View/Open
advertisement

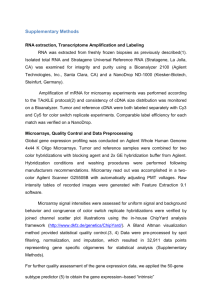
In: Tumor Markers Research Perspectives Editor: G. A. Sinise, pp. - ISBN: 978-1-60021-577-3 © 2007 Nova Science Publishers, Inc. Chapter XIV Characterization of Breast Cancer Subtypes by Immunohistochemistry in a Large Retrospective Study J. Decock 1, W. Hendrickx 1,2, C. Stefan 1, P. Neven 2, H. Wildiers 1,2, MR. Christiaens 2, A. Smeets 1,2 and R. Paridaens 1,2 * 1 Laboratory for Experimental Oncology (LEO), Department of General Medical Oncology, University Hospital Gasthuisberg, Herestraat 49, 3000 Leuven, Belgium 2 Multidisciplinary Breast Center (MBC), University Hospital Gasthuisberg, Herestraat 49, 3000 Leuven, Belgium Abstract Background: DNA microarray studies identified distinct molecular subtypes that are associated with different clinical outcome, defined as luminal A, luminal B, basal-like and Her2+ER-. This study aimed to evaluate the immunohistochemistry markers ER, PR and Her2 as surrogate markers for the previously identified molecular subtypes in a large retrospective cohort (n=1678) with invasive breast carcinomas with regard to various demographic, clinical and pathological features. Methods: All patients were diagnosed with primary breast cancer between 2000 and 2005 at the University Hospital Leuven. None of them received neo-adjuvant therapy, had bilateral cancer, tumors with direct extension to chest wall or skin, or nipple Paget’s disease. ER, PR and Her2 expression was determined by immunohistochemistry and cases with intermediary staining for Her2 were further subjected to two-color fluorescence in situ hybridization analysis. Clinical and pathological features included age at diagnosis, menopausal status, maximum tumor size, tumor grade, lymph node status and Nottingham Prognostic Index (NPI). * Corresponding author: Decock J., Laboratory for Experimental Oncology, University Hospital Gasthuisberg KULeuven, O&N1, Room 815, Herestraat 49, 3000 Leuven, Belgium. Phone: +32 (0)16.34.62.93; Fax: +32 (0)16.34.69.01; E-mail: julie.decock@med.kuleuven.be 2 J. Decock, W. Hendrickx, C. Stefan et al. Results: Of the 1678 patients with invasive breast carcinoma, 80% (n=1342) had luminal A subtype, 7% (n=119) had luminal B subtype, 9% (n=144) had basal-like type and 4% (n=73) had Her2+/ER- carcinomas. Within the luminal type, the majority of cases were PR+, with 87% and 83% for the A and B subtypes, respectively. Luminal A carcinomas were more often small in size (p=0.037), well/moderately differentiated (p<0.00001) and associated with a lower NPI value (p<0.00001). Patients with a luminal B-type tumor presented more frequently with lymph node involvement (p=0.04) and were significantly younger at diagnosis (p=0.00012) compared to the other patients. Most basal-like and Her2+/ER- carcinomas were poorly differentiated (92% and 85% respectively). Furthermore, patients with luminal A or Her2+/ER- carcinomas were more often postmenopausal than patients with a luminal B or basal-like tumor (p=0.016). Conclusions: In our large retrospective cohort of 1678 invasive breast cancers, the luminal A carcinomas were by far best represented in comparison with the other immunohistochemistry-defined (sub)types, and significantly associated with good prognostic clinical and pathological parameters. By contrast, although less represented, the luminal B, the basal-like and the Her2+ER- tumor (sub)types were more frequently associated with unfavourable prognostic factors such as younger age at diagnosis, lymph node involvement or poor histological grade. Keywords: breast cancer, subtypes, clinicopathological parameters, immunohistochemistry. Introduction Breast cancer is a heterogeneous disease consisting of several histological subtypes with different clinical outcome and with patients showing a diverse range of responses to a given treatment. Although lymph node involvement, histologic grade, tumour size, steroid hormone receptor expression and Her2 status all have been strongly correlated to prognosis, their assessment does not alter our inability to accurately predict relapse or response to therapy. A broad variety of genes and proteins has been analyzed in single-marker prognostic and predictive studies but most of them were hampered by small size, patient selection criteria, tumor heterogeneity or treatment diversity and consequentially lacked power to identify all patients at risk for recurrence and those who would benefit from a new therapy [1; 2]. A large number of genes are involved in cell growth, death and differentiation and account as such for much of the phenotypic diversity between tumors. The growing knowledge of these complex gene signal transduction pathways emphasizes the importance of studying multiple genetic alterations simultaneously and promotes the emergence of oncogenomics. A major goal in the field of oncogenomics is to try to answer the clinically important questions about which tumours will behave aggressively, which tumours will remain dormant, which patients do and do not require systemic therapy and what type of drugs should be used [3]. Analyses of thousands of genes using microarrays have classified breast carcinomas into distinct subtypes, associated with different clinical outcomes. Perou and colleagues initially classified 38 invasive breast carcinomas based on their distinct gene expression profile into four subtypes: luminal-like, basal-like, Her2+/ER- and normal breast-like [4]. Later the same research group analyzed the expression profiles of 78 breast carcinomas and categorized them into five subgroups based on variations in gene expression: luminal A, luminal B, Her2+/ER-, Breast Cancer Subtypes 3 basal-like and normal breast-like, [5]. Since then, various microarray studies confirmed the segregation of breast tumors into distinct subtypes with different clinical outcomes in various ethnic populations [6-11]. Patients with luminal A type tumors are facing a relatively good prognosis, whereas patients with basal-like tumors experience a much shorter overall and disease free survival period. Some studies also reported on the clinical and pathological characteristics of the different subtypes [6; 7; 12-16]. Furthermore, it has been shown that the various subtypes remarkably differ in their response to treatment, as reviewed by Brenton et al. [17]. Not surprisingly, hope has risen that this new classification system might improve the accuracy of prognostic stratification and lead to the development of new tumor-tailored therapeutic strategies. Although microarrays have the potential to be used as diagnostic and prognostic tools, they have not yet come into routine clinical practice due to their timeconsuming character and high cost. In this context, the usefullness of immunohistochemical surrogates for separation of the distinct subtypes should be evaluated, as indicated by the group of Carey LA [7]. They evaluated the use of immunohistochemistry (IHC) markers that were previously verified against gene expression profiles to estimate the prevalence of the intrinsic subtypes in a large population-based epidemiological study of African American and white women. They identified IHC profiles that best matched the gene expression profiles by performing both microarray analysis and IHC and validated these IHC surrogates using a 930-case tissue microarray. In this way, IHC-based definitions for the various molecular subtypes were ER+PR+/-Her2- for luminal A, ER+PR+/-Her2+ for luminal B, ER-PR-Her2+ for Her2+ subtype and ER-PR-Her2- for basal-like [5; 8; 16]. We aimed to characterize these IHC-defined subgroups on a large retrospective cohort of 1678 invasive breast cancer patients with regard to classic clinical and pathological features. Materials and Methods Patients A total of 1678 patients with primary operable breast cancer were included in this study. Patient characteristics were extracted from clinical files, tumour characteristics and lymph node status were retrieved from pathology reports, and all data were collected in our central breast cancer database. All patients were newly diagnosed at the Multidisciplinary Breast Center of the University Hospital of Leuven between 2000 and 2005, underwent mastectomy or local wide excision of their primary breast tumour and axillary lymph node dissection for staging and treatment. None of them received neo-adjuvant therapy, had bilateral cancer, tumors with direct extension to chest wall or skin, or nipple Paget’s disease. For all patients included, data are available on age at diagnosis, menopausal status, tumour size and grade, lymph node involvement, steroid hormone receptor expression and Her2 status. 4 J. Decock, W. Hendrickx, C. Stefan et al. Pathological Assessment of Tumour Tissue Tumour typing and grading were performed on paraffin embedded haematoxylin-eosin (H&E) slides according to the WHO-classification and the Ellis and Elston grading system respectively. Lymph nodes were examined with H&E using 3 sections per node. The Nottingham Prognostic Index was calculated using the equation NPI = 0.2 x tumor size (cm) + grade (I–III) + lymph node score. Immunohistochemical staining for ER, PR and Her2 was performed on 4µm thick serial paraffin sections. Heat-induced epitope retrieval was carried out in a calibrated water bath (95-99°C) and antibody complexes were visualised by Envision (Dako, Glostrup, Denmark) and DAB. A broad variety of antibodies for ER and PR has been used in the period of 2000 to 2005 and semiquantitative evaluation has been performed using the H-score for tumors resected between January 2000 and august 2003 or the Allred score system for tumors resected after august 2003. The primary mouse monoclonal antibody CB11 (Novocastra Laboratories, Newcastle-upon-Tyne, UK) directed against Her2 was applied in a dilution of 1/40 and expression was evaluated with the DAKO scoring system. Classification of Breast Cancer Subtypes Based upon ER, PR and Her2 immunohistochemical stainings, breast tumors were classified into 4 subgroups ER+PR+/-Her2-, ER+PR+/-Her2+, ER-PR-Her2- and ER-PR-Her2+, which resemble the previously identified luminal A, luminal B, basal-like and Her2+/ERsubgroups. Both the H-scoring and Allred scoring systems take in account the staining intensity and percentage of cells positively stained. A complete H-score was calculated by summing the products of the percentage positively stained cells at a given staining intensity (0–100) and the different staining intensities (0–3). The Allred score was determined by summing the score representing the proportion of positive tumour cells (0-5) with the staining intensity (0-3). For both scoring systems, ER and PR expression was considered negative when staining was completely absent. Using the H score, expression was defined positive when the final score was 1-300, while for the Allred score expression was considered positive when the final score was 2-8. The DAKO scoring system for Her2 immunostaining was applied, taking both the proportion of tumour cells with positive membrane staining and the staining intensity into account. A score of 0 or 1 was defined negative, while a score of 2 or 3 was considered positive for Her2 overexpression. Cases with a DAKO score of 2 were further analyzed by 2-color Fluorescence In situ Hybridisation (PathVysion, Vysis, Downers Grove, IL, USA) in order to distinguish true amplification from polysomie. A mean Her2/chromosome 17 ratio > 2 was considered amplified for Her2. Statistical Analyses Differences between breast cancer subtypes with regard to clinicopathological characteristics were examined using 1-way ANOVA for age at diagnosis and NPI value and Chi Square tests for the remaining variables. Statistical analyses were performed using the software package SPSS version 13, the level of significance being set at p ≤ 0,05. Breast Cancer Subtypes 5 Results Study Population The median age at diagnosis of all patients was 58 (range 26-95). The majority (1177) of the patients were postmenopausal, while 498 patients were premenopausal. Small and large tumours were equally distributed, 857 (51%) and 821 (49%) tumours respectively. A total of 231 tumours (14%) were well differentiated, 797 (47%) moderately and 650 (39%) poorly. No nodal involvement was found in 1069 (64%) patients while 609 (36%) were lymph node positive. Stratification of tumours into molecular subtype-like groups; based on ER, PR and Her2 expression; resulted in 1342 (80%) luminal A, 119 (7%) luminal B, 144 (9%) basal-like and 73 (4%) Her2+/ER- carcinomas. Within the luminal tumor type, the majority of cases were PR+, with 87% and 83% for the A and B subtypes, respectively (table 1). According to the American Joint Committee on Cancer staging system, 664 patients had stage I disease, 755 had stage II disease and 259 had stage III disease. Table 1. Distribution of immunohistochemistry- defined breast cancer subtypes according to clinical and pathological features (n=1678). variable All n all 1678 Menopausal status premenopausal 498 postmenopausal 1177 Histologic grade G1+2 1028 G3 650 Tumour size pT1 857 pT2+3 821 Axillary lymph node status negative 1069 positive 609 ERPR ER+PR+ 1272 ER+PR189 ER-PR217 Age, mean 58 NPI, mean 4,27 * luminal A %(n) luminal B %(n) basal-like %(n) p value* 9(144) Her2+/ER %(n) 4(73) 80(1342) 7(119) 28 72 39 61 37 63 26 74 0,015 72 28 31 69 8 92 15 85 <0,00001 53 47 45 55 44 56 42 58 0,037 65 35 52 48 65 35 60 40 0,044 87 13 0 59 4,1 83 17 0 54 4,85 0 0 100 56 4,97 0 0 100 57 5,02 <0,00001 0,00012 <0,00001 Associations between immunohistochemistry-defined subtypes and the continuous variables age and NPI were analyzed using one-way ANOVA, while associations with the remaining characteristics were analyzed using the Pearson Chi Square test. 6 J. Decock, W. Hendrickx, C. Stefan et al. Steroid Hormone Receptor Status of Tumor Subtypes Based on ER, PR and Her2 expression of the tumor, breast tumors can be classified into immunohistochemistry-defined subtypes. Estrogen receptor negative tumors can be subdivided into basal-like (ER-PR-Her2-) and Her2+/ER- (ER-PR-Her2+) tumors, while ER+ tumors can further be classified as luminal A (ER+PR+/-Her2-) or luminal B (ER+PR+/-Her2+). Within the luminal type, we determined the proportion of PR+ cases and found 87% and 83% of luminal A and luminal B tumors to be PR+ (table 1). Characterization of Tumor Subtypes Characteristics of the IHC-defined breast cancer subtypes are presented in table 1. Breast cancer subtypes differed significantly by age (p=0.0001), menopausal status (p=0.015), histologic grade (p< 0.00001), tumor size (p=0.037), axillary lymph node status (p= 0.044) and NPI (p< 0.00001). As the NPI value is based on tumor size, histologic grade and lymph node involvement, this result reflects the significant difference found among the various subtypes for each of these parameters. The proportion of smaller tumors (< 21 mm) was not dramatically different among the various groups, with the exception again of the luminal A group in which the tumors tended to be smaller. Luminal carcinomas and in particular luminal A-type tumors were more likely well/moderately differentiated, whereas the majority of basal-like (92%) and Her2+/ER(85%) carcinomas were poorly differentiated. Patients with a luminal B type tumor had the highest prevalence of lymph node involvement and were significantly younger than the other patients. All 4 breast tumor subtypes were associated with a NPI value indicative for a moderately good prognosis (3.4<NPI<5.4) with the lowest value observed in the luminal Atype tumors. This result for luminal A tumors is not surprisingly since the tumor size, grade and lymph node involvement in this group of tumors all indicated a good prognosis. The number of premenopausal patients was higher in the groups with luminal B and basal-like tumors compared to those with luminal A or Her2+/ER- tumors. Moreover, each of these findings was also observed in the subgroup of patients with early stage disease (stage I and II) at an even higher significance, with exception of the lymph node status (table 2). Breast Cancer Subtypes 7 Table 2. Characteristics of immunohistochemistry-defined subtypes in breast cancer patients with early stage disease (n=1419). variable all n 1419 all Menopausal status premenopausal 399 postmenopausal 1020 Histologic grade G1+2 891 G3 528 Axillary lymph node status negative 1069 positive 350 ERPR ER+PR+ 1078 ER+PR161 ER-PR180 Age, mean 59 NPI, mean 3,91 * luminal A %(n) 81(1145) luminal B %(n) 7(94) basal-like %(n) 7(123) Her2+/ER%(n) 4(57) p value* 26 74 40 60 37 63 25 75 0,002 74 26 35 65 6 94 16 84 <0,00001 76 24 66 34 76 24 77 23 0,19 87 13 0 59 3,75 82 18 0 54 4,4 0 0 100 56 4,69 0 0 100 58 4,57 <0,00001 <0,00001 <0,00001 Associations between immunohistochemistry-defined subtypes and the continuous variables age and NPI were analyzed using one-way ANOVA, while associations with the remaining characteristics were analyzed using the Pearson Chi Square test. Conclusion We examined the presence and characteristics of various immunohistochemistry-defined subtypes in a large retrospective cohort of invasive breast cancer patients by means of routine immunohistochemical staining for ER, PR and Her2. We were able to confirm the existence of four tumor subgroups, resembling the microarray identified subtypes luminal A, luminal B, basal-like and Her2+/ER-. On basis of their clinical and pathological profile, patients with luminal A tumors seem to have a good prognosis which was reflected in menopausal status, small tumor size, high proportion of well/moderately differentiated tumors and consequently a lower NPI value. In contrast, patients with luminal B tumors were more likely associated with poor prognosis as they were significantly younger than the others and were often associated with lymph node involvement. However, any conclusion regarding menopausal status rather than age in association with breast cancer phenotypes may have been biased by use of contraceptives or hormone replacement therapy. The differences in clinical prognostic features for both luminal subtypes can also in part be explained by microarray analyses which showed that luminal A type tumors have, in general, higher expression of estrogen responsive genes and lower expression of proliferative genes than luminal B [5; 8]. Just as others, we were not able to clearly characterize the ER- tumor subtypes, basal-like and Her2+/ER-, except for the observation that they were more likely poorly differentiated [5; 7; 17]. The poor prognosis of the Her2+/ER- and basal-like tumor subtypes is most probably 8 J. Decock, W. Hendrickx, C. Stefan et al. due to the fewer treatment options available for ER- and PR- tumors. Moreover, although treatment with the anti-Her2 monoclonal antibody trastuzumab in combination with chemotherapy significantly improves disease-free-survival among women with advanced breast cancer and remarkable reduces the number of patients with relapse, not all Her2+ tumors respond to trastuzumab [18]. To our knowledge, this is by far the largest retrospective cohort of invasive breast cancer patients with clinicopathological characterization of the various tumor subtypes. Although the molecular breast tumor subtypes were initially identified by microarray gene expression studies, we support Carey LA and colleagues in their hypothesis that IHC assessment of ER, PR and Her2 is a good alternative approach for analysis of the subtypes in a large retrospective cohort. Moreover, our findings are in line with the results from Calza et al. who recently reported the largest microarray study on a population-based cohort of 412 breast cancer patients [6]. They observed that luminal A carcinomas were mostly found in postmenopausal women, tended to be small and were more likely good/moderately differentiated. Furthermore, they found that in comparison with luminal A tumors, the luminal B group had a higher proportion of poorly differentiated and lymph node positive tumors. In their cohort, basal-like tumors were most often found in younger, premenopausal patients with poorly differentiated tumors, while Her2+/ER- tumors were more frequently observed in elderly women with large and poorly differentiated tumors. The strength of our study is that the cohort consisted of as well 1419 (85 %) patients with early stage (stage I, II) disease as 259 (15%) patients with advanced disease (stage III). Interestingly, analysis of early stage disease revealed the presence of the same four distinct tumor subtypes which were similarly characterized as those in the overall study population. Other groups analyzed the gene expression in DCIS for comparison with normal and invasive carcinomas in various ethnic populations and found that DCIS tumors could be similarly divided into distinct subtypes with different clinical outcomes [19-21]. All these studies imply that the molecular signatures defining the subtype of a tumor and its clinical characteristics may already be set in early stage disease and even at the pre-invasive stage of carcinogenesis. We would like to emphasize the importance of the methodology used for steroid hormone and Her2 assessment; immunohistochemical analyses have their limitations. Also, the current reproducibility and clinical relevance of microarray generated data have recently been criticized by Dupuy and Simon [22]. Both methodologies are used to measure the gene or protein expression of ER, PR and Her2 and not necessarily reflect the activity of the receptor and its downstream pathways. Moreover, immunohistochemical staining of Her2 does not allow us to distinguish between true gene amplification and polysomy and hence FISH analysis is required for cases with intermediary Her2 staining. In our institute, dual-color FISH is therefore performed as routine clinical practice for Her2 overexpressing tumors with an IHC score of 2. Expression analysis of downstream signalling pathways might enlighten the knowledge on breast cancer behaviour and improve prognostic accuracy. In conclusion, using routine immunohistochemistry we were able to confirm the presence of four subgroups, resembling the microarray identified molecular subtypes, in a large population-based cohort of breast cancer patients with early or late stage disease. Furthermore, our study supports the hypothesis that these immunohistochemistry-defined tumor subtypes are distinct biological entities with distinct clinical characteristics. Breast Cancer Subtypes 9 Acknowledgements We gratefully thank Prof. M. Drijkoningen for the pathological assessment of all tumor specimens. Further, we acknowledge all collaborators of the Multidisciplinary Breast Center, General Medical Oncology and Gynecology for their help with data input. Grant support: This work is funded by the “Vlaamse Liga tegen Kanker” and the EU Framework Programme 6 (LSHC-CT-2003-503297, Cancerdegradome). References [1] [2] [3] [4] [5] [6] [7] [8] Chatterjee, S.K. and Zetter, B.R. (2005). Cancer biomarkers: knowing the present and predicting the future. Future. Oncol., 1, 37-50. Coradini, D. and Daidone, M.G. (2004). Biomolecular prognostic factors in breast cancer. Curr. Opin. Obstet. Gynecol., 16, 49-55. Strausberg, R.L., Simpson, A.J., Old, L.J. and Riggins, G.J. (2004). Oncogenomics and the development of new cancer therapies. Nature, 429, 469-474. Perou, C.M., Sorlie, T., Eisen, M.B., van de Rijn, M., Jeffrey, S.S., Rees, C.A., Pollack, J.R., Ross, D.T., Johnsen, H., Akslen, L.A., Fluge, O., Pergamenschikov, A., Williams, C., Zhu, S.X., Lonning, P.E., Borresen-Dale, A.L., Brown, P.O. and Botstein, D. (2000). Molecular portraits of human breast tumours. Nature, 406, 747-752. Sorlie, T., Perou, C.M., Tibshirani, R., Aas, T., Geisler, S., Johnsen, H., Hastie, T., Eisen, M.B., van de Rijn, M., Jeffrey, S.S., Thorsen, T., Quist, H., Matese, J.C., Brown, P.O., Botstein, D., Eystein, L.P. and Borresen-Dale, A.L. (2001). Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. U S A, 98, 10869-10874. Calza, S., Hall, P., Auer, G., Bjohle, J., Klaar, S., Kronenwett, U., Liu, E.T., Miller, L., Ploner, A., Smeds, J., Bergh, J. and Pawitan, Y. (2006). Intrinsic molecular signature of breast cancer in a population-based cohort of 412 patients. Breast Cancer Res., 8, R34Carey, L.A., Perou, C.M., Livasy, C.A., Dressler, L.G., Cowan, D., Conway, K., Karaca, G., Troester, M.A., Tse, C.K., Edmiston, S., Deming, S.L., Geradts, J., Cheang, M.C., Nielsen, T.O., Moorman, P.G., Earp, H.S. and Millikan, R.C. (2006). Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA, 295, 2492-2502. Sorlie, T., Tibshirani, R., Parker, J., Hastie, T., Marron, J.S., Nobel, A., Deng, S., Johnsen, H., Pesich, R., Geisler, S., Demeter, J., Perou, C.M., Lonning, P.E., Brown, P.O., Borresen-Dale, A.L. and Botstein, D. (2003). Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc. Natl. Acad. Sci. U S A, 100, 8418-8423. 10 [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] [20] J. Decock, W. Hendrickx, C. Stefan et al. Sorlie, T., Wang, Y., Xiao, C., Johnsen, H., Naume, B., Samaha, R.R. and BorresenDale, A.L. (2006). Distinct molecular mechanisms underlying clinically relevant subtypes of breast cancer: gene expression analyses across three different platforms. BMC. Genomics, 7, 127 Sotiriou, C., Neo, S.Y., McShane, L.M., Korn, E.L., Long, P.M., Jazaeri, A., Martiat, P., Fox, S.B., Harris, A.L. and Liu, E.T. (2003). Breast cancer classification and prognosis based on gene expression profiles from a population-based study. Proc. Natl. Acad. Sci. U S A, 100, 10393-10398. West, M., Blanchette, C., Dressman, H., Huang, E., Ishida, S., Spang, R., Zuzan, H., Olson, J.A., Jr., Marks, J.R. and Nevins, J.R. (2001). Predicting the clinical status of human breast cancer by using gene expression profiles. Proc. Natl. Acad. Sci. U S A, 98, 11462-11467. Abd El-Rehim, D.M., Pinder, S.E., Paish, C.E., Bell, J., Blamey, R.W., Robertson, J.F., Nicholson, R.I. and Ellis, I.O. (2004). Expression of luminal and basal cytokeratins in human breast carcinoma. J. Pathol., 203, 661-671. Jacquemier, J., Ginestier, C., Rougemont, J., Bardou, V.J., Charafe-Jauffret, E., Geneix, J., Adelaide, J., Koki, A., Houvenaeghel, G., Hassoun, J., Maraninchi, D., Viens, P., Birnbaum, D. and Bertucci, F. (2005). Protein expression profiling identifies subclasses of breast cancer and predicts prognosis. Cancer Res., 65, 767-779. Kusinska, R., Potemski, P., Jesionek-Kupnicka, D. and Kordek, R. (2005). Immunohistochemical identification of basal-type cytokeratins in invasive ductal breast carcinoma--relation with grade, stage, estrogen receptor and HER2. Pol. J. Pathol., 56, 107-110. Livasy, C.A., Karaca, G., Nanda, R., Tretiakova, M.S., Olopade, O.I., Moore, D.T. and Perou, C.M. (2006). Phenotypic evaluation of the basal-like subtype of invasive breast carcinoma. Mod. Pathol., 19, 264-271. Nielsen, T.O., Hsu, F.D., Jensen, K., Cheang, M., Karaca, G., Hu, Z., HernandezBoussard, T., Livasy, C., Cowan, D., Dressler, L., Akslen, L.A., Ragaz, J., Gown, A.M., Gilks, C.B., van de, R.M. and Perou, C.M. (2004). Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin. Cancer Res., 10, 5367-5374. Brenton, J.D., Carey, L.A., Ahmed, A.A. and Caldas, C. (2005). Molecular classification and molecular forecasting of breast cancer: ready for clinical application? J. Clin. Oncol., 23, 7350-7360. Nahta, R., Yu, D., Hung, M.C., Hortobagyi, G.N. and Esteva, F.J. (2006). Mechanisms of Disease: understanding resistance to HER2-targeted therapy in human breast cancer. Nat. Clin. Pract. Oncol., 3, 269-280. Bryan, B.B., Schnitt, S.J. and Collins, L.C. (2006). Ductal carcinoma in situ with basallike phenotype: a possible precursor to invasive basal-like breast cancer. Mod. Pathol., 19, 617-621. Kepple, J., Henry-Tillman, R.S., Klimberg, V.S., Layeeque, R., Siegel, E., Westbrook, K. and Korourian, S. (2006). The receptor expression pattern in ductal carcinoma in situ predicts recurrence. Am. J. Surg., 192, 68-71. Breast Cancer Subtypes 11 [21] Yu, K., Lee, C.H., Tan, P.H. and Tan, P. (2004). Conservation of breast cancer molecular subtypes and transcriptional patterns of tumor progression across distinct ethnic populations. Clin. Cancer Res., 10, 5508-5517. [22] Dupuy A. and Simon RM. (2007). Critical review of published microarray studies for cancer outcome and guidelines on statistical analysis and reporting. J. Natl. Cancer Inst., 99, 147-57.