REVIEW REQUEST FOR
advertisement

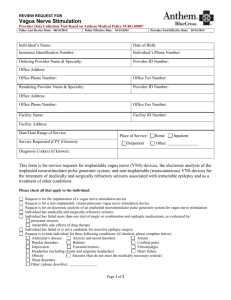
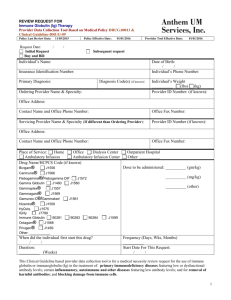
REVIEW REQUEST FOR Immune Globulin (Ig) Therapy Complete form in its entirety and fax to: Anthem Blue Cross 866-408-7195 Provider Data Collection Tool Based on Medical Policy DRUG.00013 & Clinical Guideline-DRUG-09 Policy Last Review Date: 05/15-2014 Request Date: / Initial Request Buy and Bill Policy Effective Date: 07/15/2014 Provider Tool Effective Date: 07/15/2014 / Subsequent request Individual’s Name: Date of Birth: / / Individual’s Phone Number: Insurance Identification Number: Primary Diagnosis: Diagnosis Code(s) (if known): Ordering Provider Name & Specialty: Individual’s Weight (lbs) (kg) Provider ID Number: (if known): Office Address: Contact Name and Office Phone Number: Office Fax Number: Servicing Provider Name & Specialty (If different than Ordering Provider): Provider ID Number (if known): Office Address: Contact Name and Office Phone Number: Place of Service: Home Ambulatory Infusion Office Fax Number: Office Dialysis Center Ambulatory Infusion Center Outpatient Hospital Other: Drug Name/HCPCS Code (if known) Immune Globulin 90281 90283 90284 Privigen® J1459 Gamma Globulin J1460 Bivigam® J1556 Gammaplex® Hizentra® J1559 Gamunex-C®/Gammaked Carimune® J1566 Octagam® Gammagard® J1569 J1599 Dose to be administered: J1560 Flebogamma® /Flebogamma® DIF (mg/kg) J1557 (other) J1561 J1568 J1572 Other: When did the individual first start this drug? / / Duration: (Weeks) Frequency (Days, Wks, Months) Start Date For This Request: / / Page 1 of 5 Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association. Please check all that apply to the individual: Immune Globulin (Ig) therapy for the treatment of an individual with the following: A. B. Antenatal Alloimmune Thrombocytopenia Auto-immune mucocutaneous blistering diseases (that are refractory) including: pemphigus vulgaris, pemphigus foliaceus, bullous pemphigoid, mucous membrane pemphigoid, and epidermolysis bullosa aquisita C. Autoimmune Neutropenia D. Chronic inflammatory demyelinating polyneuropathy (CIDP) (Please check the following that apply): Initial Authorization: As initial trial (up to 12 weeks) for chronic inflammatory demyelinating polyneuropathy (CIDP) and the clinical presentation is not consistent with other polyneuropathies (for example, IgM neuropathy, hereditary neuropathy, diabetic neuropathy) (Please check the following that apply): Proximal muscle weakness or sensory dysfunction caused by neuropathy and nerve conduction studies (NCS) confirm there is electrodiagnostic evidence of demyelinating neuropathy in at least 2 limbs Distal muscle weakness and results of diagnostic testing meet a recognized set of diagnostic criteria as established by the American Academy of Neurology (AAN), or Inflammatory Neuropathy Cause and Treatment (INTAC). (If checked, please indicate which criteria used and which diagnostic tests meet): Reauthorization: Clinically significant improvement in neurological symptoms is documented on physical examination. (If checked, please note improvements): Has been on treatment for less than 1 year Has been on treatment for at least 1 year and continued need is demonstrated by documentation that attempts on an annual basis to titrate the dose or the interval of therapy result in worsening symptoms. (If checked, please document dosage change and results): E. Dermatomyositis refractory to corticosteroid therapy (IVIG will be used as second line treatment after corticosteroid therapy failed) F. Eaton-Lambert myasthenic syndrome G. Guillain-Barr syndrome (acute demyelinating polyneuropathy) as an alternative to plasma exchange H. Human immunodeficiency virus (HIV) infected pediatric individual - prevention of opportunistic bacterial infections I. Hyperimmunoglobulinemia E syndrome (HIE) treatment Page 2 of 5 Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association. J. K. L. Hypogammaglobulinemia and recurrent bacterial infections associated with B-cell chronic lymphocytic leukemia (CLL) (Please check the following that apply): Documented history of recurrent bacterial infection or an active infection not responding to antimicrobial therapy Documented total IgG is less than 500 mg/dl IgG sub-class deficiency (IgG1, IgG2, IgG3, IgG4) (Please check the following that apply): One or more serum IgG subclasses are more than two standard deviations below the lower limits of the age adjusted norms History of recurrent sinopulmonary infections requiring antibiotic therapy There is documentation of a lack of, or inadequate response to, immunization (for example, but not limited to pneumococcal antigen) Immune thrombocytopenia (idiopathic thrombocytopenic purpura (ITP) (Please check the following that apply): Symptomatic thrombocytopenia (for example, but not limited to hematuria, petechiae, bruising, gastrointestinal bleeding, gingival bleeding) Platelet count less than 20,000 per microliter (mcL) (adult) Platelet count less than 30,000 per microliter (mcL) (child) M. Kawasaki Syndrome (Please check the following that apply): Within 10 days of onset of symptoms Treatment planned for no more than 5 days N. Multifocal Motor Neuropathy (MMN) (Please check the following that apply): Initial Authorization: Initial trial (up to 4 weeks) Asymmetric weakness that predominately affects distal muscles (without upper motor neuron signs) and nerve conduction studies confirm a demyelinating neuropathy is present (conduction block, slowing, or abnormal temporal dispersion in at least one nerve) Clinical history and exam do not suggest upper motor neuron disease (no bulbar weakness, no upper motor neuron signs) Labs show GM-1 antibody titers are elevated. (If checked, please document GM-1 antibody titer): Clinical presentation suggests MMN but diagnosis remains uncertain following initial exam and electrodiagnostic testing Reauthorization: Continued use after initial trial Clinical results documented an improvement in strength and function within 3 weeks of the start of the infusion period. (If checked, please note improvements): Has been on treatment for less than 1 year Has been on treatment for at least 1 year and continued need is demonstrated by documentation that attempts on an annual basis to titrate the dose or the interval of therapy result in worsening symptoms. (If checked, please document dosage change and results): O. Myasthenia Gravis which is severe and refractory to standard therapy P. Neonates - To prevent infections in high-risk, preterm, low birth weight Q. Parvovirus B19 chronic infection and severe anemia associated with bone marrow suppression Page 3 of 5 Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association. R. Severe polymyositis when other treatments have been unsuccessful, intolerable, or are contraindicated (If checked, please list previous treatments and results): S. Primary humoral immunodeficiency (If checked, please specify): Individual has a history of recurrent sinopulmonary infections requiring antibiotic therapy There is a lack of, or inadequate response to immunization (for example, but not limited to pneumococcal antigen) There is no evidence of renal (nephrotic syndrome) and gastrointestinal (for example protein losing enteropathy) as causes of hypogammaglobulinemia The initial, pre-treatment total serum IgG is more than two standard deviations below the lower limits of the age adjusted mean T. U. V. Primary humoral immunodeficiency - Other (for example, congenital agammaglobulinemia, X-linked immunodeficiency, severe combined immunodeficiency [SCID], or Wiskott-Aldrich syndrome [WAS]) when (please check all that apply): There is no evidence of renal (nephrotic syndrome) and gastrointestinal (for example, protein losing enteropathy) as causes of hypogammaglobulinemia The initial, pre-treatment total serum IgG is more than two standard deviations below the lower limits of the age adjusted mean Stiff-person syndrome not controlled by other therapies Toxic shock syndrome caused by staphylococcal or streptococcal organisms refractory to several hours of aggressive therapy W. Transplant Hematopoietic stem cell transplant (Please check the following that apply): Allogeneic bone marrow transplant (BMT) recipient in the first 100 days after transplantation To reduce risk of graft-versus-host disease associated with interstitial pneumonia (infectious or idiopathic) and infections (cytomegalovirus infections, varicella-zoster virus infection, and recurrent bacterial infection) Secondary hypoglobulinemia in an immunosuppressed individual (for example, status post bone marrow transplant) Documented total IgG less than 500 mg/dl Solid organ transplant (Please check the following that apply): Prior to a medically necessary solid organ transplantation For suppression of panel reactive anti-HLA antibodies and individuals with high panel reactive antibody (PRA) levels to human leukocyte antigens (HLA) Solid organ transplant recipients at risk for CMV X. Other Indications To prevent recurrent spontaneous abortions Alzheimer’s disease Immune optic neuropathy Multiple sclerosis Other: Page 4 of 5 Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association. This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number I attest the information provided is true and accurate to the best of my knowledge. I understand that the health plan or its designee may perform a routine audit and request the medical documentation to verify the accuracy of the information reported on this form. / / Name & Title of Provider or Provider Representative Completing Form Date & attestation (Please Print)* *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted Page 5 of 5 Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association.