choice of medical management based on symptoms and blood lead
advertisement

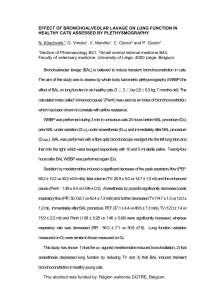
CHOICE OF MEDICAL MANAGEMENT BASED ON SYMPTOMS AND BLOOD LEAD CONCENTRATION Guidelines for the Detection and Management of Lead Poisoning for Physicians and Health Care Providers, Revised 1996 ASYMPTOMATIC CHILDREN (Before treatment, measure venous blood for lead) Clinical Presentation BLL 10 to 14 mcg/dL BLL 15 to 19 mcg/dL BLL 20 to 39 mcg/dL Treatment F Comments Pediatric evaluation Monitor blood lead levels 3-6 mo. Screen for iron deficiency anemia Provide counseling regarding appropriate nutrition and cleanlinessremoval of paint chips and dust. Pediatric evaluation Monitor blood lead levels at one month Screen for iron deficiency anemia Refer to local health department for environmental investigation and public Health Nurse Visit Provide counseling regarding appropriate nutrition and cleanliness— removal of paint chips and dust. Succimer BLL 40 to 69 mcg/dL Pediatric evaluation Monitor blood lead levels Screen for iron deficiency anemia Succimer: 10mg/kg/dose or 350 mg/m2/dose orally every 8 hours for 5 days. Reduce to 10 mg/kg/dose or 350 mg/m2/dose every 12 hours for an additional two weeks. Monitor liver function. Or CaNa2EDTA 1000 mg/m2/day Hospitalize when symptoms are present. >50 mcg/dL BLL >70 mcg/dL Pediatric evaluation Monitor blood lead levels Screen for iron deficiency anemia Hospitalization. Some clinicians use succimer. (FDA approved with blood lead levels >45 mcg/dL). Physicians should use clinical judgment or consult. Refer to local health department for environmental investigation and Public Health Nurse Visit. Provide counseling regarding appropriate nutrition and cleanlinessremoval of paint chips and dust. Succimer is preferred unless compliance requires use of CaNa2EDTA CaNa2EDTA for 5 days, preferably by continuous infusion, or in divided doses (through a heparin lock). Additional treatment may be needed depending on blood lead level rebound. A minimum of 2 weeks between courses is recommended unless more treatment is indicated. Refer to local health department for environmental investigation and Public Health Nurse Visit. Provide counseling regarding appropriate nutrition and cleanliness— removal of paint chips and dust. BAL 300 mg/m2/day and Start with BAL 50 mg/m2 IM every 4 hours. CaNa2EDTA 1000 mg/m2/day After 4 hours, start CaNa2EDTA 1000 mg/m2/day, preferably by continuous infusion, or in divided doses IV (through a heparin lock). Continue therapy with CaNa2EDTA for 5 days. BAL may be discontinued after 3 days if blood lead level <50 mcg/dL Additional treatment may be needed depending on blood lead level rebound. SYMPTOMATIC CHILDREN Acute encephalopathy Pediatric evaluation Screen for iron deficiency amenia Monitor blood lead levels Hospitalization. Refer to local health department for environmental investigation and public Health Nurse Visit. BAL 450 mg/m2/day and Start with BAL 75 mg/m2 IM every 4 hours. CaNa2EDTA 1500 mg/m2/day After 4 hours, start continuous infusion of CaNa2EDTA 1500 mg/m2/day. Provide counseling regarding appropriate nutrition and cleanlinessremoval of paint chips and dust. Continue therapy with BAL and CaNa2EDTA for 5 days. Interrupt therapy for 2 days. Treat for 5 additional days, including BAL if blood lead remains high. Other symptoms Pediatric evaluation Screen for iron deficiency anemia Monitor blood lead levels Other cycles may be needed depending on blood lead level rebound. Refer to local health department for environmental investigation and public Health Nurse Visit. Provide counseling regarding appropriate nutrition and cleanlinessremoval of paint chips and dust. BAL 300 mg/m2/day Start with BAL 50 mg/m2 IM every 4 hours. CaNa2EDTA 1000 mg/m2/day After 4 hours start CaNa2EDTA 1000 mg/m2/day, preferably by continuous infusion, or in divided doses IV (though a heparin lock). Continue therapy with CaNa2EDTA for 5 days. Discontinue BAL after 3 days if blood lead level <50 mcg/dL. Interrupt therapy for 2 days. Treat for 5 additional days, including BAL if blood lead remains high. Additional treatment may be needed depending on blood lead rebound. Adapted from Illinois Department of Public Health