Demonstrating the style for the Journal of Physics
advertisement

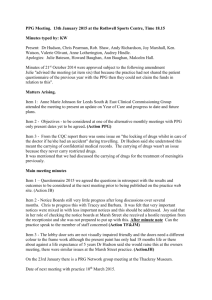
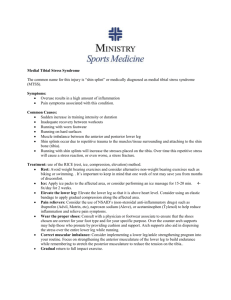
Non-invasive photoplethysmography to assess lower limb peripheral perfusion with selected postural changes Jia Zheng1 Sijung Hu1, Shangzhi Xin2, Vincent P Crabtree1, Peter R Smith1 1 Department of Electronic and Electrical Engineering, Loughborough University, Ashby Road, Loughborough, Leicestershire LE11 3TU, UK 2 College of Electrical Engineering, University of Shanghai for Science and Technology, 516 Jun Gong Road, Shanghai 200093 P.R. China E-mail: j.zheng@lboro.ac.uk Abstract. A custom dual probe photoplethysmography (PPG) system was developed to investigate the effect of passive leg raising on blood volume change in the lower limb during supine and 45 degree reclining functional test. Two infra Red (905nm) optoelectronic probes were attached to the second toes of subjects during lab trials. The AC and DC components of PPG signals were collected from a ‘before and after’ passive leg raising study, with support platform heights of 10cm to 60cm. Thirteen healthy normotensive subjects (age: 23±3, gender: M/F 9/4) participated in this study. PPG signals were simultaneously recorded from both the raised and stationary legs. Platform heights in the range of 10cm to 30cm produced AC amplitude that significantly decreased (p<0.001) while the DC value had a significant change (p<0.05) with subjects supine. The AC amplitude marginally increased, then significantly decreased (p<0.05) between the heights of 30cm and 60cm, with the subject reclining, while the DC value considerably increased between the heights of 10cm to 30cm. The signals from the stationary leg showed similar, but smaller responses. These results demonstrate local and systemic physiological phenomenon in the lower limb peripheral vasculature with postural changes. Disturbances in these phenomena could be indicative of pathology, such as vascular disease. A PPG based optoelectronic system could deliver an effective tool for non-invasive, low-cost, fast and simply assessment of these pathologies. 1. Introduction Photoplethysmography (PPG) is a non-invasive optical technique for detecting blood volume changes in tissues [1], and is ideally suited for the assessment of peripheral circulation. The fundament of PPG technology is the optical detection of the dynamic cardiovascular pulsewave, generated by the heart, as it travels throughout the body. Pulse waves obtained from the PPG signal can deliver clinically valuable information about peripheral vascular perfusion. In our study, a custom dual probe PPG system was developed to investigate lower limb peripheral vascular perfusion. The illumination extends up to several mm deep into tissue, and hence a true assessment of the microcirculation is made [2]. The autoregulatory system is sensitive to arterial blood volume variations during postural functional tests which stimulate the vascular physiology to respond. Assessment of any compensatory responses could indicate if vascular pathology is present. 2. Method 2.1. Measurement system A custom dual probe photoplethysmography (PPG) system was assembled using the DISCO4 multi-channel PPG system (Dialog Devices Ltd, UK). The system employed a NIDAQ USB6015 (National Instruments Co. USA) Data acquisition system, which is 16 bit quantisation resolution, each channel sampled at 128 times per second. The PPG AC signal was obtained from the detector output using an analogue low band-pass filter with the cut-off frequency of 0.75Hz and 11Hz. The toe probes are Dolphin 3311V (Nellcor compatible) transmission mode pulse oximetry probes (Dolphin Medical, UK), with wavelength 905nm, at approximately 2mW optical power. An EN60601 (XP power, plc.) medical approved power supply feeds the system. The system was controlled with a custom program, written in LabView (National Instruments Co. USA), operating on a standard battery powered Pentium Laptop PC. 2.2. Protocol Thirteen healthy, normotensive subjects (median 23 years, range 20-26 and gender M/F 9/4) participated in our study. The subjects rested for at least 5 minutes in a supine position on a measurement couch before having their pulse rate, systolic and diastolic blood pressures taken. All the measurements were taken in a warm temperature-controlled room (24±2°C). The ambient light in the room were turned off during the measurement. The subjects were asked to breathe naturally and stay still for the trial time. It was ensured that both legs were placed in a comfortable position in order to keep the toes relatively motionless for stable and repeatable recording. Two transmission mode PPG sensors were lightly taped to on the second toes of both of feet to reduce probe movement artifacts [3]. During the first stage, a recording was made in the supine position. In successive recordings, the right leg was passively raised and supported on sponge blocks to individual heights ranging from 10cm to 60cm for 3 times, whilst the left leg remained in the original, still position. Recording were taken for 10s at each height. After a further 5 minute rest, the subject was requested to recline on a 45 degree sponger block. The process was then repeated in an identical manner as the supine position. The protocol is shown in Figure 1. Figure 1 Schematic diagram to represent laboratory trial protocol with supine and 45 degree reclining recording positions Sequence of passive leg raising in supine position a 10s b (different height) 10s 5 min rest Sequence of passive leg raising in reclining 45degree position a 10s 10s Two sensors are attached onto both feet to gather PPG signals when wh right leg is passively raised and left leg is remaining in still 2.3. Data analysis The PPG AC and DC signals gather from the trial were analyzed using Matlab (The Math Work Inc. USA). Firstly the pulse-to-pulse AC amplitude was calculated, and then the mean AC amplitude was derived for each subject. The mean DC value was calculated by averaging over each 10s recording, as the DC signal is relatively constant over a short period. For individual postural trial heights, the mean of the AC amplitude and the DC value were calculated by averaging mean AC amplitude and DC value over all thirteen subjects. The mean of AC amplitude and DC value for each leg raise period was then normalized by dividing with the mean from the non-raised position Box-and-whisker plots were used to illustrate statistical groupings, and the Paired Student t-test was used to determine the statistical significance of changes. A p < 0.05 was considered statistically significant. 3. Results 3.1. AC amplitude with passively leg raising The Box and whisker plots of the normalized AC amplitude are shown in Figure 2, recorded over passive leg raising from heights of 10cm to 60cm. With the subject in a supine position and the right leg is passively raised, the AC amplitude shows a decreasing trend with increasing height - the decrease is statistically significant for heights from 10cm to 30cm (p<0.001). With the subject in a 45 degree reclining position and their right leg is passively raised, the AC amplitude firstly increased and then decrease, with statistically significant changes in the height range between 30cm and 60cm (p<0.001). For the left, stationary leg, the change tendency is similar but not as pronounced as the right passively raised leg. Figure 2 The position normalized AC amplitude versus the individual height of passive right leg raising in the form of box-and-whisker plot Supine posture 45 degree reclining posture 2.0 2.0 p=0.02 p=0.22 p<0.001 1.5 p=0.10 Right foot 1.5 p<0.02 0.5 1.0 p=0.15 0.5 p=0.001 p=0.10 p=0.004 p<0.001 0.0 0.0 10 20 30 40 50 60 10 20 30 40 50 60 2.0 2.0 p=0.08 1.5 p=0.04 p=0.43 p=0.38 1.5 p=0.02 p=0.04 p=0.01 Left foot Normalized amplitude, a.u. p<0.001 1.0 1.0 1.0 p=0.08 0.5 p=0.01 0.5 p=0.005 0.0 0.0 10 20 30 40 Height, cm (a) 50 60 10 20 30 40 50 60 Height, cm (b) 3.2. DC value with passive leg raising The Box and whisker plots of the normalized DC values are shown in Figure 3, recorded over passive leg raising from heights of 10cm to 60cm. The DC value from both feet showed an increasing tendency with these two selected postures. There is a statistically significant change in the normalized DC value from the height of 10 cm to 20 cm (p<0.05) in the supine position while passively raising the right foot, and a significant change in the 45 degree reclining position from heights of 10 cm to 30 cm (p<0.001). The change in the normalized DC value in the left foot is statistically significant between the height of 10 cm and 30 cm (p<0.05) when in the supine position, and is also statistically significant between the heights of 10 cm and 40 cm (p<0.05) with the subject in a 45 degree reclining position. Figure 3 The position normalized DC value versus the individual height of passive right leg raising in the form of box-and-whisker plot Supine posture 45 degree reclining posture 1.2 1.2 p=0.01 p=0.08 p<0.001 Right foot p=0.01 1.1 p=0.05 p=0.38 p=0.13 1.0 1.0 p=0.06 p=0.12 p=0.001 p=0.003 p<0.001 0.9 0.9 10 20 30 40 50 10 60 20 30 40 50 60 1.2 1.2 p=0.003 p=0.17 p=0.04 p=0.07 1.1 1.1 p=0.03 p=0.50 Left foot Normalized amplitude, a.u. 1.1 p=0.008 p<0.001 p=0.60 1.0 1.0 p=0.10 p=0.02 p=0.03 0.9 0.9 10 20 30 40 Height, cm (a) 50 60 10 20 30 40 50 60 Height, cm (b) 4. Conclusions With passively leg raising in the postural positions of supine and the 45 degree reclining, the normalized AC amplitude and DC value response similarly in both feet, indicating that a central mechanism is involved. The greater response in the normalized AC amplitude and DC value after the right leg raising than in the left leg keeping in still suggests that, in addition to the role played by a central mechanism, a local control mechanism produced a much greater effect in posture vasomotor response [4]. 5. References [1] Hertzman A B 1938 The blood supply of various skin areas as estimated by the photoelectric plethysmography AM. J. Physiol. 124 329-340. [2] Incze A, Lazar I, Abraham E, Copotoiu M, Cotoi S (2003) The use of light reflection rheography in diagnosing venous disease and arterial microcirculation Rom J Intern Med. 41 35-40. [3] X F Teng and Y T Zhang 2004 The effect of contacting force on photoplethysmographic signals Physiol. Means. 25 1323-1335. [4] Ahmad A K Hassan and J.E. Tooke 1988 Mechanism of the postural vasoconstrictor response in the human foot Clinical Science 75 379-387.