Asthma Action Plan (English) - Oakland Unified School District
advertisement
 - Oakland Unified School District")
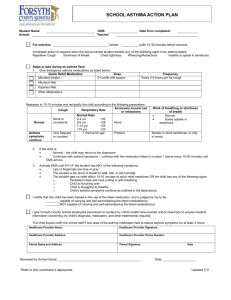
Asthma Action Plan Student Name School Parent/Guardian Name Emergency Contact Name Healthcare Provider Name Date of Birth School Phone Parent/Guardian Phone Emergency Contact Phone Health care Provider Phone ID # Attention Parent/Guardian/School Personnel: ANY student with asthma (any severity) can have a SEVERE asthma attack. Asthma is triggered by· Exercise Cold Air Animal Dander Strong Odors Grass/Pollen Colds/Flu Mold Other Controller Medicines at home How Much to Take How Often time(s) per day EVERY DAY! Other instructions Gargle or rinse mouth after use If student does not have any medication at school, notify parent immediately. Call 911 if symptoms persist longer than 10 minutes. SPECIAL INSTRUCTIONS: WHEN I AM doing well, getting worse, having a medical alert I Feel Good (Green Zone) PREVENT asthma symptoms every day: Breathing is good, and No cough, wheeze, chest tightness, or shortness of breath During the day or night, and Can work or play as normal. Peak Flow (for age 5 and up): _ _____ to _(80% - 100% of personal best) Take my controller medicines (above) every day at home as prescribed Before exercise, take _ ____puff(s) of __ with spacer (if available) 10 minutes before exercise ____ Personal Best Peak Flow is _____________ I Don’t Feel Good (Yellow Zone) Cough, wheeze, chest tightness, or shortness of breath, or can do some, but not all usual activities. Waking at night due to asthma symptoms. CAUTION, continue taking every day controller medicines at home, AND: Begin QUICK RELIEF medication right NOW Take _ ____ puffs of ___ (if available). _____ with spacer Wait 15 – 20 minutes. If symptoms are not better, repeat the above dose and wait another 15 minutes. Watch for Red Zone symptoms. Peak Flow (for age 5 and up): _ _____ to _ ___(50% - 79% of personal best) If symptoms return to GREEN ZONE wait for 15 minutes. If symptoms remain in the Green Zone, return to class and continue using quick relief medicine _ puffs every _ __ hours as needed. If NOT back in the Green Zone after the second dose of medicine, GO TO THE RED ZONE Medical Alert (Red Zone) EMERGENCY! Get help! Do not leave student alone! Severe chest tightness, or Very short of breath or uncontrolled cough, or Nose opens wide or ribs show with breath, or Quick relief medicine has not helped, or Trouble talking or walking, or Blue lips or fingernails, or drowsy or confused Peak Flow (for age 5 and up) under _ Take 4 or 6 puff of _____ spacer (if available). ________________ with Repeat every 10 – 15 minutes until paramedics arrive. Call 911 immediately and call Parent/Guardian _50% of personal best) Health Care Provider: My signature provides authorization for the above written order. I understand that all procedures will be implemented in accordance with state laws and regulations. Student carry and self-administer asthma medications: Yes No Print Provider Name/Credentials: _________________________Signature ____________________Date ________ This authorization is valid for one year from signature date. Parent Request and Authorization: I request that the school assist my child with the above asthma medication(s) and the Asthma Action Plan as ordered by the health care provider in accordance with state laws and regulations. I understand that the medication must have a pharmacy label with the name of the student and the health care provider. I give permission for the school nurse to communicate with the healthcare provider on matters related to this Asthma Action Plan. My child may carry and self-administer asthma medications: Yes No Print Parent Name: ___________________Signature _________________________Date _________ Adapted with permission from Regional Asthma Management and Prevention (RAMP), a program of the Public Health Institute, for use by Oakland Unified School District, Health Services School Nurse: ____________________________________________________ Signature ___________________________________________ Date __________________ Health Services: 746 Grand Ave. Oakland, CA 94610 • (510) 273-1510 • (510) 273-1511 fax Revised: July 2012