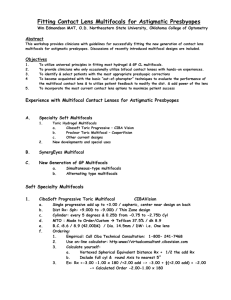
Maximize Success with the New Contact Lens Multifocals
advertisement

A. Using the New generation of multifocal contact lenses –> Simultaneous Vision 1. Acuvue Bifocal - Hydrogel bifocal - Vistakon 2. Focus Progressive - Hydrogel multifocal - CIBA Vision 3. Focus Dailies Progressive - Hydrogel multifocal - CIBA Vision 4. Frequency 55 Multifocal - Hydrogel multifocal - CooperVision B Maximize success in Presbyopic Fitting : 1. 2. 3. 4. 5. C. Pre-fitting evaluation a. Visual needs & Patient expectations Pre-fitting exam: a. Ocular health & Physical characteristics Protocol before recommending a lens modality or lens type a. Fine tune spectacle Rx b. Spherical monocular refraction c. Add plus until 20/30, balance, d. Reduce plus to most plus BVA (under normal “room” illumination) e. Evaluate Rx Pre-fitting conference with pt a Review findings & pt expectations b. Emphasize correcting presbyopia ( not fit this new bifocal) In this workshop you will develop a personal protocol or flow chart on which 5. Which lens to try first 2. How to use patient feedback to modify 3. What is the next alternative 4. What is the fall back correction Evaluating Spectacle Rx and astigmatism —> Maximize multifocal success 1. Selecting patients: Initial “flow chart” for maximum early success A. Significant Distance spherical spectacle Rx –> greater than +/- 1.00D 1. Yes ---------> RGP or Hydrogel multifocal 2. No ----------> Alternatives to multifocals: a. Multifocal in one eye only b Traditional Monovision or near lens only c. Distance contact lenses plus reading spectacles d. Other 2. Refractive cylinder: 1. 0.75D or less --------------------> Soft Multifocal or RGP Multifocal 2. 0.75D -2.50D ( due to corneal toricity ) ------------> RGP Multifocal 3. Other options: 3. Patient Feedback including Hx & requirements 1. Patient displeased with “Crispness” of vision with soft ---> RGP 2. Health issues with hydrogel lenses -----------------> RGP 3. Pt displeased with comfort of RGP’s ----------------> Soft 4. Part time wearer -------------------------------> Soft E. Alternatives multifocals Multifocal Multifocal Multifocal F. Lenses: Acuvue Bifocal 1. 2. Design: BIFOCAL with distance center 1. Five alternating distance and near zones 2. No intermediate without modification 3. Enhanced Bifocal Modification: a. Dominant Eye: Distance with Intermediate b. Non-dominant eye: Intermediate with near Parameters 1. Effective adds: +1.00, +1.50, +2.00, +2.50 2. Distance Rx: +6.00 to -9.00 3. Other: 8.5mm b.c. / 14.2 dia / UV blocker –> Two wk replacement : 6 pack Frequency 55 Multifocal: 1. 2. 3. 4. Three add powers, +1.50, +2.00, +2.50 Other parameters a. 8.7 dia. with a 14.4 dia / monthly replacement: 6 -pack b. +4.00 to -6.00 distance power ( use vertexed Sphere-cyl equiv. Power) Design: Center near aspheric multifocal for dominant (dist. enhnaced ) eye & center near aspheric multifocal for non-dominant ( near enhanced eye) For Rx’s a. between adds round down to lower add b. with sphero-cyl equivalent between to 0.25 powers -> more minus Focus Progressives & Focus Dailies Progressives: 1. 2. 3. Single progressive add up to +3.00 / Center near design One trial power designated on box for distance and wear Focus Progressives: A. B. C. 4. –---------------> Vifilcon A (group 4, 55%, dK 16) Two base curves: 8.6/8.9 with a 14.0 dia +6.00 to -7.00 distance Rx One month replacement ( option 2 weeks): available as 6 -pack Focus Dailies Progressives: -----------> nelfilcon (group 2, 69%, dK 26) A. B. C. Base curve: 8.6 with a 13.8 dia +5.00 to -6.00 distance Rx Daily replacement: available as 30 or 90 pack 5. Initial Focus Progressive lens selected from: a. Focus 1. 2. 3. 4. Progessive, “Initial Power Selection Table” Uses distance BVA spectacle Rx ( —> spherical equivalent) Table compensates for vertexes the sphero-cyl Rx to spectacle plane Spectacle add How good is the “Initial Power Selection Table “ ??? b. Or the use of the following Focus Progressive equation: Trial = Spherical Equivalent distance power plus 1/2 of the add power Example: Spectacle Rx: -3.00 dist / +1.50 add —> Trial = (-3.00 plus +0.75D) –> -2.25D ----------------------------------------------------------------------------- Selecting, Evaluating & modifying the Initial Lenses on the patient A. Selecting the distance power for the initial multifocal trial lens 1. Distance spectacle correction ------> Vertexed to corneal plane 2. Sphere only --------------------- RGP Multifocal & Sunsoft Additions 3. Sphero-cyl equivalent ------------- Focus Progressives and Acuvue Bifocal 4. Diagnostic distance lens power ® Make sure Exactly corneal plane Rx or more (+) 1. If more minus –> patient will use some of “add power” for distance B. Use Free lenses, Trial frame, or Flippers <-----------> Out of the Phoropter 1. 2. 3. 4. 5. 6. Normal “room” illumination ( Avoid mirrored rooms if possible ) Evaluate Binocularly -------->Maximum plus at distance i. Distance -----------> Initially use whole chart with 20/30 as bottom row ii. Near point materials---> use magazines or newspapers: 20/40 to 20/30 print “How do things look” Add trial lenses binocularly until you obtain the best balance between: Distance vision vs. near vision i. Add (+) O.U. ------------------->if clarity needed at near ii. Add (--) O.U. -------------------> to enhance distance vision Maximum plus to maximum acuity Motor activity: have patient walk out of exam room for feedback Problem Solving: Modification based on Patient Feedback A. “Cannot binocularly make distance sharp enough without losing near vision” 1. 2. Monocularly add minus to dominant eye, but do not occlude non-dominant eye while testing; typically -0.25D to -0.50D a. Both eyes still have a dist. And near Rx b. Enhance distance in one eye Frequency 55 and Acuvue a. Use the next lower add in the dominant eye b. Enhances distance clarity B. C. D. “Near vision not good, but distance isn’t bad” 1. Monocularly add plus to non-dominant eye a. Both eyes still have a dist. And near Rx b. “Enhanced” vision at near in non-dominant eye 2. Acuvue & Frequency 55 a. Monocularly use the next higher add in the non-dominant eye b. Enhances near Monocular addition 0.25 or 0.50 power typically all that is needed -> success vs failure Now what? 1. Insert final lenses to be dispensed a. Binocular acuity: for you and patient b. Monocular acuity: for medicao-legal documentation in chart 2. Reconfirm appropriate lens movement with slit-lamp 3. Patient education: Let the patient know a. You will be working with them to “fine tune” their Rx to meet problems and there may yet be lens changes b. There may be an adaption period (including slight shadowing of letters) c. Night driving, be cautious (halos around lights) 4. Return to office in 3 about days: 1. Long enough to evaluate vision / Short enough to prevent frustration 5. Use patient feedback modify