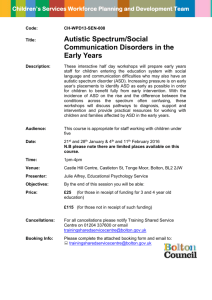
Open Access version via Utrecht University Repository
advertisement

CNV: ASD and SCZ Running head: CNVS IN AUTISM AND SCHIZOPHRENIA Rare Copy Number Variants Shared in Autism and Schizophrenia* Coppes, L. *Masters Thesis, Universiteit Utrecht, Utrecht, The Netherlands 1 CNV: ASD and SCZ 2 Abstract: Recently the large scale gathering of copy number variant (CNV) data from patients with schizophrenia (SCZ) and autism (ASD) has yielded new genetic data through which we can examine these disorders. One of the repercussions has been a suggested similarity between autism and schizophrenia, in that they may share some genetic aetiology (Corvin, 2010). While some CNVs have been shown to overlap between ASD and SCZ (Toro et al., 2010), many rare CNVs have been discarded due to low sample numbers. In this study we provide a comprehensive overview of all CNVs associated with ASD and SCZ, including rare CNVs and examine the genes found in the CNVs. Ultimately I provide an extensive overlap of the genes found in CNVs detected in ASD and SCZ. Furthermore, we present some trends in our data by examining the gene ontology and expression of the overlapped CNVs. Using a literature search in PubMed, recently published CNV data was accumulated from 2008 onwards for ASD and SCZ, including rare CNVs previously ignored. This yielded a list of 939 and 852 genes for ASD and SCZ respectively, of which 130 were shared. While the trends in the data are difficult to pin point, some suggested shared molecular functions, processes and cellular components are provided with supporting background literature. These include, but are not limited to, a discussion of neurodevelopment and cell adhesion processes. What this study illustrates is a potentially shared genetic aetiology between ASD and SCZ. This converges with a broader hypothesis suggesting that many psychiatric disorders share genetic variants which lay a framework for later psychiatric dysfunction (Craddock & Owen, 2010). This study also provides new genetic data to examine the relationship between ASD and SCZ. Keywords: autism, schizophrenia, copy number variant, cell adhesion molecule, GABA receptor, acetylcholine receptor, cell junction, genetics, genetic variants, genetic aetiology CNV: ASD and SCZ 3 Introduction: Psychiatric disorders have been, and continue to be separated by symptomatic differences, as significant behavioural differences exist between psychiatric disorders. Autism spectrum disorders (ASD) has been characterised by behaviours such as impairments in social interaction and the expression of repetitive behaviours. This is in contrast with schizophrenia (SCZ) which has been characterised by two sets of symptoms, both positive and negative. Positive symptoms include hallucinations and delusions, whereas negative symptoms involve a lack of motivation and emotion. The influence of genetics is unquestionable in both disorders as ASD has a heritability estimate of 90% (Bailey et al., 1995) and SCZ has a heritability estimate of 80% (Sullivan, Kendler, & Neale, 2003). While it seems that these two psychiatric diseases diverge, due to the different symptoms, new data suggests that they may be more similar than perceived as a number of specific copy number variants (CNVs) are shared between ASD and SCZ patients (Corvin, 2010). It should also be noted that the similarities between ASD and SCZ is not a novel idea, as Kanner initially suggested that ASD was a subtype of SCZ (Kanner, 1943), although we later went on to think of ASD and SCZ as independent and unrelated (Rutter, 1975). The idea that ASD and SCZ share some commonality is re-emerging as it seems that ASD and SCZ share a number of genetic variants (Corvin, 2010), and consequently neurobiological pathways. These variants are not exclusively shared by ASD and SCZ, as it seems that these variants are also involved in the progression of many other psychiatric disorders, including bi-polar disease, epilepsy, attention-deficit/hyperactivity disorder (ADHD) and intellectual disability. This has lead to the suggestion that there is an underlying genetic similarity between different psychiatric disorders, which lays a groundwork for neurological dysfunction (Craddock & Owen, 2010). The groundwork essentially predisposes one to an increased likelihood of psychiatric disorder, whereas environmental influence, and likely other genetic variants and mutations, play a role in guiding one to a specific psychiatric disorder. This breakthrough in psychiatric research is in part due to CNV: ASD and SCZ 4 large sample screens for rare copy number variants (CNV), the genetic culprits of interest in this paper. CNVs are portions of DNA with copy-number differences when comparing multiple genomes (Feuk, Carson, & Sherer, 2008). These structural variants may infringe on a gene through its coding region, promoter region or any region essential to genetic expression. The disruption manifests itself as a dosage-dependant gain or loss of function due to deletions or duplications of the copy-numbers (Toro et al., 2010), and when certain critical genes are altered the potential for grave neuropsychiatric disorders increases. Another type of genetic alteration that has been examined are single nucleotide polymorphisms (SNP). While there is unquestionable utility in examining and understanding SNPs, it would seem that utilizing CNVs is certainly as important. First of all, CNVs are reported to have a larger nucleotide content than CNVs, suggesting a large wealth of genetic data and potential influence over phenotypes (Pang et al., 2010; Redon et al., 2006, Stranger et al., 2007). Secondly, SNPs provide only a locus of interest within a gene, sometimes appearing outside of the protein coding region and having little downstream effect. On the other hand CNVs mark a causal gene by interrupting or duplicating it potentially affecting gene expression or gene dosage (Shelling & Ferguson, 2006). While SNPs have provided critical information to understand psychiatric disease, it would seem that examining CNVs is required to develop a more complete framework. Recently large samples have been screened for CNVs in both SCZ (Stefansson et al., 2008; 2009) and ASD (Pinto et al., 2010). These studies, along with their predecessors, have provided some integral insight into the genetics of these disorders. While a number of significant genetic candidates are elucidated, some challenges must be faced to address the breadth of genetic variants observed in SCZ and ASD. This includes the rarity of certain genetic abnormalities, as a number of genetic variants are found in extremely limited number of patients, often even a single patient referred to as a private mutation (Stefansson et al., 2008). This has caused some rare CNVs to remain outside of previous analyses, CNVs that may be harbouring prime genetic culprits for SCZ and/or ASD. Another issue is addressing a lack of replicable data, to reliably illustrate the CNV: ASD and SCZ 5 implication of a rare CNV and the manifestation of the psychiatric disorder in question. Although progress is being made as some deletions have been replicated for ASD (Kumar et al., 2008; Marshall et al., 2008; Weiss et al., 2008; Mefford et al., 2009) and SCZ (International Schizophrenia Consortium, 2008; Stefansson et al., 2008; Wilson et al., 2006; Vrijenhoek et al., 2008; Xu et al., 2008). Finally, and perhaps most important for this paper, is the overlap of similar genetic abnormalities in different psychiatric diseases that have emerged from these studies. Genetic variants that breach a specific psychiatric disorder and show significant associations in multiple neurodevelopment disorders have lead to the suggestion that these disorders may share a common genetic aetiology, at least in part. For example, Corvin (2010) examined a number of genome-wide association studies (GWAS) for genetic alterations found in bipolar disease, SCZ and ASD. They found that cell adhesion molecules (CAM), such as CNTNAP2 and NRXN1 are often disrupted in all three of these patient groups. They go on to suggest that CAMs likely underlie morphological abnormalities present in psychiatric disorders by altering neurodevelopment, a suggested function of CAMs. Toro et al. (2010) found similar results examining genetic variants associated to ASD and SCZ, among other disorders. CAMs like NRXN1 and CNTNAP2 showed a higher CNV burden in SCZ and ASD. CAMs seem to play a significant role in SCZ and ASD, as their appearance seems scattered amongst much CNV research. Two CAMs likely implicated in brain development and synapse formation are of particular interest, NRXN1 and CNTNAP2. NRXN1 has been associated with ASD (Wiśniowiecka-Kowalnik et al., 2010; Bucan et al., 2009; Glessner et al., 2009; Kumar & Christian, 2009; Marshal et al., 2008; Kim et al., 2008) and SCZ (Rujescu et al., 2009; Kirov et al., 2009; Corvin, 2010); CNTNAP2 has also been associated with ASD (Burbach & van der Zwaag, 2009; Kumar & Christian, 2009) and SCZ (Burbach & van der Zwaag, 2009; Friendman et al., 2010 ). Moreover NRXN1 has been associated with ADHD (Bradley et al., 2010) and intellectual disability (Ching et al., 2010), and CNTNAP2 has been associated with bipolar disease (Wang, Lui & Aragam, 2010). These genetic similarities point to the potential for shared aetiology between not only ASD and SCZ, but a plethora of psychiatric disorders, CNV: ASD and SCZ 6 potentially through the pathways in which CAMs such as NRXN1 and CNTNAP2 are players. However it would seem that this is just the tip of the iceberg, as many rare CNVs, such as private mutations, have yet to be examined across psychiatric disorders. This issue was mentioned earlier in the introduction, and as such all CNVs, including private CNVs, will be included in this paper. Moreover, few comparisons of CNV data for SCZ and ASD have been done to date. While it seems certain that SCZ and ASD do share some genetic variants, such as NRXN1 or CNTNAP2 (Corvin, 2010), a deeper examination of this overlap is crucial to understanding the relationship between SCZ and ASD. Finally, SCZ and ASD are not exclusively related, as the shared variants include psychiatric disorders like bipolar disease, epilepsy and ADHD. This has lead to a proposed model by Craddock and Owen (2010) suggesting that psychiatric disorders share genetic variants that lay a foundation for psychiatric dysfunction. While the relationship between SCZ and ASD remains unclear, what seems to be emerging is shared genetic infringements by CNVs are causing us to reconsider the relationship between SCZ, ASD and many other psychiatric disorders. Newly published literature has started illustrating how ASD, SCZ and other psychiatric disorders share specific genetic variants. However, this genetic overlap remains mostly undefined, partially due the large number of rare CNVs, or private mutations, discussed in the introduction. As such, our goal is to examine the entire breadth of shared CNVs in SCZ and ASD, specifically elucidating rare genetic variants shared in ASD and SCZ. We also clustered the affected genes in terms of genetic ontology and examined the expression analysis across different brain regions and over time. This would allow us to not only present a list of shared genetic variants between SCZ and ASD, but hopefully characterise the shared variants based on molecular function, biological process, cellular component and expression patterns. While the relationship between ASD and SCZ will not be characterised based on the results, we hope to provide a comprehensive overview of genetic variants to be examined more CNV: ASD and SCZ 7 closely within ASD and SCZ, elucidating a wealth of genetic abnormalities upon which the overlap between SCZ and ASD can be furthered and understood. Methods: Procedure 1) Assembly of gene lists: A search using PubMed was applied to acquire recently published large scale CNV data for ASD and SCZ. No special consideration was given when selecting published CNV data other than utilising the most recent data, published from 2008 until now. Using the publically available supplementary materials provided from the selected papers, an overview of genes found in CNVs was created for both SCZ and ASD independently. All disease selective genetic variants were included in our assembly to assure that a comprehensive overview was compiled. Therefore, some CNVs may be rare and found in only one individual, while other CNVs are found significantly more often in cases rather than controls. Also the resulting gain or loss of function due to the CNVs was not taken into account, as any altered gene expression was considered. The two compiled data sets were superposed and the genes were examined for the presence of CNVs in both populations. 2) Gene ontology analysis: A further analysis of gene ontology was also pursued. The genes found in CNVs in both ASD and SCZ were clustered based on molecular function, cellular component and biological process using the protein analysis through evolutionary relationships (PANTHER) classification system gene expression analysis tool (pantherdb.org, 2010). It allowed us to examine if there were functions, processes or cellular components that were significantly overrepresented in our list of shared CNVs. This was done using the list of shared CNVs between SCZ and ASD and comparing it too a reference list of the homo-sapiens genome provided by PANTHER (pantherdb.org, 2010). Based on the reference list and the total number of genes in the shared list, an estimate of the expected CNV: ASD and SCZ 8 genes for each molecular function, biological process or cellular component in the matched list was calculated. The actual number of genes found for each molecular function, biological process and cellular component were compared to the estimate to determine the significance of over/under representation. A detailed methodology explaining the bioinformatic algorithms involved can be found in Thomas et al. (2003) and Mi et al. (2005). To provide more meaningful results general groupings such as “binding” were ignored to highlight more specific groupings such as “protein or nucleic acid binding.” This was achieved by removing grouping terms with more than 5000 genes from the reference list associated with it. 3) Expression Analysis: Finally the lists were also sent for an expression analysis by Sigrid Swagemakers and Peter van der Spek at Erasmus UMC Rotterdam with data from Gene Logic Inc. (Gaithersburg, MD). An analysis was done for shared CNVs between SCZ and ASD, all CNVs for both SCZ and ASD individually, and non-shared CNV for both SCZ and ASD individually. Heat maps were created representing higher and lower than average expression, with red and blue coloring respectively. The expression analysis was done across different ages and different brain regions. Data Sources While no special consideration was given to selecting published CNV data other then how recently it was published, a list of the selected studies is provided: Autism: Pinto et al. (2010); van der Zwaag et al. (2009); Christian et al. (2008) Schizophrenia: Magri et al. (2010); Kirov et al. (2009); Lee et al. (2010); Xu et al. (2009); Crespi, Stead, & Elliot (2010); Tam et al. (2010); Glessner et al. (2010); Stefansson et al. (2009). It should be noted that some of the CNV data was acquired by different procedures, based on the methodology provided by the original authors of the data. While aware of the potential problematic impact, no correction for this was pursued in this research as the procedures used across the research remain fairly arbitrary from one research group to another. We hope only to compare previously presented CNV data that is selective to CNV: ASD and SCZ 9 ASD and SCZ, acquired and analyzed according to the paper from which the data was drawn. Results: A list of CNVs was made for SCZ and ASD, with a total of 852 and 939 genes in each list respectively. These lists were compared to identify the CNVs present in both SCZ and ASD populations. There were 130 CNVs that appeared both in SCZ and ASD (see Table 1). Therefore of the 852 CNVs found in SCZ, 15.3% showed overlap with ASD, and of the 939 CNVs found in ASD, 13.8% showed overlap with SCZ. This suggests that there are similar CNVs in SCZ and ASD. Table 1. CNVs Shared in Schizophrenia and Autism Pinto et al. (2010) “known” ASD genes Pinto et al. (2010) “candidate” ASD genes Pinto et al. (2010) rare CNVs, Tam et al. (2010) ANKRD12 Glessner et al. (2010) International Schizophrenia Consortium (2008) PARK2 NUDT3, GPC6 EHHADH, ATP2C2, GPC6 PRIM2A, FAM19A2 Crespi et al. (2010) TBX1 SHANK3, TBX1 PRKAG2 GPR89A GRM7, ERBB4, MLL3 UBE2L3 van der Christian et al. Zwaag et al. (2008) AGRE (2009) ASD abnormalities susceptibility genes MKRN3 RAB23, PRIM2A LARGE SNAP29, SERPIND1 RTN4R, COMT, SEPT5 DGCR14, GSCL, C25A1, HIRA, CLTCL1, MRPL40, CDC45L, SEPT5, CLDN5, TBX1, GP1BB, GNB1L, C22orf29, COMT, XNRD2, ARCF, C22orf25, HTF9C, RANBP1 , ZDHHC8, TN4R, DGCR6L, SCARF2, NF74, KLHL22, PCQAP , RPM1, KLF13 RTNR4, SHANK3, COMT, TRPM1, KLF13, KCTD13, SEZ6L2, TAOK2, CDC95, CNV: ASD and SCZ SEPT5 Xu et al. (2009) Lee et al. (2010) Kirov et al. (2009) Magri et al. (2010) UBE3A, TBX1 NRXN1 PARK2, CNTN4 C4orf45 CSMD1 PRKAG2 RXRA TPPP, FHIT, GABRB3, GABRA5 TBC1D5, CAMK1D, ABCA13, DSC3 ZC3HAV1, TTC26, MPV17L, C16orf45, DSG3 NKD2, VIPR2, GSC2, SNAP29, SERPIND1, RTN4R, COMT, SEPT5 B3GAT1 NIPA1, CYFIP1, NRXN1, NIPA2 10 DOC2A, FAM57B, ALDOA, PPP4C, TBX6 YPEL3, MAPK3, GDPD3, DGCR14, PMP22, GSCL SLC25A1, CLTC1 , HIRA, UFD1, MRPL40, CLDN5, CDC45L, SEPT5, TBX1, GNB1L,c22orf29,COMT TXNRD2,ARVCF, DGCR8, c22orf25, RANBP1, HTF9C, RTNR4, ZDHHC8 DGCR6L CNTN4 OPTN, MCM10, C10orf49, PHYH, SEPHS1, CDRT15 HS3ST3B1, PMP22, FLJ45831, TEKT3, DGCR2, TSSK2, DGCR14, SLC25A1, MRPL40, CDC45L, UFD1L, SEPT5 CLDN5, TBX1, GP1BB GNB1L, C22orf29, COMT, TXNRD2, ARVCF, DGCR8, c22orf25, RANBP1, HTF9C, RTNR4, ZDHHC8, DGCR6L, ZNF74, SCARF2, KLHL22, ALG10, MAGEL2, MKRN3, C15orf2, NDN, SNURF, SNRPN, ATP10A, UBE3A, GABRB3, GABRA5, GABRG3, KLF13, TRPM1 NIPA2, KLF13, RPM1, TUBGCP5, CYFIP1, C16orf45 In order to characterise the genes that emerged from the list of shared CNVs in SCZ and ASD, the genes were further analysed for gene ontology, specifically molecular function (see figure 1), biological process (see figure 2) and cellular component (see figure 3). To focus on the most significant biological processes, molecular functions and cellular components, only significantly represented clusters (p<0.05), are presented in this paper. CNV: ASD and SCZ 11 For molecular function this included 10 different processes which involved 60 genes, of which some genes were duplicates involved in multiple processes. For molecular function this included 21 different functions which involved 247 genes, of which many genes were duplicates. Finally, cellular component included 3 different components which involved only 13 genes, of which some genes were duplicates. These duplicates occur because genes participate in multiple functions, processes and across various cellular components within the body. For an overview of the genes associated with each molecular function, biological process and cellular component see the supplementary materials provided (see supplementary 1-3). Figure 1. Molecular Function clustering Acetylcholine receptor activity GABA receptor activity Cytoskeleton protein binding Transferase activity Lipid transporter activity Ligand-gated ion channel activity Methyltransferase activity Receptor activity Calcium ion binding This illustrates the different molecular functions that were associated with the CNVs shared by ASD and SCZ. CNV: ASD and SCZ 12 Figure 2. Biological Process clustering developmental process oxygen and reactive oxygen species metabolic process anion transport mesoderm development cell adhesion protein metabolic process skeletal system development neurological system process meiosis cell cycle cellular calcium ion homeostasis cell-cell adhesion system process homeostatic process lipid metabolic process cellular component morphogenesis anatomical structure morphogenesis synaptic transmission cell communication lipid transport This illustrates the different biological processes that were associated with the CNVs shared by ASD and SCZ. Figure 3. Cellular Component clustering Cell junction Plasma membrane Microtubule This illustrates the different cellular components that were associated with the CNVs shared by ASD and SCZ. CNV: ASD and SCZ 13 In order to provide some overview of significance, this data is also presented in decreasing order of significance for each gene ontology clustering. This was done for biological process (see table 2), however only the top 10 processes are shown as 21 processes showed significance (p<0.05), and thus a cut off was made to make the data more presentable. All 21 biological processes can be seen in figure 2 or supplementary material 2. This data was also presented for molecular function (see table 3) and cellular component (see table 4). For a comprehensive list of the genes associated with each molecular function, biological process and cellular component see the supplementary materials (supplementary 1-3). Some notable biological processes include the developmental process, cell adhesion and neurological system processes. Some notable functions include receptor activity, specifically acetylcholineterase receptor activity and GABA receptor activity, and transferase activity, specifically methytransferase. Finally, the only cellular components in the matched list were cell junctions, microtubules and plasma membranes. This suggests that there are groups of CNVs with a heavy burden in ASD and SCZ, unfortunately the amount of significant data makes it very difficult to point out only a few culprits. Table 2. CNV disrupted genes shared by Autism and Schizophrenia, clustered by Biological Process. Biological Process # of genes # of genes in Reference in ASD & SCZ match list Developmental 3001 28 process Oxygen and 63 3 reactive oxygen species metabolic process Anion 150 4 transport Mesoderm 1528 16 development Cell adhesion 1333 14 Protein 3240 27 metabolic Expected # of genes Increase (+) or Decrease (-) Significance (P value) 16.58 + 0.00314 0.35 + 0.00531 0.83 + 0.00989 8.44 + 0.00990 7.36 17.90 + + 0.0153 0.0166 CNV: ASD and SCZ process Skeletal system development Neurological system process Meiosis Cell cycle 490 7 2.71 + 0.0193 1954 18 10.80 + 0.0212 192 1840 4 17 1.06 10.17 + + 0.0223 0.0244 14 Table 3. CNV disrupted genes shared by Autism and Schizophrenia, clustered by Molecular Function. Molecular Function # of genes in Reference Expected # of genes Increase (+) Significance or Decrease (P value) (-) 47 # of genes in ASD & SCZ match list 3 Acetylcholine receptor activity GABA receptor activity Cytoskeleton protein binding Transferase activity Lipid transporter activity Ligand-gated ion channel activity Methyltransferase activity Receptor activity Calcium ion binding Ligase activity 0.26 + 0.00235 47 3 0.26 + 0.00235 396 7 2.19 + 0.00334 1593 16 8.80 + 0.0143 92 3 0.51 + 0.0148 112 3 0.62 + 0.0246 132 3 0.73 + 0.0373 1808 454 16 6 9.99 2.51 + + 0.0403 0.0406 613 7 3.39 + 0.0540 Table 4. CNV disrupted genes shared by Autism and Schizophrenia, clustered by Cellular Component. Cellular Component # of genes in Reference Cell junction 121 Plasma 131 membrane # of genes in ASD & SCZ match list 4 4 Expected # of genes 0.67 0.72 Increase (+) or Decrease (-) + + Significance (P value) 0.00472 0.00622 CNV: ASD and SCZ Microtubule Intracellular 348 1192 5 11 1.92 6.59 + + 15 0.0444 0.0656 The CNVs shared by both SCZ and ASD were further analysed for expression in various regions of the human brain (see figure 4) and during various stages of development (see figure 5), with a complete overview provided in the supplementary materials (see supplementary 4). Figure 4: The expression of CNVs shared by autism and schizophrenia across various brain regions CNV: ASD and SCZ 16 Figure 5: The expression of CNVs shared by autism and schizophrenia from 0.1 to 83 years of age Globally what was observed is that both SCZ and ASD have many genes with higher than average expression when individuals are 2 years or younger. However, SCZ has far more genes with higher than average expression when individuals are older, over 65 years of age. In the list of matched CNV disrupted genes between SCZ and ASD we see predominantly higher than average expression during early development. This points to developmentally early shared genetic dysfunction in ASD and SCZ, suggesting that these genes may lay the groundwork for later psychiatric dysfunction in life. As an overwhelming amount of data was provided the results are referred to in the discussion for specific CNV disrupted genes of interest. The expression data results referred to in the discussion include the early expression patterns of genes with receptor activity, such as GABRB3, GABRA5 and GABRG3; genes responsible for cell adhesion, such as NRXN1, SEZ6L2, DSC3, SCARF2, DSG3, RTN4R, CSMD1, ERBB4 and CNV: ASD and SCZ 17 CNTN4; and finally genes expressed in cell junctions, such as CLDN5 and ARVCF. The details of this expression data will be presented in the discussion for these individual genes, in an attempt to characterise some of the gene ontology clusters. Discussion: The aim of the paper was to examine the overlap of CNVs between ASD and SCZ, specifically attempting to provide a broad overview of all the genes found in CNVs detected between ASD and SCZ, including rare CNVs. As hypothesized there were many CNVs shared by SCZ and ASD alluding to a shared genetic aetiology. This is not the first example of shared genetic dysfunction in ASD and SCZ, as a number of studies have indicated significant overlap in NRXN1, CNTNAP2 and other cell adhesion molecules (Corvin et al. 2010; Toro et al. 2010). Moreover, as mentioned in the introduction, the genetic overlap between psychiatric disorders doesn’t include only ASD and SCZ, but extends to include disorders such as epilepsy, bipolar, ADHD and intellectual disability (Craddock & Owen, 2010). We also examined the clustering of genes based on genetic ontology to preliminarily characterise the genes found in CNVs shared between SCZ and ASD. However, the amount of significant data acquired makes it difficult to point out specific culprits as having a larger effect on ASD and SCZ development. The same can certainly be said for expression analysis, as a detailed conclusion seems impossible given the amount of data. Having said this, including previously published data may allow us to examine certain clusters and expression patterns that might critical to the development of ASD and SCZ, such as CAMs and early neurodevelopment. As indicated the results illustrate genetic commonality in two disorders that show high levels of genetic influence and heritability. Along with the expression analysis, illustrating that many shared CNVs between SCZ and ASD have higher than average expression during early development, a suggestion could be made. It could be that genes that normally show higher than average expression during early development and are found in CNVs detected SCZ and ASD, are laying a neural groundwork leading to a high CNV: ASD and SCZ 18 susceptibility for psychiatric disorders. It is through this early dysfunction that ASD and SCZ are related, and perhaps also related to a plethora of other psychiatric disorders. While no single CNV can be suggested as a prime culprit, this study does suggest that CNVs may burden early neurodevelopment and lay the groundwork for psychiatric dysfunction. What emerges is that two disorders presently examined, diagnosed and treated differently might actually be progressing through shared neurobiological pathways. While clustering the genes seems to provide little conclusive evidence, due to the amount of data, we can examine some convergence with previous literature in an attempt to comment on what processes, functions and components might be dysfunctional in ASD and SCZ. Beginning with molecular function, some interesting comments can certainly be made. We see that genes associated with receptor activity have a high CNV burden in ASD and SCZ, specifically GABA and acetylcholine receptors. The genes for GABA and acetylcholine receptor activity were GABRG3, GABRB3, GABRA5 all of which show significantly higher expression in early development when introducing the details of our expression results. The most notable may be GABARA5 with significantly higher than average expression before 2 years of age. GABA receptors have previously been discussed in SCZ, and in fact GABAergic treatment is also being investigated very closely (Coyle et al., 2010). Moreover, Wassef, Baker & Kochan (2003) illustrated abnormalities in GABA receptors in a SCZ population, and along with the significance of GABA receptor activity in our results may point towards the GABA receptor as a culprit in SCZ progression. GABA is also present in ASD research, as reduced GABA(A) receptors were found posterior cingulate cortex and fusiform gyrus in ASD (Oblak, Gibbs, & Blatt, 2010). In our results we also see that acetylcholine receptor activity is highly burdened by CNVs in SCZ and ASD. In previous literature, a decrease in nicotinic receptors were found in the cerebral cortex of patients with ASD (Lee et al., 2002; Ray et al., 2005) and in SCZ lowered levels alpha7 nicotinic acetylcholine receptor have been found (Perl et al., 2003). Moreover both ASD and SCZ research is examining treatments targeting acetylcholine receptors (Lipiello, 2006; Hajos & Rogers, 2010). It would seem that examining genes found in CNVs with GABA and acetylcholine receptor CNV: ASD and SCZ 19 functionality may provide a new means to understanding the dysfunction in GABA and acetylcholine receptors seen in ASD and SCZ. Moreover, the significantly high expression in early development suggests that these genes may be worth examining as potential culprits that might lay the groundwork for psychiatric disorders such as SCZ and ASD. The same examination was done for biological process clustering. The most interesting process was cell adhesion, as it plays a central role in neurodevelopment. This specifically includes cell-cell adhesion, whose dysfunction has previously been considered as a shared culprit between ASD and SCZ (Toro et al., 2010). The genes found in CNVs that were included in our list were NRXN1, SEZ6L2, DSC3, SCARF2, DSG3, RTN4R, CSMD1, ERBB4 and CNTN4. It is also interesting that all of these genes show significantly higher than average expression in early development, most only up to 2 or 3 years of age, when introducing the details of our expression results. However, RTN4R and NRXN1 show moments of higher than average expression into adolescence, up to 18 years of age. As these genes show higher than average early expression they may be involved in laying the groundwork for later psychiatric disorders, such as SCZ and ASD. Moreover, as NRXN1 and other CAMs have previously been shown to play a significant role in SCZ and ASD, to continue examining CAMs is likely a fruitful endeavour. Finally we examined the cellular components that were found to be significantly burdened by CNVs in ASD and SCZ. These were cell junctions, plasma membrane and microtubules. The importance of cell junctions is particularly interesting as CAMs play a role in the maintenance of cell junctions. Therefore the dysfunction of genes in the cell junction component may support the dysfunction of CAMs, an accepted culprit in ASD and SCZ. The genes found in cell junctions in our data set include CLDN5, DSC3, DSG3 and ARVCF. As DSC3 and DSG3 were also included in cell adhesion clustering for biological process, and both show higher than average early expression up to 2.5 years of age, when introducing the details of our expression results. This would suggest that they would be key genes to investigate more closely. The association of CAMs with CNV: ASD and SCZ 20 cell junction genes, specifically DSC3 and DSG3, may elucidate the role of CAMs in SCZ and ASD. Moreover, these genes once again show higher than average expression in early development, supporting the hypothesis that early developmental problems may lay the groundwork for a multitude of psychiatric disorders, including SCZ and ASD. To summarize the clustering of genes found in CNVs detected SCZ and ASD, it would seem that the complexity of these disorders comes to the forefront, as many processes and functions are associated with these genes. Hopefully some clarity is brought to the results through the aid of previous literature, but these results will only be fully comprehended when a more in-depth investigation of these CNVs is done. It would seem that CAMs are of much interest in the progression of ASD and SCZ, and the dysfunction of CAMs is likely linked to the development of ASD and SCZ. Moreover, cell junctions may be of interest based on the overwhelming data suggesting CAM dysfunction as critical to ASD and SCZ and the association of cell junctions and CAMs. Finally the GABA and acetylcholine receptor activity is significantly burdened by CNVs in ASD and SCZ, and the genes involved show very early expression in development. Although these results are presented as the key trends in our data based on the previous literature, much of our data remains to be examined and is potentially very useful. While ASD and SCZ may seem like traditionally different disorders, this is not in fact completely true. ASD was initially considered a subtype of SCZ by Kanner in the early 1900’s (Kanner, 1943). ASD was later considered as distinct and separate from SCZ (Rutter, 1975) the prevailing clinical perception we still have today. More recently, Crespi et al. (2010) have re-introduced a relationship between SCZ and ASD reminiscent of Bleuler, although certainly different. Based on the examination of seven statistically significant CNV loci in ASD and SCZ they have suggested that ASD and SCZ may be diametrically opposite disorders. ASD tended to exhibit up-regulation of pathways due to loss of function mutations in negative regulators, contrasted with SCZ which tended to exhibit reduced pathway activation (Crespi et al., 2010). When examining this in conjunction with general brain size differences in ASD and SCZ, enhanced and reduced brain size respectively, it seems that ASD and SCZ may in fact be opposite ends of a CNV: ASD and SCZ 21 developmental spectrum. One should note that genes such as NRXN1 were in fact identically disrupted in ASD and SCZ in terms of functionality. Therefore the relationship is likely not a straight forward dichotomy, but in fact something more complex than that. While we have yet to examine the dosage dependant gain-loss of function of the CNVs discussed in this paper, there is a convergence of our results with Crespi et al. (2010) in that shared genetic aetiology is presented. It would seem safe to say that SCZ and ASD have a significant overlap in CNVs, however the relationship within our results needs to be examined, specifically the gain-loss of function. While the overlap is presented and discussed in detail, one should note that the majority of CNVs weren’t overlapping between ASD and SCZ (see figure 6). Figure 6: This is a visual representation of CNV overlap between SCZ, ASD and other psychiatric disorders, illustrating that while overlap exists the majority of the CNVs are outside of this overlap. It also illustrates that different types of overlap exists, CNVs shared by many psychiatric disorders including ASD and SCZ (black), CNVs shared by ASD and SCZ only (red), CNVs shared by either SCZ or ASD and other psychiatric disorders (green and blue respectively), and finally CNVs exclusive to a psychiatric CNV: ASD and SCZ 22 disorder such as ASD or SCZ (white). Based on our study SCZ showed 15.3% overlap with ASD, and conversely ASD showed 13.8% overlap with SCZ The CNVs that weren’t shared between ASD and SCZ likely represent two groups of genes, one group that is exclusive to SCZ or ASD development and the second group that overlaps with other psychiatric disorders. As mentioned, the overlap between psychiatric disorders doesn’t end with SCZ and ASD, but we see that many psychiatric disorders share some genetic aetiology (Craddock & Owen, 2010). Moreover, many of the CNVs shared by SCZ and ASD are likely also shared by many other psychiatric disorders. As mentioned this research follows a trend of recent studies examining the overlap of various psychiatric disorders including, but not limited to, SCZ, ASD, ADHD, bipolar disorder and epilepsy. As more evidence surfaces illustrating that psychiatric disorders have underlying genetic similarities there will come a time that a new model will be applied to understanding psychiatric disorders in general. A proposed system has been made by Craddock and Owen (2010) in which shared genetic variants, along with environmental pressures, effect a number of neural systems and ultimately are expressed as clinical symptoms associated with psychiatric disorders (see figure 7). CNV: ASD and SCZ 23 Figure 7: Proposed model between genotype variation and differing phenotype manifestation – a simplification (Craddock & Owen, 2010) This model illustrated how genetic variants (asterisks) influence different biological systems (blue arrows) and ultimately affect different neural modules (blue ovals). Also, environmental influences can shape different modules to express different clinical syndromes across the different domains on psycho-pathology. We see that a genetic variant (asterisks in figure 7) can have a number of influences over various biological systems, something that was also noted in the overwhelming data of the gene ontology analysis. It is here were genetic variants may lay the groundwork for later psychiatric dysfunction. The biological systems in turn influence a number of neural modules, it may also be here that environmental pressures channels the influence of the genetic variant towards a more specific neural module and ultimately a specific phenotype. Finally the neural modules influence a variety of psychopathological spectrums, which illustrate not only the spectrum of associated behaviours, but also the overlap between different domains of psychopathology often present in clinical practice. CNV: ASD and SCZ 24 It is this potential for broad influence that gives CNVs the capability of emitting different phenotypes from similar genotype differences. Examining the model proposed by Craddock & Owed (2010) in conjunction with our results we see how the model offers a potential method through which shared CNVs ultimately lead to different clinical symptoms. This is illustrated by genetic variants having a broad effect over various different neural modules, neural modules responsible for different symptoms such as mood and cognition. This effect is most obvious in our gene ontology data, as a number of genes have multiple functions and therefore affect multiple neural modules. The model also includes the need for other influences, both genetic and environmental, ultimately guiding an individual towards a specific psychiatric disorder are also taken into account. This includes the genetic variation not shared between psychiatric disorders, with repercussions on neural modules leading to specific symptoms, and environmental influence specifically altering the neural modules as the express specific symptoms. While this model is certainly a simplification of the entire process, it would seem to offer a number of benefits in understanding the data both in this paper and across the literature examining CNV overlap between psychiatric disorders. There are a number of limitations of which the reader should be cautioned when examining these results. Most notable is the lack of statistical significance when overlapping the CNVs between SCZ and ASD. This choice was made consciously as many rare CNVs, which were one of the main areas of focus for this paper, occur in such low levels compared to the sample sizes involved that they are immediately discarded. When this occurs there in no reassurance that these rare CNVs don’t play a significant role in the progression of the disorder, and these CNVs are therefore just as critical to examine. This certainly means that some of the genetic overlap between SCZ and ASD presented in this paper is not actually overlapping, but the breadth of overview offered in this paper compensates for this fact. Another limitation to address is the different origins of the data, as we collected CNV data across diverse literature. While aware that most of the time CNVs are found using different methodologies in different papers, one of the CNV: ASD and SCZ 25 primary goals of this paper was to increase the breadth of examined overlap between ASD and SCZ. As such we decided to compile data from across the field, regardless of the methods used. Moreover, we focused on including all rare CNVs found in patient groups presented in these papers, not only significant CNVs. Due to this there was no need to standardize the methodology of CNV discovery, as we are truly interested in any potential rare CNV. These limitations should not be underestimated or neglected, but the trade off for a more thorough examination of SCZ and ASD overlap was the primary goal of this paper. As SCZ and ASD are currently treated and discussed as different psychiatric disorders, this paper will hopefully challenge us to re-examine the relationship between SCZ and ASD more carefully. We have seen that there is some shared genetic aetiology between SCZ and ASD, and other literature further illustrates this overlap across a variety of psychiatric disorders. While psychiatric disorders clearly differ based on clinical symptoms, we should not assume that this means that the mechanisms responsible for these symptoms are also exclusively different between psychiatric disorders. In fact, this shared genetic aetiology is suggesting that there are similar mechanisms responsible for many psychiatric disorders. While the clinical symptoms differ, the process of developing these symptoms might be similar, and therefore treatment and a general understanding of psychiatric disorders requires an examination of this shared overlap between psychiatric disorders. This may ultimately lead to a new overview of psychiatric disorders, how they progress and how they are interrelated. The list of CNVs presented should open the possibility to examine the significance of CNVs and their influence on ASD and SCZ more closely. While a large amount of information is delivered in this paper the question still remains, which of these CNVs could be culprits in the progression of SCZ and ASD. Some suggestions have been made, such as DSG3 and DSC3 associated with cell junction and CAMs, or SCARF2 associated with CAMs and showing early expression during development. Also GABA and acetylcholine receptor activity, specifically GABRA5, GABRB3 and GABRG3 showed a significant CNV burden in ASD and SCZ and also showed early expression during development. However, this is just the beginning of potential research to better understand the relationship between SCZ CNV: ASD and SCZ 26 and ASD, and the relationship of all psychiatric disorders in general, based on the list of shared CNVs between SCZ and ASD. The purpose of this paper was to provide a comprehensive overview of CNVs in ASD and SCZ, the next step is to take the individual genes and examine them more closely. When are they expressed during development? Are they producing a gain or loss of function? Is the gain or loss of function the same in both ASD and SCZ, or rather do they oppose each other as suggested by Crespi et al. (2010)? The continuous dissection of the genetic influences shared by ASD and SCZ will be crucial not only in understanding and treating these respective disorders, but will likely play a huge role in our understanding of psychiatric disorders in general. This shared overlap is part of a larger trend in research examining the genetic overlap among virtually all psychiatric disorders, and may one day drastically alter our understanding of psychiatric disorders, their individual progression and their shared dysfunctions. CNV: ASD and SCZ 27 References: Bailey A., Le Couteur A., Gottesman I., Bolton P., Simonoff E., Yuzda E., and Rutter M. (1995) Autism as a strongly genetic disorder: evidence from a British twin study. Psychological medicine, 25, 63-77. Bradley, W.E., Raelson, J.V., Dubois, D.Y., Godin, E., Fournier, H., Prive, C., …Paulussen, R.J. (2010). Hotspots of large rare deletion in the human genome. PLoS One, 5(2), e9401 Bucan M., Abrahams B.S., Wang K., Glessner J.T., Herman E.I., Sonnenblick L.I., ... and Hakonarson H. (2009) Genome-wide analyses of exonic copy number variants in a family-based study point to novel autism susceptibility genes. PLoS Genetics. 5(6). Burbach, J.P., and van der Zwaag, B. (2009). Contact in the genetics of autism and schizophrenia. Trends in neuroscience. 32(2), 69-72. Cheung C., Yu K., Fung G., Leung M., Wong C., Li Q., Sham P., Chua S., and McAlonan G. (2010). Autistic disorders and schizophrenia: related or remote? An anatomical likelihood estimation. PLoS One, 18:5(4). Ching, M.S., Shen, Y., Tan, W.H., Jeste, S.S., Morrow, E.M., Chen, X.,… Children’s Hospital Boston Genotype Phenotype Study Group. (2010). Deletions of NRXN1 (neurexin-1) predispose to a wide spectrum of developmental disorders. American Journal of Medical Genetics Part B, Neuropsychiatric Genetics, 153B(4), 937947. Cook, E.H. Jr., and Scherer, S.W.. (2008). Copy-number variatios associated with neuropsychiatric conditions. Nature, 455(7215), 919-923. CNV: ASD and SCZ 28 Corvin, A. P. (2010). Neuronal cell adhension genes: Key players in risk for schizophrenia, bipolar disorder and other neurodevelopmental brain disorders? Cell adhesion and migration, 26:4(4). Coyle, J.T., Balu, D., Benneyworth, M., Basu, A., and Roseman, A. (2010). Beyond the dopamine receptor: novel therapeutic targets for treating schizophrenia. Dialogues in clinical neuroscience. 12(3), 359-382. Craddock, N., and Owen, M.J. (2010). The Kraepelinian dichotomy – going, going… but still not gone. The British Journal of Psychiatry: The journal of mental science. 196(2), 92-95. Crespi, B., Stead, P., and Elliot, M. (2010) Comparitice genomics of autism and schizophrenia. PNAS, 107, 1736-1741. Feuk L., Carson A.R., and Scherer S.W. (2008). Structural variation in the human genome. Nature Review Genetics, 7, 85-97. Guilmatre A., Dubourg C., Mosca A. L., Legallic S., Goldenberg A., DrouinGarraud V., and Campion D. (2009). Recurrent rearrangement in synaptic and neurodevelopmental genes and shared biologic pathways in schizophrenia, autism, and mental retardation. Archives of general psychiatry, 66, 947-956. Glessner, J., Reilly, M., Kim, C., Takaheshi, N., Albano, A., Hou, C., … and Hakonarson, H. (2010). Strong synaptic transmission impact by copy number variations in schizophrenia. PNAS, 107(23, 10584-10589. CNV: ASD and SCZ 29 Glessner J.T., Wang K., Cai G., Korvatska O., Kim C.E., Wood S., ... and Hakonarson H. (2009) Autism genome-wide copy number variation reveals ubiquitin and neuronal genes. 459(7246), 569-573. Hajos, M., and Roger, B.N. (2010). Targeting the alpha7 nicotinic acetycholine receptors in the treatment of schizophrenia. Current pharmaceutical design. 16(5), 538554. International Schizophrenia Consortium. (2008). Rare chromosomal deletions and duplications increase risk of schizophrenia, Nature 455, 237–241. Kanner L. (1943). Autistic disturbances of affective contact. Nervous Child 1943; 2: 217 –50. Kim H.G., Kishikawa S., Higgins A.W., Seong I.S., Donovan D.J., Shen Y., … and Gusella J.F. (2008). Disruption of neurexin 1 associated with autism spectrum disorder. 82(1), 199-207. Kirov, G., Grozeva, D., Norton, N., Ivanov, D., Mantripragada, K. K., Holmans, P., … and O’Donovan, M., C. (2009). Support for the involvement of large copy number variants in the pathogenesis of schizophrenia. Human Molecular Genetics, 18(8), 14791503. Kirov G., Rujescu D., Ingason A., Collier D.A., O'Donovan M.C., and Owen M.J. (2009) Neurexin 1 (NRXN1) deletions in schizophrenia. Schizophrenia Bulletin. 35(5), 851-854. Kumar R.A., and Christian S.L. (2009) Genetics of autism spectrum disorders. Current neurology and neuroscience reports. 9(3), 188-197. CNV: ASD and SCZ 30 Kumar R.A., Kara-Mohamed S., Sudi J., Conrad D.F., Brune C., Badner J.A., ... and Christian S.L. (2008). Recurrent 16p11.2 microdeletions in autism. Human Molecular Genetics, 17(4), 628-638. Lee, C. H., Liu, C. M., Wen, C. C., Chang, S. M., and Hwu, H. G. (2010). Genetic copy number variants in sib pairs both affected with schizophrenia. Journal of Biomedical Science, 17(1): 2. Lee, M., Martin-Ruiz, C., Graham, A, Court, J., Jaros, E., Perry, R., … and Perry, E. (2002). Nicotinic receptor abnormalities in the cerebellar cortex in autism. Brain. 125(7), 1483-1495. Leyfer O., Folstein S., Bacalman S., Davis N., Dinh E., Morgan J., Tager-Flusberg H., and Lainhart J. (2006). Comorbid psychiatric disorders in children with autism: Interview development and rates of disorders. Journal of autism and developmental disorders, 36, 849-861. Lippiello, P.M.(2006). Nicotinic cholinergic antagonists: a novel approach for the treatment of autism. Medical hypotheses. 66(5), 985-990. Magri, C., Sacchetti, E., Traversa, M., Valsecchir, P., Gardella, R., Bonvicini, C., …, and Barlatil, S. (2010) New copy number variation in schizophrenia. PLoS One, 5(10): e13422. Marshall C.R., Noor A., Vincent J.B., Lionel A.C., Feuk L., Skaug J., … and Scherer S.W. (2008) Structural variation of chromosome in autism spectrum disorder. American Journal of Human Genetics. 82(2), 477-488. CNV: ASD and SCZ 31 Mefford H.C., Cooper G.M., Zerr T., Smith J.D., Baker C., Shafer N., … and Eichler E.E. (2009) A method for rapid, targeted CNV genotyping identifies rare variants associated with neurocognitive disease. Genome Research. 19(9), 1579-1585. Mi, H., Lazareva-Ulitsky, B., Loo, R., Kejariwal, A., Vandergriff, J., Rabkin, S., … Thomas, P. (2005). The PANTHER database of protein families, subfamilies, functions and pathways. Nucleic Acids Research. 33(suppl.1), D284-D288. Oblak, A.L., Gibba, T.T., and Blatt, G.J. (2010). Reduced GABA(A) receptors and benzodiazepine binding sites in the posterior cingulated cortex and fusiform gyrus in autism. Brain research. Epub ahead of print. Pang, A.W., MacDonald, J.R., Pinto, D., Wei, J., Rafig, M.A, Conrad, D.F., …Scherer, S.W. (2010). Towards a comprehensive structural variation map of an individual human genome. Genome Biology, 11(5), R52. Perl, O., Ilani, T., Strous, R.D., Lapidus, R., and Fuchs, S. (2003). The alpha7 nicotinic acetylcholine receptor in schizophrenia: decreased mRNA levels in peripheral blood lymphocytes. Federation of America societies for experimental biology. 17, 19481950. Pinto D., Pagnamenta A.T., Klei L., Anney R., Merico D., Regan R., … and Betancur C. (2010). Functional impact of global rare copy number variation in autism spectrum disorders. Nature. 466(7304), 368-372. Protein ANalysis THrough Evolutionary Relationships (PANTHER): Version 7.0. (2010) www.pantherdb.org. CNV: ASD and SCZ 32 Ray, M., Graham, A., Lee, M., Perry, R., Court, J., and Perry E. (2005). Neuronal nicotinic acetylcholine receptor subunits in autism: an immunohistochemical investigation in the thalamus. Neurobiology of disease. 19(3), 366-377. Redon, R., Ishikawa, S., Fitch, K.R., Feuk, L., Perry, G.H., Andrews, T.D.,… Hurles, M.E. (2006). Global variation in copy number in the human genome. Nature, 444, 444-454 Rujescu D., Ingason A., Cichon S., Pietiläinen O.P., Barnes M.R., Toulopoulou T., … and Collier D.A. (2009). Disruption of the neurexin 1 gene is associated with schizophrenia. Human molecular genetics. 18(5), 988-996. Rutter, M. (1975). Childhood schizophrenia reconsidered. Journal of autism and developmental disorders, 2(3), 315-337. Shelling, A.N., and Ferguson, L.R. (2007). Genetic variation in human disease and a new role for copy number variants. Mutation Research: Fundamental and Molecular Mechanisms of Mutagenesis, 622, 33-41. Stefansson H., Ophoff R.A., Steinberg S., Andreassen O.A., Cichon S., Rujescu D., … and Collier D.A. (2009). Common variants conferring risk of schizophrenia. Nature. 460(7256), 744-747. Stefansson H., Rujescu D., Cichon S., Pietiläinen O.P., Ingason A., Steinberg S., … and Stefansson K. (2008) Large recurrent microdeletions associated with schizophrenia. Nature. 455(7210), 232-236. Stranger B.E., Forrest M.S., Dunning M., Ingle C.E., Beazley C., Thorne N., … and Dermitzakis E.T. (2007). Relative impact of nucleotide and copy number variation on gene expression phenotypes. Science. 315(5813), 848-853. CNV: ASD and SCZ 33 Sullivan, P. F., Kendler, K. S., and Neale, M. C. (2003). Schizophrenia as a complex trait: evidence from a meta-analysis of twin studies. Archives of general psychiatry, 60, 1187-1192. Toro R., Konyukh M., Delorme R., Leblond C., Chaste P., Fauchereau F., … and Bourgeron T. (2010) Key role for gene dosage and synaptic homeostasis in autism spectrum disorders. Trends in genetics. 26(8), 363-372 Tam, G., van de Langemaat, L., Redon, R., Strathdee, K., Croning, M.Malloy, M., ..., and Grant, S. (2010). Confirmed rare copy number variants implicate novel genes in schizophrenia. Biochemical Society Transactions, 38, 445-451. Thomas, P., Campbell, M., Kejariwal, A., Mi, H., Karlak, B., Daverman, R., … Narechania, A. (2003) PANTHER: A library of protein families and subfamilies indesxed by function. Genome Research, 13, 2129-2141. van der Zwaag B., Franke L., Poot M., Hochstenbach R., Spierenburg H.A., Vorstman J.A., ... and Staal W.G. (2009). Gene-network analysis identifies susceptibility genes related to glycobiology in autism. PLoS One. 28(4), e5324. Vrijenhoek T., Buizer-Voskamp J.E., van der Stelt I., Strengman E.; Genetic Risk and Outcome in Psychosis (GROUP) Consortium, Sabatti C., … and Veltman J.A. (2008). Recurrent CNVs disrupt three candidate genes in schizophrenia patients. American Jounral of Human Genetics, 83(4), 504-510. Wang, K.S, Liu, X.F., and Aragam, N.(2010) A genome-wide meta-analysis identifies novel loci associated with schizophrenia and bipolar disorder. Schizophrenia Research, 124(1-3), 192-199. CNV: ASD and SCZ 34 Wassef, A., Baker, J., and Kochan, L.D. (2003). GABA and schizophrenia: a review of basic science and clinical studies. Journal of clinical psychopharmacology. 23 (6), 601-640. Weiss L.A., Shen Y., Korn J.M., Arking D.E., Miller D.T., Fossdal R., … and Autism Consortium. (2008) Association between microdeletion and microduplication at16p11:2 and autism. New England Journal of Medicine, 358(7), 667-675. Wilson G., Flibotte S., Chopra V., Melnykl B., Honer W., and Holt R. (2006). DNA copy-number analysis in bipolar disorder and schizophrenia reveals aberrations in genes invlved in glutamate signalling. Human Molecular Genetics, 15(5), 743-749. Wiśniowiecka-Kowalnik B., Nesteruk M., Peters S.U., Xia Z., Cooper M.L., Savage S., … and Stankiewicz P. (2010) Intragenic rearrangments in NRXN1 in three families with autism spectrum disorder, developmental delay, and speech delay. American Journal of medical genetics. Part B, Neuropsychiatric Genetics: the official publication for the international society of psychiatric genetics. 153B(5), 983-993. Xu B., Roos J.L., Levy S., van Rensburg E.J., Gogos J.A., and Karayiorgou M. (2008). Strong association of de novo copy number mutations with sporadic schizophrenia. Nature Genetics, 40(7), 880-885 Xu B., Woodroffe A., Rodriguez-Murillo L., Roos J. L., van Rensburg E. J., Abecasis G. R., …, and Karayiorgou M. (2009). Elucidating the genetic architecture of familial schizophrenia using rare copy number variant and linkage scans. PNAS, 106(39), 16746-51. CNV: ASD and SCZ 35 Supplementary Materials: Supplementary 1: Significant molecular functions and their associated CNV disrupted genes Genes involved Significance (p value) Acetylcholine GABRG3, GABRA5, GABRB3 0.00235 GABRG3, GABRA5, GABRB3 0.00235 Cytoskeleton TEKT3, TSSK2, TPPP, TUBGCP5, KLHL22, 0.0061 protein binding CAMK1D, ARVCF Tranferase TSSK2, PRIM2A, MAPK3, HS3ST3B1, SEPHS1, activity TAOK2, HTF9C, B#GAT1, LARGE, ALG10, MLL3, receptor activity GABA receptor activity 0.0143 OCA2, ERBB4 Lipid transporter SEZ6L2, NRXN1, CSMD1 0.0246 GABRG3, GABRA5, GABRB3 0.0373 HTF9C, MLL3, COMT 0.0373 GRM7, SEZ6L2, NRXN1, SCARF2, TRPM1, 0.0403 activity Ligand-gated ion channel activity Methyltransferas e activity Receptor activity GABRG3, GABRA5, RTNR4, CSMD1, VIPR2, GABRB3, ERBB4 Calcium ion binding TSSK2, DSC3, SCARF2, DSG3, OCA2, PPP4C, 0.0406 CNV: ASD and SCZ 36 Supplementary 2: Significant biological processes and their associated CNV disrupted genes Genes involved Significance (p value) Developmental UBE3A, TEKT3, TSSK2, PMP22, CLDN5, process SCARF2, NRXN1, DGCR13, RTRN4, TPPP, 0.00314 MAPK3, VIPR2, TUBGCP5, KLHL22, TBC1D5, OCA2, HERC2, PARK2, PHYH, GSC2, ERBB4, TBX6, CNTN4, CAMK1D, KLF13, TBX1 Oxygen and oxygen TXNRD2, PMP22, MPV17L 0.00531 Anion transport GABRG3, GABRA5, GABRB3, OCA2 0.00989 Mesoderm UBE3A, TSSK2, NRXN1, SCARF2, RTN4R, 0.00990 development MAPK3, HERC2, VIPR2, CA2, TBX6, GSC2, reactive species metabolic process ERBB4, CNTN4, KLF13, TBX1 Cell adhesion SEZ6L2, NRXN1, SCARF2, DSC3, RTN4R, 0.0153 CSMD1, DSG3, GPC6, VIPR2, ERBB4, CNTN4, ARVCF, NDN Protein metabolic UBE3A, YPEL3, UBE2L3, TSSK2, MKRN3, process SEZ6L2, PRKAG2, NRXN1, CSMD1, MAPK3, 0.0166 HS3ST3B1, KLHL22, OCA2, TAOK2, HERC2, PARK2, LARGE, ALG10, ERRBB4, EHHADH, PPP4C, CNTN4, CAMK1D, SERPIND1, MRPL40, UFD1L Skeletal system UBE3A, NRXN1, SCARF2, RTN4R, HERC2, development GSC2 Neurological system GRM7, TSSK2, CLTCL1PMP22, NRXN1, process SCARF2, DOC2A, GABRG3, GABRA5, VIPR2, KLHL22, RAB23, PMP22, OCA2, GABRB3, CAMK1D, RXRA, COMT, GNB1L 0.0193 0.0212 CNV: ASD and SCZ Meiosis TSSK2, OCA2, PPP4C, CAMK1D 0.0223 Cell cycle CDC45L, TSSK2, MKRN3, PMP22, PRIM2A, 0.0244 SEPT5, MAPK3, TUBGCP5, RAB23, OCA2, ERBB4, CNTN4, PPP4C, CAMK1D, RXRA, HIRA, NDN Cellular calcium ATP2C2, ATP10A 0.0328 SEZ6L2, DSC3, NRXN1, SCARF2, DSG3, 0.0333 homeostasis Cell-cell adhesion RTN4R, CSMD1, ERBB4, CNTN4 System process GRM7, TSSK2, CLTCL1, PMP22, NRXN1, 0.0347 SCARF2, DOC2A, GABRG3, GABRA5, VIPR2, KLHL22, RAB23, OCA2, GABRB3, CNTN4, CAMK1D, RXRA, COMT, GNB1L Homeostatic process ATP2C2, ATP10A, VIPR2 0.0446 Lipid metabolic YPEL3, GDPD3, ABCA13, SLC25A1, PRKAG2, 0.0455 process ATP2C2, NUDT3, PHYH, EHHADH, RXRA, ATP10A Cellular component TEKT3, TSSK2, PMP22, CLDN5, TPPP, morphogenesis DGCR13, TUBGCP5, KLHL22, TBC1D5, 0.0460 CAMK1D Anatomical structure TEKT3, TSSK2, PMP22, CLDN5, TPPP, morphogenesis DGCR13, TUBGCP5, KLHL22, TBC1D5, 0.0460 CAMK1D Synaptic CLTCL1, DOC2A, NRXN1, GABRG3, transmission GABRA%, GABRB3, COMT Cell communication GRM7, TSSK2, CLTCL1, MKRN3, SEZ6L2, PRKAG2, SCARF2, NRXN1, SHANK3, DOC2A, DSC3, CYFIP1, CSMD1, GABRG3, GABRA5, RTN4R, DSG3, MAPK3, HS3ST3B1, VIPR2, RAB23, OCA2, PARK2, ERBB4, GABRB3, PPP4C, CNTN4, CAMK1D, COMT, RXRA 0.0471 0.0477 37 CNV: ASD and SCZ Lipid transport ABCA13, SLC25A, ATP2C2, ATP10A 38 0.0481 Supplementary 3: Significant cellular components and their associated CNV disrupted genes Genes involved Significance (p value) Cell junction CLDN5, DSC3, DSG3, ARVF 0.00472 Plasma membrane CLDN5, DSC3, DSG3, ARVF 0.00622 Microtubule TEKT3, TSSK2, TPPP, TUBGCP5, CAMK1D 0.0444 Supplementary 4: Expression Analysis See attached PowerPoint for expression data overview. -Slides 2-4: expression analysis for shared CNVs between ASD and SCZ across brain regions. -Slides 5-7: expression analysis for shared CNVs between ASD and SCZ over time. -Slide 8: expression analysis for all CNVs in ASD over time -Slide 9: expression analysis for all CNVs in ASD across brain regions -Slide 10: expression analysis for CNVs in SCZ across brain regions -Slide 11: expression analysis for CNVs in SCZ over time -Slide 12: expression analysis for CNVs only in SCZ over time -Slide 13: expression analysis for CNVs only in SCZ across brain regions -Slide 14: expression analysis for CNVs only in ASD over time -Slide 15: expression analysis for CNVs only in ASD across brain regions