A&T Nigeria Summary and Problem Statement
advertisement

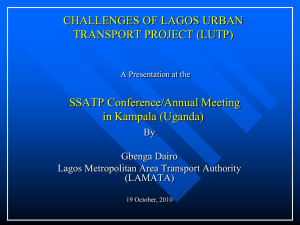
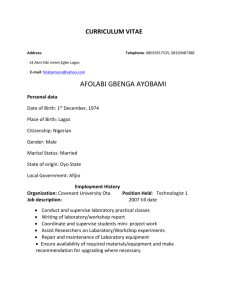
A&T Nigeria: Summary and problem statement 1. Executive Summary Every year, millions of children die and many more fail to realize their full potential because of undernutrition in the critical 1,000 day period. Nigeria is home to about 7% of the world's sub-optimally breastfed children and ranks second in countries with high mortality due to sub-optimal feeding. Progress in reducing undernutrition has been hampered by a number of challenges (many of which are not unique to nutrition, but rather are systemic and are operational issues that affect numerous sectors) but unprecedented political attention to undernutrition over the last few years has created a critical window of opportunity in Nigeria. We believe this investment has the potential to lower deaths attributable to sub-optimal breastfeeding through implementation of Alive & Thrive’s (A&T) proven approach, drawing on experience and lessons learned from the program’s first phase. Because of the size and complexity of Nigeria, the program is proposed to focus on two states, Lagos and Kaduna, with national level advocacy. All four components from A&T’s framework will be applied in the states: (1) advocacy and policy; (2) interpersonal communication and social mobilization; (3) mass communication; and (4) strategic use of data. The primary learning question for the evaluation in Nigeria will be: Can implementation of the four component framework in Nigeria have an impact on infant and young child feeding (IYCF) behaviors similar to what was observed in Phase I A&T countries? The primary outcomes to be measured will be IYCF practices in the two states where A&T will be implementing all four components—Lagos and Kaduna. The outcomes are related to the WHO-recommendations for optimal breastfeeding and complementary feeding practices for children under 24 months of age. These will include, but may not be limited to: increases in early initiation of breastfeeding (within one hour of birth), increases in exclusive breastfeeding, and increases in minimum diet diversity and minimum meal frequency among children 6-23 months. These will be the primary outcomes of two of the key A&T components: interpersonal communication and community mobilization and mass communication. A&T experiences in other countries have shown that a model that incorporates advocacy for pro-IYCF policies and strategic use of data are effective at achieving the behavioral outcomes listed above due to their positive impact on supportive social norms. Additional outcomes expected from these two components include: improved implementation of IYCF-friendly policies and increased use of data to support IYCF programs and policy. 2. Problem Statement Infant mortality, stunting/wasting, and IYCF Nigeria, the most populous country in Africa with 178.5 million people,1 has some of the world’s lowest maternal and child health indicators. In the last five years, moreover, rates of improvement slowed and the country barely reached the half-way mark toward its 2015 MDG targets. According to the most recent Nigeria Demographic and Health Survey (NDHS-2013),2 under-5 mortality was 128 deaths per 1,000 live births and infant mortality was 69. The neonatal mortality rate hardly changed in the preceding five years, dropping from 41 to 37 deaths per 1,000 live births. The maternal mortality ratio also remained high at 560 per 100,000 live births. Nutrition indicators have shown a similar pattern of stagnation. The exclusive breastfeeding rate for 0-6 month olds—a practice that can significantly reduce child deaths—has remained unchanged since 1999 at an astounding 17%. Stunting among children under 5, high at 37% nationwide, dropped 3 percentage points over the previous 5 years. But the rate of wasting actually rose— from 14% to 18%. Table 1 shows basic nutrition indicators for children 0-23 months in Nigeria nationally and for the two priority program states of Lagos and Kaduna by richest and poorest socioeconomic status (SES) quintiles. 3 The data highlight the distribution of population by wealth in the two states (strongly reflecting the urban vs. rural population divides). The data also highlight the extreme nutritional deficiencies prevalent particularly in Kaduna across wealth quintiles, and the presence of high wasting even among the urban rich in Lagos. 1 World Bank data. Available at: http://data.worldbank.org/country/nigeria National Population commission [Nigeria] and ICF Interntaional (2014). Nigeria Demographic and Health Survey 2013. Aguja, Nigeria, and Rockville, MD, USA: NCP and ICF International. (Henceforth NDHS 2013) 3 USAID has been conducting a review of data quality (especially anthropometry) in the NDHS 2013. At project outset, A&T will consider any issues/implications related to this review and will conduct its own anthropometric survey to establish baseline measures for the project areas. 2 Table 1: Nutritional status of children < 2 year in the richest and poorest* quintiles, nationally and by region (NDHS 2013)+ Indicator National Poorest – richest Lagos Poorest – richest Kaduna-Urban Poorest – richest Kaduna-Rural Poorest – richest Stunting (% < -2SD) Severe stunting (% < -3SD) Wasting (% <-2SD) Severe Wasting (% < -3SD) 48 – 14 29 – 6 19 – 13 6–3 N/A – 9 N/A – 1 N/A – 17 N/A – 3 N/A – 60 N/A – 39 N/A – 33 N/A – 18 53 – N/A 39 – N/A 44 – N/A 19 – N/A *Note: Wealth quintiles were calculated based on the national sample. In Lagos, the survey identified no women into the two bottom quintiles. In urban Kaduna, the survey identified no women in the poorest quintile. In rural Kaduna, the survery identified women in the richest (top) quintile. Some of the very wide variation in status among these sites may be a function of the way the index was identified and warrants study. + The NDHS survey did not focus specifically on children aged 0-2 and the sample for this subgroup is small. See also footnote (3) on possible issues refarding anthropoetric data quality. Undernutrition undermines the health and development benefits of country investments. The Foundation 2015-2020 strategy notes: Millions of children die and many more fail to realize their full potential because of undernutrition in the critical 1,000 day period between their mother’s pregnancy and their second birthday. Malnutrition is responsible for nearly half of all underfive child deaths each year. Children who miss out on good nutrition during these 1,000 days never achieve full physical or mental growth, limiting their ability to learn in school and reducing their productivity as adults. IYCF interventions focus on preventing undernutrition in the 1,000 day window of opportunity. However, causes of undernutrition may be multi-sectoral and, similarly, no single strategy is likely to bring about large-scale change. Determinants may range from basic food security, to wealth and social status, to access to services, to maternal education, to broad-based social norms and cultural beliefs and family practices. The two priority states for this program—Lagos and Kaduna—offer an opportunity to investigate determinants and plan program strategies A banker: “It is just not feasible to exclusively breastfeed for large populations (10.7 million and 7.3 million respectively) with for six months. Is it that easy? Well, I’d like to do it, if I distinct urban and rural differences (Lagos state is mostly urban) and don’t have to work. Our workplaces are strictly for other variations (such as predominant ethnic and religious groups) business, not for nursing mothers. If you still need your that to some degree reflect the enormous diversity of the country. job, you’ll not take your baby into a bank.” On pumping According to WHO guidelines, the level of severe wasting in rural milk: “The milk easily sours and besides, it is better for Kaduna may also require a fundamental difference in emphasis on the baby to suck directly from the source than be fed supplementation vs. prevention. (See Section 3. Scope and Approach with a bottle. So, at two months, I had to stop exclusive for further on the state-level rationale). breastfeeding – using infant formula along with breast milk when I’m available.“ Why breastfeeding is becoming unpopular, by mothers Wole Oyebade, The Guardian (newspaper), August 12, 2013 The current status of IYCF practices to be addressed by A&T Priority nutrition practices for children under 2 years of age include timely initiation of breastfeeding (BF), exclusive BF up to age 6 months, introduction of complementary foods (CF) around 6-8 months of age with appropriate frequency of meals and diversity of food groups, and continued BF up to two years. Given the close tracking of urban and rural residence with SES status in the two priority states, one would expect poorer practices in rural areas—but this is not consistently the case. For example, Table 2 shows that in the two states, timely initiation of BF was lowest in largely urban Lagos (only 19%) compared to Kaduna (U-39%, R-35%). Continued BF for children 12-24 months was also lowest in Lagos (75%) compared to Kaduna (U-78%, R-92%). However, generally in 2013, IYCF practices were poor in both of the priority states. Giving pre-lacteals within the first 3 days was common (Lagos-42%; Kaduna/U-60%, R-66%). The majority of babies received plain water. Further, receiving water was a norm for infants of all ages. Even during the first month of life, most infants nationwide (54%) were given water in addition to breastmilk. By 4-5 months, only 10% of infants nationwide received breastmilk with no additional liquids. The belief that infants require water is the chief reason for the low exclusive BF rate among infants 0-6 months in the priority states (Lagos-37%; Kaduna/U-19%, R-7%). 2 Table 2: Nutrition-related indicators for Nigeria (national), Lagos, and Kaduna (NDHS 2013) Indicator Nigeria Lagos Timely initiation of BF (<1 hr) *Prelacteal given during the first 3 days Exclusive BF (<6 mo) Exclusive BF at 4-5 mos Timely introduction of CF (6-8 mo) *Early introduction of CF (4-5 mo) Minimum meal frequency of CF (6-23 mo) Dietary Diversity (> 4 groups) of CF (6-23 mo) Minimum acceptable diet (6-23 mo) Continued BF at 12-15 mos *Infant formula (0-6 mos) *Bottle feeding (0< 23 mo) 33 60 17 10 64 38 60 19 10 78 6 16 19 42 37 20 67 24 46 11 3 75 12 27 Urban Kaduna 39 60 19 18 86 40 93 29 24 78 8 20 Rural Kaduna 35 66 7 0 80 54 85 10 8 92 7 13 *These four indicators show percent practicing harmful behaviors; other indicators are for positive behaviors. Bottle feeding is a particularly dangerous practice and the NDHS 2013 notes that the trend is increasing. In Lagos, 27% of all children under 2 were bottle fed the previous day. Acceptability of the practice is particularly evident when data are disaggregated by age: in Lagos, 42% of children 6-11 months were bottle fed and in urban Kaduna, 39% of children 0-5 months were bottle fed. Giving infant formula is less common but still worrisome, especially in Lagos (12%). Nigerian infants are typically introduced to complementary foods both too early and too late. According to the NDHS 2013, introduction of solid or semi-solid foods between 4-5 months was especially prevalent in Kaduna (U-40%, R-54%) but also common in Lagos (24%). At the same time, only 64% of children nationwide were introduced to complementary foods “on time” (between 6-8 months). Timely introduction was lower in Lagos (67%) vs. Kaduna (U-86%, R-80%). The quality and frequency of foods given varies greatly. Nationally in 2013 only 10% of children 0-23 months received a minimum acceptable diet (Lagos-3%, Kaduna U-24%, R-8%). Poor dietary diversity was the biggest factor; only 11% of children in Lagos received the recommended four or more food groups, compared to Kaduna (U-29%, R-10%). Minimum meal frequency was particularly problematic in Lagos (only 46% of children) compared to Kaduna (U-93%, R-85%). See infant feeding practices by age in urban Lagos and rural Kaduna in the figures on the next page. Figure 1 (a) and (b): Infant feeding practices by age (in months) in urban Lagos and rural Kaduna (NDHS 2013) (b) Rural Kaduna (a) Urban Lagos 100% 100% 80% 80% 60% 60% 40% 40% 20% 20% 0% 0% 0-1 2-3 4-5 0-1 3 2-3 4-5 Potential determinants of IYCF practices (social and public health context) Policies, services, social norms, and various household characteristics may all be important determinants of the key IYCF practices. Ineffective implementation of the International Code of Marking of Breastmilk Substitutes (BMS) and lack of a policy on maternal workplace protection (Convention 183) are major issues for Nigeria. An even greater problem has been the lack of improvement over time in basic maternal and child health services. Table 3 (following page) shows that in 2013, nationwide coverage of services was two or more times higher in urban areas than in rural areas. Notably, 66% of urban women had skilled attendance at birth, compared to only 23% of rural women. This is a crucial service not only to ensure survival of both mother and baby, but to assist with BF initiation. In contrast, prevalence of a postnatal visit within two days of delivery was high everywhere. This contact is also an important opportunity to help the mother establish exclusive BF. (In rural Kaduna, 46% of visits were by traditional birth attendants [TBAs] and their skill levels may vary.) Basic coverage and reach problems are also common for child health services. In 2013, care-seeking for child diarrhea (which can be a valuable window for changing IYCF practices) was low in Lagos (42%) and even lower in Kaduna (12%). Table 3: Health service indicators for Nigeria (national), Lagos, and Kaduna (NDHS 2013) Indicator Nigeria (urban/rural) 52 38 (67/23) 94 28 (35/26) Four or more ANC visits Skilled attendance at birth Postnatal visit (<2 days) Care-seeking for child diarrhea (0-23 mo) Lagos 97 87 94 42 Urban Kaduna 60 55 99 Rural Kaduna 34 20 96 12 Countdown 20154 emphasizes the challenge for Nigeria in achieving SES equity in services. Those in the two richest quintiles benefit from up to four times better coverage of MNCH services than those in the lowest two quintiles. Moreover, this imbalance is often greater than the basic urban/rural split. Nationwide, only around 10% of the poorest women have skilled attendance at birth and only around 20% have 4 ANC visits. Improving practices through face-to-face counseling will be a challenge given the low use of services by those who are most vulnerable. Other determinants play less certain roles in IYCF practices and their effects need to be studied. Table 4 provides more information on different household characteristics that may influence practices. (See also, section “3. Scope and Approach”) Table 4: Maternal/household characteristics and preferences, Lagos, and Kaduna (NDHS 2013) 4 Indicator Lagos Urban Kaduna Rural Kaduna Religious identification Christian 57%, Muslim 33% Ethnic identification Place of giving birth (public facility/private/home) Maternal literacy Weekly media access by women Household ownership of mobile phone Yoruba 58%, Igbo 20% Public = 21%, Private = 57% Home = 22% 81% Radio = 60%, TV =73% Muslim 66%, Christian 21% (more Muslim in rural areas) Hausa 54%, Fulani 8% Public = 47%, Private =7% Home = 56% 50% Radio = 39%, TV = 43% Publ.=19%, Priv.=1% Home=80% 19% Radio=26%,TV=16% 97% 91% 63% Available at: http://www.countdown2015mnch.org/country-profiles/Nigeria 4 Given reliance on private providers even by the poorest groups (for maternal delivery but also for advice on common illnesses) engaging this sector will be an important strategy. Religious institutions may be powerful channels for reaching even the “hard to reach” in all areas. In Lagos and Kaduna, the potential of mass media is uncertain before considering factors such as wealth and maternal education. In rural areas, where only 26% of women listen to the radio weekly, use of mass media will be particularly challenging. Although a high percentage of households reported having a mobile phone, access by women is not well known. (Nationally, male ownership is predominant).5 A&T’s Theory of Change To address these challenges and issues described in the Problem Statement, A&T developed a Theory of Change, which underpins our approach to work in Nigeria and describes the links between the individual barriers and chosen strategies, approaches, and likely impact. Figure 2: A&T Theory of Change If we address these barriers… Inadequate resources and priority given to IYCF interventions in MNCH Few health care service contacts during child’s first 2 years Inadequate knowledge, skills, and motivation of frontline health workers to support IYCF Poor families face food insecurity Lack of social support for recommended IYCF practices among family members, community leaders, frontline health workers Lack of large-scale interventions to shift social norms, beliefs, and IYCF behaviors Cultural misperceptions and traditional practices (e.g., giving water) in with these strategies…….. then we can achieve….. Targeted advocacy & technical support at national and State levels Improved contacts with mothers at 0-24 months for BF/CF counseling (facility-, community-, homebased) Health care provider (public, private, NGO) orientation, training, and performance improvement in IPC Identification of foods available even in food insecure households Social mobilization through Ward Dev. Committees, religious associations, NGO programs Mass and traditional media and mobile phone communication to reach multiple audiences and address relevant beliefs and misperceptions Data collection/use to improve interventions and policies Additional IYCF resources from States and other stakeholders Guidelines issued by State Ministers of Health to prioritize IYCF in all health services Mothers supported during pregnancy, at delivery, and up to 2 years to feed as recommended Health workers achieve high coverage & quality Perception among foodinsecure families that recommendations are feasible Communities enlightened to support priority IYCF behaviors Widespread perception that recommended IYCF practices are the norm 5 IMPACT Increase in IYCF practices: early initiation of breastfeeding, exclusive breastfeeding, minimum dietary diversity, minimum meal frequency Increase in newborn and infant lives saved Improved child health, growth, and development Broadcasting Board of Governors, Gallup (2014). Contemporary Media Use in Nigeria. Available at: http://www.bbg.gov/wpcontent/media/2014/05/Nigeria-PPT-FINAL.pdf 5