Syracuse Family Dental Clinic
advertisement

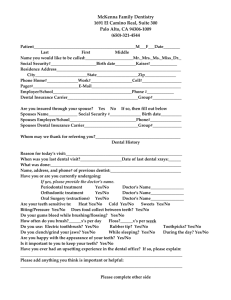
Syracuse Family Dental Clinic LLC Dr. Michael L. Gailey, DDS, MS Today’s Date: ________________ Patient Name: ____________________________________ Medical Physician’s Name: ____________________ Gender: M F Date of Birth: __________ Although dental personnel primarily treat the area in and around your mouth, your mouth is a part of your entire body. Health problems that you may have, or medication that you may be taking, could have an important interrelationship with the dentistry you will receive. Thank you for answering the following questions. Are you under a physician’s care now? Yes No If yes, explain ______________________________ Have you ever been hospitalized or had a major operation? Yes No If yes, explain__________________________________________________________________________ Have you ever had a serious head or neck injury? Yes No If yes, explain__________________________________________________________________________ Are you taking any medications, pill, or drugs? Yes No If yes, explain ________________________ Are you currently taking medication for or have you been diagnosed with osteoporosis? Yes No Do you use tobacco? Yes No Are you on a special diet? Yes No Do you use controlled substances? Yes No WOMEN: Are you: Pregnant/trying to get pregnant? Nursing? Taking oral contraceptives? Are you allergic to any of the following? Aspirin Penicillin Codeine Acrylic Metal Latex Local anesthetics Other _____________________ Do you have or have you had any of the following? AIDS/HIV Positive Alzheimer’s Disease Anaphylaxis Anemia Angina Arthritis/Gout Artificial Heart Valve* Artificial Joint* Asthma Blood Disease Blood Transfusion Breathing Problem Bruise Easily Cancer Chemotherapy Chest Pains Cold Sores/Fever Blisters Congenital Heart Disorder Convulsions Cortisone Medicine Diabetes Drug Addiction Easily Winded Emphysema Epilepsy or Seizures Excessive Bleeding Excessive Thirst Fainting Spells/Dizziness Frequent Cough Frequent Diarrhea Frequent Headaches Genital Herpes Glaucoma Hay Fever Heart Attack/Failure Heart Murmur* Heart Pace Maker* Heart Trouble/Disease Hemophilia Renal Dialysis Hepatitis A Rheumatic Fever* Hepatitis B or C Rheumatism Herpes Scarlet Fever High Blood Pressure Shingles Hives or Rash Sickle Cell Disease Hypoglycemia Sinus Trouble Irregular Heartbeat Spina Bifida Kidney Problems Stomach/Intestinal Disease Leukemia Stroke Liver Disease Swelling of Limbs Low Blood Pressure Thyroid Disease Lung Disease Tonsilitis Mitral Valve Prolapse* Tuberculosis Pain in Jaw Joints Tumors or Growths Parathyroid Disease Ulcers Psychiatric Care Venereal Disease Radiation Treatments Yellow Jaundice Recent Weight Loss *Condition may require medication Have you ever had any serious illness not listed above? Yes No N/A _________________ Comments:_____________________________________________________________________________ ______________________________________________________________________________________ I authorize Syracuse Family Dental Clinic LLC and /or such associates or assistants as designated to perform those procedures as may be deemed necessary or advisable to maintain my dental health or the dental health of any minor or other individual for which I have responsibility including arrangement and/or other pharmaceutical agent(s), including those related to restorative, palliative, therapeutic or surgical treatments. I understand that the administration of local anesthetic may cause an untoward reaction or side effects, which may include, but are not limited to bruising, hematoma, cardiac stimulation, temporary or rarely, permanent numbness, and muscle soreness. I understand that occasionally needles break and may require surgical retrieval. I understand that as a part of dental treatment, including preventive procedures such as cleaning and basic dentistry, including fillings of all types, teeth may remain sensitive or even possibly quite painful both during and after completion of treatment. Gums and surrounding tissues may also be sensitive or painful during and/or after treatment. I voluntarily assume any and all possible risks, including the risk of substantial and serious harm, if any, which may be associated with general preventative and operative treatment procedures in hopes of obtaining the potential desired results, which may or may not be achieved, for my benefit or the benefit of my minor child or ward. I acknowledge that the nature and purpose of the foregoing procedures have been explained to me if necessary and I have been given the opportunity to ask questions. Signature:______________________________________________Date:___________________________ (Patient, legal guardian or authorized agent of patient) Witness:_______________________________________________Date:____________________________