Oesophageal Doppler
advertisement

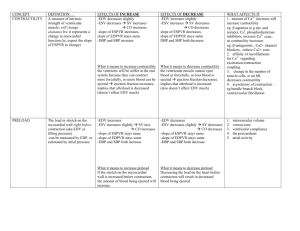
Oesophageal Doppler 30/11/10 OHOA pages 984-986 FANZCA Part II Notes USES - non-invasive cardiac output monitor DESCRIPTION - measures velocity of blood in descending aorta and calculates SV and Q - its uses a nomogram based on age, weight and height to estimate aortic diameter (some models measure aortic root diameter using TOE) Contra-indications - IABP severe coarctation known pharyngo-oesophageal pathology severe bleeding Indications - major surgery with large fluid/blood shifts - high risk patients - haemodynamic instability Jeremy Fernando (2010) METHOD OF INSERTION AND/OR USE - lubricate probe well - insert probe into oesophagus via nose or mouth - turn volume up initially (sharpest sound = best position) - input age, height and weight - insert probe to 35-40cm from teeth (T5/6) - manipulate probe until characteristic Doppler signal found (well defined triangle with black centre surrounded by red with white in trailing edge) = distribution of RBC velocities @ a given point in time - adjust cycle length (5 = good starting point), gain (to decrease ambient noise, start @ 5 also) - the brighter (whiter) the colour the greater the number of RBCs travelling at the given velocity - it is a dynamic monitor so needs refocusing prior to each reading INFORMATION - Q = SV x HR - SV dependent on preload, afterload and contractility Jeremy Fernando (2010) - Q estimated by minute distance SV measured by stroke distance x aortic root diameter preload measured by FTc afterload measured by interpretation of FTc and PV contractility measured by PV - Corrected systolic flow Time (FTc) (s) – indexed to preload, normal = 0.33-0.36s, - Peak velocity (cm/sec) – indexed to contractility, age related, (20yrs 90-120 cm/sec, 90 yrs 30-60 cm/sec) - Minute distance (cm) - stroke distance (AUC) x HR, linear cardiac output parameter, distance moved by a column of blood through aorta in 1 minute (<800cm = low flow state, >1200cm = high flow state) Actions from readings (need to be interpreted in clinical context) - low low low low SV -> fluid FTc -> fluid PV -> inotrope PV + low FTc -> decrease afterload COMPLICATIONS/DISADVANTAGES - bleeding perforation ulceration stricture formation learning curve (significant inter and intra-observer variability) probe displacement requiring repositioning Jeremy Fernando (2010)