SPWC_Text
advertisement

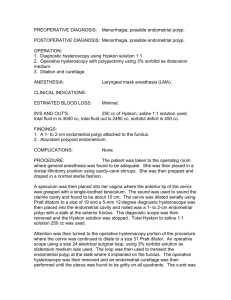
SURGICAL PATHOLOGY CONFERENCE Dr. Belur S. Bhagavan Case 1 (Slide 3069) History: 35 year old woman with a polyp in the body of the stomach. Image: http://pathology2.jhu.edu/jkronz/images/JMD_6-28-04_SPWC/Case_1/a1.jpg Multiple choices: a. Hyperplastic polyp b. Fundic gland polyp c. Intestinal metaplasia d. Adenomatous polyp Histology: This biopsy taken from the body of the stomach shows cystically dilated, tortuous and budding fundic glands lined by parietal cells, chief cells and mucous neck cells. There is focal apical “snouting” of the parietal cells suggestive of proton pump inhibitor therapy. The overlying epithelium is normal in appearance. No dysplasia is present. FUNDIC GLAND POLYP OF STOMACH: Fundic gland polyps (FGP), also known as Elster’s polyps, occur in the oxyntic mucosa both in the setting of familial adenomatous polyposis (FAP) syndrome as well as outside of it, but more commonly in the former setting. Spontaneous regression occurs. In the syndromatic setting, the patients are younger and most of them female. Variously regarded as hyperplastic, neoplastic and hamartomatous, these have no clinically significant malignant potential. There is some evidence to support a possible causal relationship between the use of Omeprazole, a proton pump inhibitor and development of FGP. FGP are usually small, less than 0.5 cm in size, sessile & smooth surfaced. They may be numerous and may carpet the mucosa. Hyperplastic expansions of the deep epithelial compartment of oxyntic mucosa with budding are represented in collections of assorted, distorted, cystically dilated oxyntic glands with overlying short pits. The cysts are of various shapes and sizes and are lined by oxyntic, chief and mucus neck cells. The overlying surface and foveloar epithelium may be atrophic, normal or dysplastic. When dysplasia occurs, it is usually low grade, rarely high grade and may be seen in both the syndromatic and non-syndromatic settings. Dysplasia is more common in the FAP associated FGP. FAP associated FGP have APC mutations where as sporadic FGP have beta catenin mutation. These observations suggest that these are indeed probable neoplasms, however, progression to carcinoma is vanishingly rare. FGP are not regarded as premalignant lesions of clinical significance. Case 2 (Slide 3070) History: 40 year old man with a 2.5 cm polyp in the colon. Image: http://pathology2.jhu.edu/jkronz/images/JMD_6-28-04_SPWC/Case_2/a1.jpg Multiple choices: a. Hyperplastic polyp b. Tubular adenoma c. Juvenile polyp d. Peutz-Jegher’s polyp e. Changes consistent with mucosal prolapse Histology: This large polyp shows mature and differentiated colonic epithelium overlying arborizing fascicles of smooth muscle seen in the lamina propria. There are elongated, branching and dilated crypts containing abundant inspissated mucus and intramucosal hemorrhage which obscures the lamina propria smooth muscle at low power. The epithelium is focally proliferative and shows reparative changes in areas adjacent to a superficial erosion. Small benign, entrapped glands are seen in cross-section in the center of the specimen. Dysplasia is absent. PEUTZ-JEGHER’S POLYP OF COLON: Peutz-Jegher’s (PJ) polyps of colon contain a mature colonic epithelium that drapes underlying arborizing proliferations of smooth muscle from the muscularis mucosae. PJ polyps of other gastrointestinal locations are made up of mature mucosa native to the segment in which they occur. PJ polyps occur in both the syndromatic and non-syndromatic settings and in both situations they may be solitary or multiple. Colonic PJ polyps show normal, elongated or branching crypts and the surface may have a villous architecture. While all of the native cell types may be present, goblet cells may predominate. Surface erosion, granulation tissue and regenerative changes are common. Epithelial pseudoinvasion, cystic dilatation of crypts, mucinous extravasates, inflammatory changes and calcification may occur in the deeper portions of the polyps and may be mistaken for infiltrating carcinoma. Adenomatous foci (dysplastic foci) and carcinoma may develop in the setting of PJ polyp. Case 3 (Slide 3072) History: 30 year old male with a polyp in the sigmoid colon. Image: http://pathology2.jhu.edu/jkronz/images/JMD_6-28-04_SPWC/Case_3/a1.jpg Multiple choices: a. Inflammatory (pseudo-) polyp b. Mucosal changes consistent with mucosal prolapse c. Chronic inflammatory bowel disease d. Juvenile polyp e. Hamartomatous polyp Histology: At low power one observes a fragment of colonic epithelium with pronounced crypt elongation and architechtural distortion. At higher power, one notes Paneth cell metaplasia and focal surface erosion. The stromal inflammatory infiltrate has prominent eosinophils and neutrophils. Reactive epithelial changes, but no dysplastic changes are present. Given the endoscopic appearance, the findings are consistent with an inflammatory polyp. INFLAMMATORY (PSEUDO-) POLYP OF COLON: Inflammatory polyp (IP) of the colon, also known as inflammatory pseudopolyp (a misnomer and an oxymoron since the term “polyp” only connotes any mass that protrudes into the lumen of a hollow viscus) describes a non-neoplastic residual mucosal island commonly seen in idiopathic inflammatory bowel disease (IBD). They may also be seen in amebiasis, schistosomiasis, ischemic colitis, anastomotic sites and adjacent to ulcers. The IP is composed of inflamed and often regenerative colonic mucosa left in situ when an ulcero-inflammatory process destroys the surrounding mucosa. Often solitary, frequently they are multiple. Rarely, these polyps may carpet the entire mucosa. The polyp itself is composed of distorted and dilated crypts, a stroma that is often edematous and containing assorted inflammatory cells, smooth muscle fascicles and atypical stromal cells. These atypical stromal cells may be mistaken for malignant cells and caution should be exercised in not over interpreting them. The crypt epithelium is often reactive and may simulate adenomatous epithelium. Although dysplastic changes may be seen in the epithelium, the polyps are not regarded as preneoplastic and have no malignant potential. When dysplastic changes are noted, it is important to biopsy and study the surrounding mucosa for similar changes. In small lesions and small endoscopic biopsies, it may not be possible to differentiate or exclude other polyps such as juvenile polyp, Cowden’s polyp and hamartomatous polyps. The biopsy interpretation in such instances must be made with caution and in the proper clinical context. Case 4 (Slide 3071) History: 45 year old female with a rectal polyp and a history of constipation. Image: http://pathology2.jhu.edu/jkronz/images/JMD_6-28-04_SPWC/Case_4/a1.jpg Multiple choices: a. Chronic inflammatory bowel disease b. Mucosal prolapse polyp (solitary rectal ulcer syndrome) c. Ischemic colitis d. Peutz-Jegher’s polyp Histology: At low power this colonic mucosal biopsy specimen shows obvious crypt architectural distortion (some crypts showing a distinctive “diamond” configuration in cross section) and alteration of the lamina propria. At higher power, one notes a superficial erosion with underlying vascular ectasia and congestion in the lamina propria. The lamina propria is fibrotic with wisps of smooth muscle ingrowth from the muscularis mucosae across the entire biopsy specimen. The muscle, however, conspicuously lacks an “arborizing” pattern. MUCOSAL PROLAPSE POLYP (SOLITARY RECTAL ULCER SYNDROME) OF RECTUM: Mucosal prolapse polyp of rectum is commonly known as solitary rectal ulcer/solitary rectal ulcer syndrome (SRUS). Mucosal prolapse of the rectum is associated with varied gross macromorphology, which includes solitary ulcer, multiple ulcers, a diffuse erythematous colitic (proctitic) appearance, bullous edema, mucosal polyp/s, submucosal soft to firm mass/masses and stricture. Since historically and by usage the term solitary rectal ulcer syndrome is entrenched in the literature it is important to emphasize that this lesion is neither solitary nor is it always an ulcer. Furthermore, these lesions are not restricted to the rectum. They occur in different parts of the gastrointestinal tract and are disguised under many different terms depending on their site and gross appearance. It is now well recognized that the common etiologic and pathogenetic mechanism of SRUS is mucosal proplapse with superimposed ischemia mediated changes. Micromorphologically, the features are distinctive and diagnostic. The mucosa is inflamed, eroded/ulcerated. The crypts are elongated, hyperplastic and may show moderate to severe reactive changes which might raise a concern for dysplastic changes. There is vascular ectasia, congestion and hemorrhage. The lamina propria is often condensed, fibrotic and shows ingrowth of smooth muscle from the muscularis mucosae. Associated with this fibromuscular obliteration of the lamina propria there may be proliferation of fine fibrillar elastotic tissue around crypts. The cross sectional and oblique profiles of the crypts often appear diamond shaped. In long standing cases, there may be down growth of the benign mucosal epithelium into the submucosa. Here, the crypts might rupture forming mucus pools. There may be superimposed calcification. Localized colitis cystica profunda aptly describes these changes and are part of the spectrum of mucosal prolapse changes. Case 5 (Slide 3068) History: 35 year old female with epigastric pain. Biopsy taken from the antrum of the stomach. Image: http://pathology2.jhu.edu/jkronz/images/JMD_6-28-04_SPWC/Case_5/a1.jpg Multiple choices: a. Gastrointestinal stromal tumor b. Eosinophilic gastroenteritis c. Inflammatory pseudotumor d. Inflammatory fibroid polyp e. Erosive helicobacter pylori gastritis Histology: This biopsy specimen from the antrum of the stomach at low magnification shows a poorly circumscribed fibroinflammatory lesion centered in the lamina propria which splays apart fibers of the muscularis mucosae to involve the submucosa. There is overlying mucosal erosion. At higher power, the lesion is variably cellular and composed of plump to elongated spindle cells in a myxoid stromal background which contains a mixed inflammatory infiltrate with prominent eosinophils. There is focal germinal center formation. The spindled stromal cells and eosinophils form characteristic concentric rings around large and small blood vessels when seen in cross section. INFLAMMATORY FIBROID POLYP OF STOMACH: Inflammatory fibroid polyp (IFP), described by Vanek in 1949 is a mesenchymal reactive tumifactive process involving the GI tract. The exact nature and etiology remain elusive and controversial but many issues relating to their diagnosis and differential diagnosis have been clarified. The stomach, antrum in particular, is the most common site of involvement but they also occur in the small and large intestine and very rarely in the esophagus. It is more common in females and can occur at all ages. The IFP especially in the stomach is poorly circumscribed, infiltrative and centered in the submucosa but may impinge on the mucosa and tunica muscularis. The ileal IFP tends to be a bit more circumscribed and polypoid. Complications include ulceration, bleeding and intussusception. This non-neoplastic tumor is composed of proliferating spindle cells in a loose myxoid vascular stroma admixed with assorted inflammatory cells such as plasma cells, lymphocytes, histiocytes and a generous sprinkling of eosinophils. In the majority of the lesions, the spindle cells show a loose concentric arrangement (onion skinning) around blood vessels and glands. In a small subset of these lesions this arrangement is not seen. This and other observations have lead to the speculation that there may be two different lesions included under the term inflammatory fibroid polyp. The spindle cells are positive for CD34 (negative in those tumors lacking concentric onion skinning) in the majority of cases, as is vimentin. Some histiocytic markers are also positive in some cases. The lesions are negative for muscle and neural markers. CD 117 is consistently negative. Genetically no substitution, deletion, insertion occur in c-kit exon 11 or c-kit exon 9. A diffuse positivity for fascin and focal positivity for CD35 in 10 cases has suggested a dendritic cell phenotypic differentiation. Distinction should be made of IFP from other reactive, neoplastic and quasineoplastic spindle cell mass lesions such as granulation tissue, eosinophilic gastroenteritis, gastrointestinal stromal tumor, inflammatory pseudotumors (inflammatory myofibroblastic tumors also known as plasma cell granuloma), benign fibroblastic polyps, solitary fibrous tumor, hemangioendothelioma and hemangiopericytoma. This differential diagnosis may be particularly challenging in small endoscopic mucosal biopsies from the GI tract.