Community Acquired Pneumonia (CAP) Diagnosis The diagnosis of
advertisement
 Diagnosis The diagnosis of")
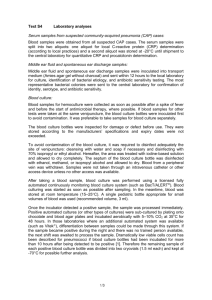
Community Acquired Pneumonia (CAP) Diagnosis The diagnosis of pneumonia should be considered in any patient who has newly acquired respiratory symptoms (cough, sputum production, and/or dyspnea), especially if accompanied by fever and abnormal breathing sounds and crackles. In patients with advanced age or an inadequate immune response, pneumonia may present with non-respiratory symptoms such as confusion, failure to thrive, worsening of an underlying chronic illness, or falling down. In these patients, fever may be absent, but tachypnea is usually present. Diagnosis studies Chest radiograph Standard PA and lateral chest radiographs are valuable in patients whose symptoms and physical examination suggest the possibility of pneumonia. The radiographic findings may suggest specific etiologies or conditions which as lung abscess, or tuberculosis. The radiograph can also identify coexisting conditions such as bronchial obstruction or pleural effusion. Radiography is also useful for evaluating severity of illness by identifying multilobar involvement. Sputum Gram’s stain and culture Routine bacterial cultures of sputum often demonstrate pathogenic organisms, but sensitivity and specificity are poor, and findings should be correlated with the predominant organism identified on Gram’s stain. When drug-resistant pneumococci, other resistant pathogens, or organisms not covered by the usual empiric therapy options are anticipated, sputum culture and sensitivity results may be useful. Direct staining of sputum (non-Gram method) may be diagnostic for some pulmonary infection, including those due to Mycobacterium sp., endemic fungi, Legionella sp., and Pneumocytic carinii. Specialized cultures for Mycobacterium sp., Legionella sp., and endemic fungi may be valuable in the appropriate clinical circumstance. Viral culture is not useful in the initial evaluation of patient with CAP and should not be routinely performed. In the appropriate season, testing of respiratory secretions for influenza antigens, using rapid detection methods, may be helpful in guiding decisions about the use of new antiviral agents. PORT Prediction Rule Model Age over 65 y/o Presence of coexisting illness Chronic obstructive lung disease Bronchiectasis Malignancy Diabetes mellitus Chronic renal failure Congestive heart failure Chronic liver disease Chronic alcohol abuse History of hospitalization within the past year Physical finding Respiratory rate ≥ 30 breaths/min Diastolic BP ≤ 60 mmHg or systolic BP ≤ 90 mmHg Pulse ≥ 125/min BT < 35 or ≥ 40°C Confusion or decreased level of consciousness Evidence of extrapulmonary sites of infection Laboratory findings WBC < 4 × 109/L or > 30 × 109/L, or ANC < 1 × 109/L PaO2 < 60 mmHg or PaCO2 > 50 mmHg while breathing room air Serum creatinine > 1.2 mg/dl or BUN > 20 mg/dl Presence of certain unfavorable chest radiograph findings More than on lobe involvement, presence of a cavity, rapid radiographic spreading Presence of a pleural effusion Evidence of sepsis or organ dysfunction manifested by a metabolic acidosis or coagulopathy Arterial pH < 7.35 Malnutrition Cerebrovascular disease Post-splenectomy Severe CAP Minor PaO2/FiO2 < 250 Bilateral pneumonia or multilobar pneumonia 2 Systolic BP ≤ 90 mmHg Major Need for mechanical ventilation Septic shock or need for pressors for > 4 hrs Meet 2 minor or 1 major criteria Recommended Tests Chest radiograph Complete blood count and differential count Routine blood chemistry test Including glucose, liver and renal function, and electrolytes Oxygen saturation assed by oximetry Artery blood gas In patient with severe illness or chronic lung disease Sputum culture and smear Blood culture Two sets, before initiation of antibiotic therapy Pleural effusion To rule out empyema, or complicated parapneumonic effusion Including white blood cell count and differential count, measurement of protein, glucose, lactase dehydrogenase (LDH), and pH, Gram’s stain and acid-fast stain, and culture for bacteria, fungi, and mycobacteria Urine Legionella Ag (serogroup 1) 3 CAP is present OUTPATIENT NO CARDIOPULMONARY DISEASE, NO MODIFIERS GROUP 1, TABLE 2 INPATIENT HISTORY OF CARDIO-PULMONARY DISEASE, AND/OR MODIFIERS MILD-MODRATE ILLNESS SEVERE CAP GROUP II, TABLE 3 CARDIOPULMONARY DISEASE AND/OR MODIFIERS NO CARDIOPULMONARY DISEASE, NO MODIFIERS NO RISKS FOR PSEUDOMAS AEROGINOSA RISKS FOR PSEUDOMAS AEROGINOSA GROUP IIIA TABLE 4A GROUP IIIA TABLE 4B GROUP IIIA TABLE 5A GROUP IIIA TABLE 5A Table 1. MODIFYING FACTORS THAT INCREASE THE RISK OF INFECTION WITH SPECIFIC PATHOGENS Penicillin-resistant and drug-resistant pneumococci Age > 65 yr β-Lactam therapy within the past 3 mo Alcoholism Immune-supressive illness (including therapy with corticosteroids) Multiple medical comorbidities Exposure to a child in a day care center Enteric gram-negatives Residence in a nursing home Underlying cardiopulmonary disease Multiple medical comorbidities Recent antibiotic therapy Pseudomonas aeruginosa Structural lung disease (bronchiectasis) Corticosteroid therapy (> 10 mg of prednisone per day) Broad-spectrum antibiotic therapy for > 7 d in the past month Malnutrition 4 Table 2. GROUP I: OUTPATIENTS, NO CARDIOPULMONARY DISEASE, NO MODIFYING FACTORS Organisms Streptococcus pneumoniae Mycoplasma pneumoniae Clamydia pneumoniae (alone or as mixed infection) Hemophilus influenzae Respiratory viruses Miscellaneous Legionella spp. Therapy Advanced generation macrolide: azithromycin or clarithromycin or Doxycycline Mycobacterium tuberculosis Endemic fungi Table 3. GROUP II: OUTPATINT, WITH CARDIOMPULMONARY DISESE, AND/OR MODIFYING FACTORS Organisms Therapy Streptococcus pneumoniae (including β-Lactam (oral cefpodoxime, DRSP) Mycoplasma pneumoniae Chlamydia pneumoniae Mixed infection (bacteria plus atypical pathogen or virus) Hemophilus influenzae Enteric gram-negatives Miscellaneous Moraxella catarrhalis, Legionella spp., aspiration (anaerobes), Mycobacterium cefuroxime, high-dose amoxicillin, amoxicillin/clavulanate; or parenteral ceftriaxone followed by oral cefpodoxime) plus Macrolide or doxycylline or Antipneumococcal fluoroquinolone (used alone) tuberculosis, endemic fungi 5 Table 4. GROUP III: INPATIENTS, NOT IN ICU Organisms Therapy A. Cardiopulmonary Disease and/or Modifying Factors (Including Being from a Nursing Home) Streptococcus pneumoniae (including DRSP) Hemophilus influenzae Mycoplasma pneumoniae Chlamydia pneumoniae Mixed infection (bacteria plus atypical Intravenous β-lactam (cefotaxime, pathogen) Enteric gram-negatives Aspiration (anaerobes) Viruses fluoroquinolone alone ceftriaxone, ampicillin/sulbactam, high-dose ampicillin) plus intravenous or oral macrolide or doxycyline or intravenous antipneumococcal Legionella spp. Miscellaneous Mycobacterium tuberculosis, endemic fungi, pneumocystic carinii B. No Cardiopulmonary Disease, No modifying factors S. pneumoniae Intravenous azithromycin alone H. influenzae M. pneumoniae C. pneumoniae Mixed infection (bacteria plus atypical pathogens) Viruses Legionella spp. Miscellaneous M. tuberculosis, endemic fungi, P. carinii If macrolide allergic or intolerant: Doxycyline and a β-lactam or Monotherapy with an antipneumococcal fluoroquinolone 6 Table 5. GROUP IV: ICU-ADMITTED PATIENTS Organisms Therapy A. No risk for Pseudomonas aeruginosa Streptococcus pneumoniae (including DRSP) Legionella spp. Hemophilus influenzae Enteric gram-negative bacilli Staphylococcus aureus Mycoplasma pneumoniae Intravenous β-lactam (cefotaxime, cefriaxone) plus either Intravenous macrolide (azithromycin) or Intravenous fluoroquinolone Respiratory viruses Miscellaneous Chlamydia pneumoniae, Mycobacterium tuberculosis, endemic fungi B. Risks for Pseudomonas aeruginosa All of the above pathogens plus P. aeruginosa Selected intravenous anti-pseudomonal β-lactam (cefepime, imipenem, meropenem, piperacillin/tazobactam) plus intravenous anti-pseudomonas quinolone (ciprofloxacin) Or Selected intravenous anti-pseudomonal β-lactam (cefepime, imipenem, meropenem, piperacillin/tazobactam) plus intravenous aminoglycoside Plus either Intravenous macrolide (azithromycin) Or intravenous non-pseudomonal fluoroquinolone 7 Antibiotic Therapy Administer the first dose in 8 hrs from the time of arrival to the hospital. Length of therapy: 7-14 days Switching to oral therapy Patient who is clinically stable, may switch to oral therapy on day 3 of hospital stay, if: 1. Improvement in cough and dyspnea 2. Afebrile on 2 occasions 8 hrs apart 3. WBC is decreased 4. GI tract is functioning with adequate intake Organism-specific if etiologic pathogen is known If specific pathogen is not known, continue treatment with parenteral agent with wide spectrum of activity. 8