Fever without Source in Infant
advertisement

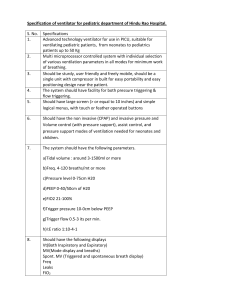
Santa Clara Valley Medical Center Inpatient Pediatric Wards/PICU Rotation Teaching Module Fever without a Source A 22-day-old term male infant presents to the ER with a chief complaint of fussiness and a 1-day history of poor feeding. He has only had 2 wet diapers today. He was born at 38 weeks to a 26 yo G1P1 woman by NSVD with a positive GBS screen. Rupture of membranes occurred 12 hours prior to birth, and mother was given 4 doses of ampicillin before delivery. On exam, his vitals are T 38.4 C, HR 190, RR 52, wt 4 kg. He is asleep in his mother's arms when you enter the room. You note some crusted dry mucus below his nose. Findings on physical exam are otherwise normal and his capillary refill time is less than 2 seconds centrally. Question 1: What is the approximate risk of a serious bacterial infection in this age group? A) 2% B) 12% C) 37% D) 48% Question 2: Which bacteria cause the majority of serious bacterial infections in infants under 29 days of age? A) GBS B) Strep. pneumoniae C) E. coli D) Listeria monocytogenes E) A, B, and C F) A, C, and D Question 3: What is the next recommended step in management? A) Thorough physical exam, then discharge home if well-appearing infant B) Physical exam, CBC, UA, then discharge home if normal C) Physical exam, CBC, UA, Blood culture, then discharge home after dose of ceftriaxone D) Admission for CBC, UA/Urine culture, and CSF panel/culture and antibiotics (Answers on following page) Suzanne Swanson Mendez, MD Answer to Question 1: B) 12% ("Fever without a Source in Children 0 to 36 Months of Age," by Dr. Ishimine. See full reference below). However, some studies have found the prevalence of SBI in this age group to range from 5-14%. Answer to Question 2: F) GBS, E. coli, and L. monocytogenes "Neonates are at a particularly high risk of SBI. The majority of febrile neonates presenting to the ED are diagnosed ultimately with a nonspecific viral illness, but approximately 12% of all febrile neonates presenting to a pediatric emergency department have serious bacterial illness. When they are infected, neonates are infected typically by more virulent bacteria (eg, Streptococci group B, E. coli, and Listeria monocytogenes) and are more likely to develop serious sequelae from viral infections (eg, HSV meningitis). Group B Streptococcus, a common bacterial pathogen in the age group, is associated with high rates of meningitis (39%), non-meningeal foci of infection (10%), and sepsis (7%). This age group is the least likely to be affected by the use of the pneumococcal vaccine because only a small percentage of neonates are infected by this pathogen. Although infection is uncommon, those neonates who are infected with Strep pneumoniae have a mortality rate of 14%. The most common bacterial infections in this age group are UTIs and occult bacteremia." (from "Fever without a Source in Children 0 to 36 Months of Age," by Dr. Ishimine. See full reference below). Answer to Question 3: D) Admission for CBC with differential, UA/Urine culture, and CSF panel/culture with antibiotics This is currently the standard recommended management for a febrile infant less than 29 days old and is the guideline that we tend to follow at Valley, however you may see a different practice in other settings. "Traditional risk-stratification strategies have used ancillary testing to supplement the limited information available from the history and physical exam. Unfortunately, it is difficult to predict accurately which neonates have invasive disease, even when laboratory testing is used....Chest radiographs are indicated only in the presence of respiratory symptoms, and stool analyses are indicated only in the presence of diarrhea." (from reference by Dr. Ishimine, as listed below). The different risk-stratification strategies include using the Rochester, Philadelphia, and Boston criteria. The peripheral wbc count has been used by many practitioners to determine whether to perform a lumbar puncture but does not have reliable predictability for meningitis in this age group. Serial Suzanne Swanson Mendez, MD CRP's can be helpful in ruling out sepsis in this age group but the initial CRP at the time of presentation may be falsely negative. (see Dr. Benitz reference). You initiate a sepsis evaluation that includes a CBC with differential, Blood culture, C-reactive protein, urinalysis/urine culture by urethral catheterization, and a lumbar puncture, and you arrange for admission for suspected sepsis. Question 4: Which antibiotics are recommended for treatment of suspected serious bacterial infection in this age group? A) Ampicillin and gentamicin B) Vancomycin and gentamicin C) Ampicillin and ceftriaxone D) Azithromycin (Answer on next page) Suzanne Swanson Mendez, MD Answer to Question 4: A) Ampicillin and gentamicin According to Dr. Ishimine’s article, "Because of the high rates of serious bacterial infections, all febrile neonates should receive antibiotics. Typically, these patients are treated with a third-generation cephalosporin or gentamicin. Ceftriaxone is not recommended for neonates who have jaundice because of the concern for inducing unconjugated hyperbilirubinemia. Other third-generation cephalosporins, such as cefotaxime, or gentamicin are used in this age group. Additionally, although the incidence of L monocytogenes is quite low, ampicillin is still recommended in the empiric treatment of these patients. Neonatal herpes simplex virus infections occur in approximately 1 per 3200 deliveries in the U.S. Neonates with HSV infections usually present within the first 2 weeks of life, and only a minority of infected children have fever. Rates of morbidity and mortality are high with neonatal HSV, but treatment with high-dose acyclovir improves outcomes in patients. Acyclovir is not recommended routinely for empiric treatment in addition to standard antibiotics in febrile infants but should be considered in febrile infants with risk factors for neonatal HSV. Risk factors include primary maternal infection, especially those infants delivered vaginally, prolonged rupture of membranes at delivery, the use of fetal scalp electrodes, skin, eye, or mouth lesions, seizures, and CSF pleocytosis.” “Febrile neonates should be hospitalized, regardless of the results of laboratory studies. Outpatient management of these patients has been suggested and occurs frequently when patients present to pediatricians' offices. However, given the lack of prospective studies addressing this approach as well as the limitations inherent in the screening evaluation in the emergency department and frequent difficulties in arranging follow-up evaluation, hospitalization is strongly recommended." (from "Fever without a Source in Children 0 to 36 Months of Age," by Dr. Ishimine. See full reference below). However, a recent meta-analysis suggests that some febrile infants, even those in the first month of life, might be able to be classified as “low-risk” and avoid antibiotic therapy: http://pediatrics.aappublications.org/cgi/content/abstract/125/2/228 Also, the question arises what to do when CSF cannot be obtained. For these cases, provided the infant is well-appearing and clinically stable, observation in the hospital without antibiotics can be a judicial management strategy. Suzanne Swanson Mendez, MD Question 5: The mother returns from picking up her other child from school and mentions that her 2-year-old also has a fever, runny nose, and cough at home. You send NP swabs for RSV, Influenza A and B PCR. The NP swab returns positive for RSV. How does this possibly change your management? A) A positive RSV test increases your suspicion for a urinary tract infection B) A positive RSV test increases your suspicion for meningitis C) A positive RSV test decreases your suspicion for bacteremia D) None of the above (Answer on next page) Suzanne Swanson Mendez, MD Answer to Question 5: D) None of the above In a prospective, cross-sectional study of over 1,200 infants aged 60 days or less, those testing positive for RSV had a rate of serious bacterial infections of 7.0% (SBI, as defined by either meningitis, bacteremia, UTI, or bacterial enteritis). This is in contrast to the RSV-negative group, which had a SBI rate of 12.5%. You can find the article here: http://pediatrics.aappublications.org/cgi/content/abstract/113/6/1728 The most common SBI in both groups of infants was a urinary tract infection, with 5.4% of the RSV-positive infants versus 10.1% of the RSV-negative infants being given the diagnosis of a UTI. The infants with a positive RSV test had a statistically significant decreased rate of UTIs, and also had lower rates of bacteremia and meningitis but these rates did not reach statistical significance. A study in 2009 of infants 60 days and younger with influenza also yielded similar results. http://pediatrics.aappublications.org/cgi/content/abstract/124/1/30 However, the question is how does this change our clinical management? (Also, the question also arises about how to define a UTI, but that's enough for a whole separate learning topic!) For the under 29 day old infant, the guidelines would suggest proceeding with a full septic workup and antibiotics. However, for the 29-60 day old infant, many practioners would only check a UA/urine culture and possibly a blood culture but forego the lumbar puncture, given the lower risk of bacteremia and meningitis, but this is an evolving topic. Please see the recent article in Pediatrics: "Performance of Low-Risk Criteria in the Evaluation of Young Infants with Fever: Review of the Literature" for more. http://pediatrics.aappublications.org/cgi/content/abstract/125/2/228 At Valley, if an infant is RSV-positive but otherwise well-appearing, we may choose to send the child home prior to 48 hours of culture growth, but the cultures need to be followed daily by our medical team until at least 48-72 hours of growth and the family must be reliable for follow-up. Of note, at Valley, blood cultures are continuously monitored by a machine and an alert sounds if bacterial growth is detected. For CSF and urine cultures, these are checked daily in the microbiology lab during the hours of 8am to 5pm. So if a CSF culture or urine culture is sent at 2am, you will not know if it's been negative for 24 hours until at least 8am (and often 10am) the day after admission. Sometimes this does alter our management, and it does bring up the question of the timing of growth on cultures. One recent article regarding central venous catheter infections noted that nearly all were positive by 36 hours, though this depended on bacterial type (Gram negatives vs. positives in particular): http://pediatrics.aappublications.org/cgi/content/abstract/121/1/135. Suzanne Swanson Mendez, MD Another article from the pre-Prevnar era with pediatric outpatients noted 95% of positive blood cultures were positive by 48 hours: http://pediatrics.aappublications.org/cgi/content/abstract/106/2/251. However, the amount of blood drawn from a younger infant is usually less than that drawn from older children or children with central venous catheters, which can result in falsely negative cultures. So, it does make sense to maintain caution when interpreting a negative blood culture result prior to 36-48 hours in this age group. Also, in the late spring and summer seasons, or if there is a history of enteroviral-like symptoms in the family (vomiting, headache, diarrhea), consider sending the CSF for an Enteroviral PCR. If this returns positive, it is unlikely that the infant has an SBI. References/Recommended Reading: Benitz WE et al, "Serial Serum C-Reactive Protein Levels in the Diagnosis of Neonatal Infection," Pediatrics 1998; 102; e41. (http://www.pediatrics.org/cgi/content/full/102/4/e41) Caviness AC et al, "The Prevalence of Neonatal Herpes Simplex Virus Infection Compared wtih Serious Bacterial Illness in Hospitalized Neonates," Journal of Pediatrics, vol. 153, no. 2, pp. 164-9. Ishimine P, "Fever Without Source in Children Ages 0 to 36 Months," Pediatric Clinics of North America, 53: 167-194, 2006. http://hsc.unm.edu/emermed/PED/physicians/residents/articles/Fever%20Wi thout%20a%20Source%20in%20Children%200%20to%2036%20Months%2 0of%20Age.pdf Huppler AR et al, "Performance of Low-Risk Criteria in the Evaluation of Young Infants with Fever: Review of the Literature," PEDIATRICS Vol. 125 No. 2 February 2010, pp. 228-233. http://pediatrics.aappublications.org/cgi/content/abstract/125/2/228 Suzanne Swanson Mendez, MD