Supplemental Digital Content 2: Supplemental Methods and Results
advertisement

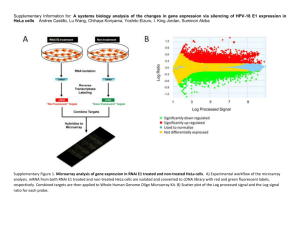
Supplemental Digital Content 2: Supplemental Methods and Results Methods Collection of biopsy tissue samples Needle-core protocol biopsies were obtained using an automated biopsy gun with an 18-gauge needle, under ultrasound guidance. Routine diagnostic tissue samples were taken along with a separate core of renal cortex which was immediately placed in RNAlater (Ambion Inc, Austin, TX) and stored at –80°C until RNA extraction and subsequent microarray analysis. RNA extraction and microarrays Total RNA was extracted from each biopsy using TRIzol Reagent (Invitrogen, Carlsbad, CA) as per manufactures protocol, and measured for RNA integrity using the RNA 6000 Nano LabChip ® Kit (Agilent Technologies, Waldbronn, Germany) on a 2100 Bioanalyzer (Agilent Technologies, Waldbronn, Germany). Total-RNA suitable for use is defined by a RNA integrity number exceeding 7 [1, 2]. 100ng of quality total-RNA from each extracted biopsy was amplified, via first reverse transcription into cDNA followed by amplification; then labeled with Biotin using the OvationTM Biotin System (NuGEN Technologies, San Carlos, CA), following the manufactures instructions. The cDNA fragments from the various individual protocol biopsies were hybridized onto Affymetrix GeneChip® Human Genome U133 Plus 2.0 Arrays comprising more than 54,000 probe sets, covering 38,500 well-characterized human genes (Affymetrix Inc., Santa Clara, CA). The microarrays were scanned using the GeneChip Scanner 3000 (Affymetrix Inc., Santa Clara, CA) on predefined settings. Microarray and pathway analysis The microarrays were normalized and analyzed using the latest versions of R (2.11.1) statistical computing environment [3] and Bioconductor 2.6 [4] incorporating the main analysis packages of affy [5], GCRMA [6] and samr [7], along with additional add-on packages for data visualization and processing. In addition, the Excel based significant analysis of Microarrays 1 (SAM) analysis packages were used in the focused analyses, CAI vs. no-CAI at each time point in an un-paired comparison. Genes were ranked based upon their false discovery rates (FDR) and Q-values, which were set to 10% for differential expression. Differentially expressed gene lists were interrogated using DAVID [8], SOURCE [9], GeneCards® [10], (Ingenuity® Systems, Redwood City, CA) and Entrez PubMed [11]. The gene expression output from EMT related differentially expressed genes, was subject to hierarchical clustering using Spearman’s correlation and average correlation matrix (Cluster 3.0) and results visualized as a heat map (TreeView 1.60). Statistical analysis Normalized gene expression values obtained from the transplant biopsies for each EMT gene of interest were analyzed against the various histological scores using a Spearman’s Rank correlation in GraphPad Prism 5 (GraphPad software Inc., La Jolla, CA), which was also used to generate Forest plots. Odds ratios were calculated using logistic regression for the presence of CAI with SAS [12]. Correlations between gene expression and pathology were performed in a categorical fashion with each time point independent from the other, with the pathology score at each time point versus the gene expression of each gene. Only correlations ≥0.4 with a Pvalue <0.05 were considered viable and significant to be further used in the analysis. EMT associated gene enrichment in CAI associated genes was assessed using hypergeometric analysis via a Chi Squared test with a Yates correction in GraphPad Prism 5 (GraphPad software Inc.). A probability of less than 0.05 was considered significant for all statistical analyses. All values are expressed as mean±standard deviation unless specified. Post-hoc probabilities are presented for microarray analyses. Results Enrichment analysis of EMT associated genes Using the differentially expressed gene findings from the previously published paper on chronic allograft injury (767 DEGs) [13], we performed an enrichment analysis for EMT associated genes 2 (243 genes) [14], using the Chi squared test with Yates correction. Performing an intersection analysis we observed 13 out of the 243 EMT associated genes were present in the CAI differentially expressed list of 767 genes. This gave a significant two tailed P-value (P=0.005) from a Chi squared analysis, thus indicating enrichment for EMT in CAI (Table 1). Table 1: Chi squared analysis of EMT gene enrichment in CAI Study CAI associated genes (Naesens et al., [13]) EMT associated genes (Vitalone et al., [14]) Total Total genes 33000 243 33243 DEG genes 767 13 780 Total 33767 256 34023 Chi Squared, with Yates correction (P=0.005) QPCR validation of MMP2 at 3mo post-transplant QPCR was performed on an independent cohort of 12 patients on their 3mo protocol biopsy to validate the significantly differentially expressed gene MMP2 (q score in the microarray data set of 5.39, and a false discovery rate of <5%), recognized to play a role in EMT, using one house keeping gene (GAPD) as an endogenous control. The expression of MMP2 in each phenotype (CAI and no-CAI) was determined then and corrected against GAPD and expressed as a ratio of fold change of CAI/no-CAI, which is the same comparison as performed in the microarray analysis. We observed that MMP2 was up-regulated in CAI compared to no-CAI by 1.3 fold. As this gene was also seen to be up-regulated from the microarray analysis, thus validating the expression seen on the arrays. Table 2: Comparative fold change of MMP2 in 3mo biopsies with CAI MMP2 Fold change Arrays 2.9 Fold change QPCR 1.3 Decreased E-cadherin staining (CDH1) in CAI patients 3 We observed a significant decrease in the number of CDH1 positive only cells in the tubules of biopsies with CAI compared to no-CAI biopsies (P=0.04, 132.9±38.6 vs. 161.4±16.4, per HPF respectively) as seen in composite Figure 1. The decrease in CDH1 staining can be considered a reflection of tubular injury and tubular epithelial cell loss, which is the first stage of the EMT mechanism and a measure of EMT. Figure 1: Increased number of E-cadherin (CDH1) stained cells (black arrows) in noCAI (A) versus CAI (B) as indicated by positive cells per high powered field (C, mean±SEM). HPF= high powered field, SEM= standard error of the mean. 4 References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. Fleige, S. and M.W. Pfaffl, RNA integrity and the effect on the real-time qRT-PCR performance. Mol Aspects Med, 2006. 27(2-3): p. 126-39. Schroeder, A., et al., The RIN: an RNA integrity number for assigning integrity values to RNA measurements. BMC Mol Biol, 2006. 7: p. 3. R Development Core Team, R: A language and environment for statistical computing. R. F. f. S. Computing. 2007. Bioconductor. 2011; Available from: http://www.bioconductor.org. Bolstad, B.M., et al., A comparison of normalization methods for high density oligonucleotide array data based on variance and bias. Bioinformatics, 2003. 19(2): p. 185-93. Jean(ZHIJIN) Wu, R.I., James MacDonald, Jeff Gentry GCRMA (2.22.0). Tusher, V.G., R. Tibshirani, and G. Chu, Significance analysis of microarrays applied to the ionizing radiation response. Proc Natl Acad Sci U S A, 2001. 98(9): p. 5116-21. Dennis, G., Jr., et al., DAVID: Database for Annotation, Visualization, and Integrated Discovery. Genome Biol, 2003. 4(5): p. P3. Diehn, M., et al., SOURCE: a unified genomic resource of functional annotations, ontologies, and gene expression data. Nucleic Acids Res, 2003. 31(1): p. 219-23. Rebhan, M., et al., GeneCards: integrating information about genes, proteins and diseases. Trends Genet, 1997. 13(4): p. 163. NCBI NLM NIH. SAS, SAS® 9.1.2 Qualification Tools User's Guide. 2004: SAS Institute Inc., Cary, NC. Naesens, M., et al., Microarray expression profiling associates progressive histological damage of renal allografts with innate and adaptive immunity. Kidney International, 2011. In Press. Vitalone, M.J., et al., Epithelial-to-mesenchymal transition in early transplant tubulointerstitial damage. J Am Soc Nephrol, 2008. 19(8): p. 1571-83. 5