ACLS NOTES
advertisement

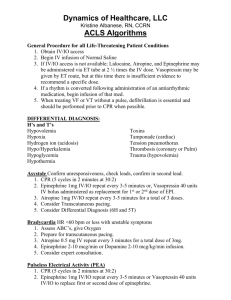
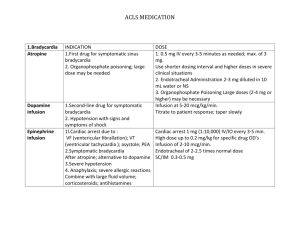
ACLS NOTES 8/9/10 Analyzing EKG: 1. are there P waves to every QRS cmplex 2. is rhythm regular or irregular, fast or slow 3. are waves Narrow/Atrial or Wide/Ventricular Pulseless VT: wide complex Asystole: Flat line, NO SHOCK PEA/pulseless electrical activity: No P wave, No T wave, no pulse, NO SHOCK 2nd degree Type 1/wiekenbach: PR interval changes/getting shorter, then drops QRS cmplex 2nd degree Type 2/mobitz: same PR interval, then drops QRS V.Tachy w/pulse: cardiovert, synch, charge, clear, fire SVT: Narrow complex, valsalva maneuver, give adenosine, CARDIOVERT V.Tachy: Wide complex, NO ADENOSINE Defibrillator Machine: Leads: White/RUQ, Black/LUQ, Red/LLQ (of chest) Monophasic AED: 360J Biphasic AED: 200J Cardiovert: Machine on, lead select, 50-100J, SYNCH, LOCKS ON R WAVE, Charge, ALL CLEAR/PUSH RED BUTTON Pt w/pulse: CARDIOVERT Pt w/o pulse: DEFIB Pace: 3rd degree, is most common/place pads Front to Back, bradyrhythm/symptomatic/ non responsive Pace: 30 bpm, set rate 76-80, select mili-amps 0-1-2-3-4, check heart rate, pt will get small shocks and will see spikes, NEEDS QRS to capture beat V.FIB AND PULSELESS V.TACHY------AED SHOCK ONLY 1st INDICATION FOR USE OF AED: 1. unconscious 2. not breathing 3. pulseless CPR: 30 compressions 2 breaths Rescue Breathing: 1 breath q 5-6sec Advanced airway: 1 breath q 6-8 sec and 100 compressions Anti-arrhythmic Drugs: Epinephrine or Vasopressin Lidocaine or Amiodarone in Cardiac Arrest, V.Tach, V.Fib EPINEPHRINE: IV/IO/ET, like adrenaline Indications: cardiac arrest, VF, pulseless VT, asystole, pulseless electrical activity/PEA 1mg (10ml 1:10,000 soln) q 3-5min NO MAX DOSE, Continue CPR---ONCE HAVE PULSE—STOP giving Endotracheal Tube: give 2-2.5mg diluted in 10ml NS Atropine Sulfate: IV/IO/ET, given after Epinephrine Indications: cardiac arrest, PEA, SYMPTOMATIC SINUS BRADY <60bpm, asystole 1mg q 3-5min, MAX 3 DOSES (3mg) Bradycardia: 0.5mg IV q 3-5 min, DO not exceed 0.04mg/kg (3mg) Endotracheal Tube: 2-3mg diluted in 10ml NS Treats----Organophosphate Poisoning-----Given in large dose 2-4mg Amiodarone: IV/IO, Treats life threatening arrhythmias that have not responded to other interventions (CPR, Shock, Vasopressin) Indications: RECURRENT V.FIB, Recurrent hemodynamically unstable V.Tachy 300mg PUSH, dilute in 20-30ml D5W Give 150mg ONCE IV PUSH, 3-5min. Recurrent Life threatening V.Arrhythmia: give 150mg q 10min, repeat 150mg q 10min prn 160 mg q 6hrs 540 mg q 18hrs Adenosine: short ½ life Indications: Treats PSVT >150-200bpm IV RAPID PUSH 1. 6mg 1-3sec, then 20ml NS flush, elevate arm 2. 12mg-----20ml NS, 1-2min 3. 12mg-----20ml NS, 1-2min MAX DOSE 30mg IF UNRESPONSIVE-------NEED CARDIOVERSIONLidocaine: IV/IO/ET 1-1.5mg/kg Indication: REFACTORY V.Fib 0.5-0.75mg/kg IV PUSH, repeat 5-10min, MAX 3 DOSES TOTAL 3mg/kg ET: 2-4mg/kg Vasopressin: IV/IO/ET Indications: REFACTORY V.FIB, asystole, PEA 40 UNITS 1 DOSE ONLY CAN REPLACE 1ST OR 2ND DOSE OF EPINEPHRINE Diltiazem: Acute Rate Control Indications: controls Vent. Rate in A. Fib, A. Flutter, Terminated re-entrant arrhythmia that requires AV nodal conduction 15-20mg (0.25mg/kg) IV over 2min May give other dose in 15min at 20-25mg (0.35mg/kg) over 2min USE AFTER ADENOSINE--------2ND LINE TREATMENT TO TREAT SVT Do not use with Ca+ channel blockers, or WPW syndrome, or w/Beta Blockers (drop Bp) Dopamine: 2nd line Tx for Symptomatic Bradycardia----after ATROPINE Indications: use in Hypotension, BP systole 70-100 w/signs of shock Can cause excess vasoconstriction IV: 2-20ug/kg per min, Titrate to pt response, taper slowly Precaution: correct hypovolemia, volume replacement Sodium Bicarbonate: Indications: treat hyperkalemia, bicarb acidosis (DKA, aspirin/TCA overdose, Cocaine, diphenyhydramine-OD) Not used in hypercarbic acidosis 1mEq/kg IV bolus Use ABG analysis to guide bicarb therapy ABG not reliable indicator of acidosis in Cardiac Arrest Example questions: Can be given ET: atropine, lidocaine, epinephrine, NO ADENOSINE Pt awake, alert, rapid heart beat, SVT-narrow, 172 HR, BP 108/69: Action=ADENOSINE 6mg Vasopressin Administer: can be given as 1st or 2nd dose of epinephrine (replaces administration of epinephrine) Pt w/CP, confused, sinus brady, 40bpm: ATROPINE, 0.5mg IV q 3-5min