instruction to Improve Knowledge and Skills Jeri Pullum, MS D. Breck Rushton, RN, MPH This pilot test was designed to improve the pediatric airway management and positioning knowledge and skills for emergency medical technicians working in a rural ambulance service. Problems with pediatric airway management and positioning are well documented in the literature. Rural EMTs typically receive some training in pediatric care, but low call volumes, especially in rural areas, provide few opportunities to practice their skills or use their knowledge.1,2 Knowledge and skill deterioration is well documented in EMS.3,4,5 Although training is often advocated to retain knowledge and skills,6,7,8, 9 high-quality local training is not always available. The Pediatric Emergency distance learning program included self-study materials contained on an Internet World Wide Web site, in published textbooks, and on interactive CD-ROM programs. The training was conducted by an instructor in Salt Lake City, UT, who communicated with 9 prehospital providers, aged 20-59, in Fort Benton, MT, using E-mail and desktop video conferencing. The instructor reviewed and critiqued videotapes Performance Scores of the ambulance crew members’ performance skills taped before the training began. The 60 performance skill required participants to assess and provide care for a pediatric trauma patient 50 in a simulated emergency. The providers took a written test, filled out a questionnaire to measure self-confidence, and completed the performance test before and after the training. Quantitative data showed statistically significant improvement in performance but no change in either written knowledge or self-confidence. 40 30 20 10 0 Pretest Posttest During a focus group meeting and personal interviews, the ambulance crew members Pretest performance scores range: 19.67 – 47 (median 38) Posttest performance scores range: 33.7 – 50.67 (median 40.7) identified the chance to review their own performance on Total scores significantly higher at posttest (M = 42.4) videotape and to have access to than pretest (M = 36.7), t (2.357), p = .025 (one-tailed) an expert instructor as the most valuable components of the training program. The lack of improvement on the written test may have been because ambulance crew members concentrated on the performance test, making little use of the self-study materials. Extended Abstract The pilot program shows promise for making high quality training, including performance skills training, available to all prehospital providers, regardless of their location. Major findings of program Gave rural EMTs access to expert instructor in another state Videotaped performance skill allowed EMTs to critique themselves Remote instructor reviewed tapes and critiqued via E-mail EMTs and instructor considered the videotaping the strongest component of the program Desktop video conference allowed remote instructor and EMTs to discuss self-study materials and written performance critiques Self-study didactic materials decreased required classroom time Self-study was not well used Students need good support system for self-study 1. Glaeser PW, Linzer J, Tunik MG, Henderson DP, Ball J. Survey of nationally registered emergency medical services providers: Pediatric education. Annals of Emergency Medicine 2000;16:33-38. 2. Seidel JS, Henderson DP, Ward P, Wayland BW, Ness B. Pediatric prehospital care in urban and rural areas. Pediatrics 1991;4:681-690. 3. Skelton MB, McSwain NE. A study of cognitive and technical skill deterioration among trained paramedics. Journal of the American College of Emergency Physicians 1977;6:436-438. 4. Latman NS, Wooley K. Knowledge and skill retention of emergency care attendants, EMT-As, and EMT-Ps. Annals of Emergency Medicine 1980;9:183-189. 5. Zautcke JL, Lee RW, Ethington NA. Paramedic skill decay. Journal of Emergency Medicine 1987;5:505-512. 6. Eichelberger MR, Stossel-Pratsch G, Mangubat EA. A pediatric emergencies training program for emergency medical services. Pediatric Emergency Care 1985;1:177-179. 7. Hobbs GD, Moshinskie JF, Roden SK, Jarvis JL. A comparison of classroom and distance learning techniques for rural EMT-I instruction. Prehospital Emergency Care 1998;2:189-191. 8. Larmon B, Schriger DL, Snelling R, Morgan MT. Results of a 4-hour endotracheal intubation class for EMT-basics. Annals of Emergency Medicine 1998;31:224-7. 9. Stewart RD, Paris PM, Pelton GH, Garretson D. Effect of varied training techniques on field endotracheal intubation success rates. Annals of Emergency Medicine 1984;13:1032-1036. Contact: Jeri Pullum Critical Illness and Trauma Foundation 2125 1st Ave. South, Great Falls MT 59401 406.761.2692 jpullum@citmt.org Contact: D. Breck Rushton Utah Bureau of EMS P.O. Box 142004 Salt Lake City, UT 84116-2004 (801) 538-6719 brushton@doh.state.ut.us