Referral for Renal Specialist Outpatient Appointment
advertisement

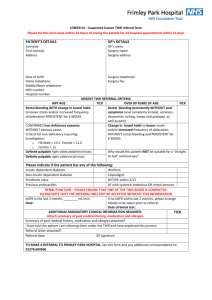
Request for Renal Specialist Outpatient Appointment Please complete referral letter overleaf. To move from one field to the next, please use the “tab” key HOSPITAL SPECIALTY / CLINIC Renal NAME OF SPECIALIST PREFERRED Has the patient previously been seen by this hospital? Yes No Has the patient previously been referred to the renal clinic / speciality Year Yes No PATIENT DETAILS Medical Record Number (if known) Please tick if applicable for this referral: DVA White DVA gold Medicare Number: Date of Birth: Ref No: / Male / Country of Birth: Marital Status: Number: Married Single Widow Female Aboriginal Torres Strait Islander Divorce Separated Surname: Previous surname First names: Preferred Name/Title Neither Defacto (i.e. maiden name): Address: Mailing Address (if different) Phone: home Work: Mobile: Next of Kin (Essential if under 18 years/guardian) SPECIAL NEEDS Relationship: If interpreter required, specify language & dialect First Name: Surname: Other special needs: Phone: Mobile: REFERRING DOCTOR LENGTH OF REFERRAL Name: 12 months Address: Other REFERRAL RECOMMENDATION This patient needs to be seen (please indicate Postcode: Routine Phone: Urgent Fax: or CPAC category 1,2, 3, 4, 5 (please indicate) USUAL GP: as above Other (see below) Have discussed with Registrar/Consultant) Name (if known) Name: Suburb: Appointment date given: (if applicable) Yes / No / 1of 2 Referral Letter for Renal Disease REASON FOR REFERRING (Please tick more than one if applicable from the list below) Immediate referral (Contact Renal Service via Hospital Switchboard) Malignant hypertension Hyperkalaemia (K>7.0mmol/l) eGFR <15ml/min Acute Renal Failure and Systemic Illness Urgent referral (Category 1 <30 days) Acute Nephrotic Syndrome (Proteinuria>300mg/mmol), oedema & low serum albumin Suspected systemic illness, eg SLE with renal involvement. Unexplained or Symptomatic eGFR 15–29ml/min Routine referral (Category 2 = 30 – 90 days) Suspected Glomerulonephritis: e.g Proteinuria/haematuria (urine PCR >100mg/mmol) eGFR 15–29ml/min (clinically well or known diagnosis) eGFR 30–59ml/min and: indigenous with diabetes* eGFR <60ml/min and eGFR decline >10% in 2 months* Anaemia (Hb <100g/l)* Abnormal potassium, calcium or phosphate* uncontrolled hypertension on 3 agents including a diuretic* Routine referral (Category 3 = 90 – 365 days) eGFR 30–59ml/min with >10% decline in 6 months Additional Diagnoses eGFR >60ml/min and suspected renal disease Other Conditions: o Diabetes mellitus: No Yes o Hypertension: No Yes o Cardiac disease No Yes o Peripheral vascular disease No Yes Smoking Status: Body Weight: Creatinine: eGFR Current medications: OTHER REASONS/COMMENTS for REFERRAL. Attach other information for eg drug allergies or reactions with patient’s name and DoB clearly printed : PLEASE ATTACH COPIES OF ALL CURRENT RELEVANT INVESTIGATIONS / REPORTS/ LETTERS Doctor’s Signature Provider Number Date 2of 2