Adverse Drug Reaction ADR Form
advertisement

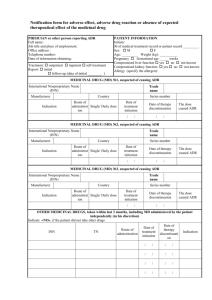
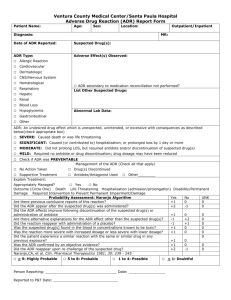
PLACE LABEL HERE ADVERSE DRUG REACTION (ADR) FORM Submission of this report does not constitute an admission that medical personnel or the product caused or contributed to the event. ADR DEFINITION- Any unexpected, unintended, undesired, or excessive response to a drug that: requires discontinuing the drug (therapeutic or diagnostic); requires changing the drug therapy; requires modifying the dose (except for minor dosage adjustments); necessitates admission to a hospital; prolongs stay in health care facility; necessitates supportive treatment; significantly complicates diagnosis; negatively affects prognosis, or results in temporary or permanent hard, disability or death. Additionally: Allergic reactions (an immunologic hypersensitivity occurring as the result of unusual sensitivity to a drug) and an idiosyncratic reactions (abnormal susceptibility to a drug that is peculiar to the individual) are considered ADRs. Suspected ADRs should also be documented and reported. - Mild ADR: no or minimal intervention required to prevent incapacity, i.e. drug held, discontinued or antidote given Moderate ADR: requires initial or prolonged hospitalization or is life threatening. Severe ADR: results in persistent incapacity or death (Notify Pharmacy in addition to Physician) PHYSICIAN NOTIFICATION: IMMEDIATE if the ADR has harmed or potentially harmed the patient. Suspected Medication(s): ____________________________ Dose___________ Route______ Time administered__________ ____________________________ Dose___________ Route______ Time administered__________ Clinical Staff Review: Patient weight ________kg Serum Creatinine level________ (date_______) Drug Allergies: NKA or ________________________________________________ Date Reaction Noted __________________ Time______________________ Reaction occurred prior to admission/visit? Yes No Admission/visit due to this ADR? Yes No Description of reaction: _________________________________________________________________________________________________ _________________________________________________________________________________________________ _________________________________________________________________________________________________ Intervention/Treatment: _________________________________________________________________________________________________ _________________________________________________________________________________________________ Resolution/Outcome: _________________________________________________________________________________________________ Name of Physician notified __________________________________ Date________Time ______ Name of Pharmacist notified _________________________________Date________ Time ______ Clinical Staff Name (print)__________________________________ Ext._______ Signature_______________________________________________ Date_______ Time________ Physician Review: Yes Based on this reaction, should patient be advised to avoid this drug in the future? Yes NEW Allergy: No No ________________________________________________________________________________________________ _________________________________________________________________________________________________ WHITE: Order section of Chart *1-16153* 1 CANARY: Pharmacy, AFTER Physician review FORM 1-16153 REV. 11/2012 Page 1 of PLACE LABEL HERE ADVERSE DRUG REACTION (ADR) FORM ______________ Date ___________________ Time WHITE: Order section of Chart *1-16153* 1 _________________________________ Physician Signature __________ PID Number CANARY: Pharmacy, AFTER Physician review FORM 1-16153 REV. 11/2012 Page 1 of