Karissa Felix - Hidden Briar Wellness
advertisement

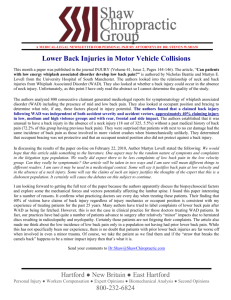
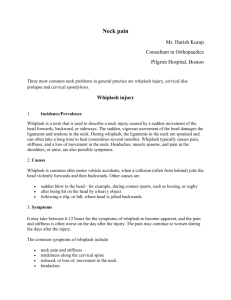
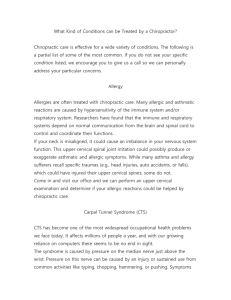
The Effectiveness of Myofascial Release, Joint Mobilizations and Trigger Point Therapy on Chronic Whiplash Associated Disorder Karissa Felix 2nd Year Massage Therapy Student at OVCMT karissafelix@live.com Abstract The purpose of this case report was to determine the effectiveness of Myofascial Release, Joint Mobilization and Trigger point therapy on individuals suffering from chronic whiplash associated disorder (WAD). Whiplash is a neck injury due to forceful, rapid back-and-forth movement of the neck. It most often occurs during a rear-end auto accident, but the injury can also result from a sports accident, physical abuse or other trauma. This study hypothesizes that using the massage therapy techniques mentioned previously are effective modalities in increasing range of motion (ROM) and decreasing pain and headaches in patients with chronic WAD. This is a single subject case study done over the course of 7 weeks on a 1 hour a week basis. The subject is a 24 year old female who has been suffering from chronic WAD for 6 years after being involved in a motor vehicle accident. She complains of consistent, throbbing headaches and decreased motion in her cervical spine. Assessments were done every treatment and included AROM of the cervical spine, postural scans and subjective information on pain and headaches. At the end of these treatments the results showed an increase in pain free cervical spine AROM and a decrease in neck and headache pain from 8/10 to 4/10. Headaches were also reported as having decreased in reoccurrence as well from 5x/wk. to 3x/wk. The study supports the hypothesis that the use of myofascial release, joint mobilization and trigger point therapy are effective modalities in treating chronic WAD. Keyword List “Whiplash Associated Disorder” “Massage Therapy” “Post-Traumatic Headache Disorder” “Neck Pain” “Myofascial release” “Joint Mobilizations” “Trigger point therapy” Introduction Whiplash is an injury to the cervical spine and surrounding tissues caused by a forceful, rapid back-and-forth movement of the neck. It most often occurs during a rear-end auto accident, but it can also be a result from sports accidents, physical abuse or other trauma (Mayo Clinic, 2015). Common signs and symptoms in a patient suffering from whiplash include; neck pain, muscle stiffness, decreased range of motion in the cervical spine and headaches or migraines (Rattray, 2000). Most people with whiplash recover within a few months after a course of pain medication, exercise and manual therapies. Some people, though, experience chronic neck pain and other ongoing complications for a much longer period of time.(Mayo Clinic, 2015) A whiplash injury is classified as chronic if a patients’ symptoms extend beyond 6 months.(Norton et al., 2013). In order to assess the severity of each individual whiplash case the Quebec Task Force created a guideline in 2001 for classification of WAD into 4 different stages. These stages range in severity from a patient experiencing no complaints of neck pain to experiencing neck pain associated with vertebral fractures and dislocations (Rattray, 2000). WAD injuries have the possibility of creating lesions in most of the structures within the neck and in severe cases are assessed for the potential of fractures and dislocations in the cervical spine. WAD injuries typically involve the most of the muscles, ligaments, joints and nervous tissues of the neck,but can also extend into the shoulders and back due to the body’s response of guarding and repairing the damaged structures.(Elesko, 2014) The muscles which often experience the most damage include; the sternocleidomastoids, scalenes group, trapezius and longus coli muscles. Muscular strain injuries may also be seen in the suboccipitals, intrinsic spinal muscles, cervical erector spinae, levator scapulae, rectus capitis anterior, longus capitis, platysma and the supra and infrahyoid muscles (Rattray , 2000.) The joints most commonly affected by whiplash are the facet joints of the cervical spine and the intervertebral joints and discs, possibly resulting in avulsion fractures. Damage may occur along the thoracic spine, or to the shoulder girdle, and these are also common referral patterns for cervical spine lesions. It is important to note that patients with chronic WAD may have multiple injuries stemming from one common traumatic event (Elesko, 2014). Due to the many differences each patient may present with treatment for whiplash is dependent on the severity of the injury and can range from manual therapy to surgical intervention. In most cases a doctor will prescribe pain medication, possibly a neck brace for a few days and referral of the patient to a physiotherapist, chiropractor and/or registered massage therapist (RMT) may be given. When treating whiplash as an RMT the main focus is to restore a patients pain free ROM, decrease matured adhesions in the soft tissue around the neck and maintain joint health in the cervical, and possibly thoracic, spine (Rattray, 2000). Various technique such as; Swedish Massage, Deep Tissue Massage, Trigger point therapy, Myofascial release, Joint mobilizations, Therapeutic Exercise, Range of Motion and Neuromuscular Therapy among others have been found to be effective in doing this (Sutton, 2014) For this Case Report I have decided to focus on using Myofascial release, Trigger point therapy and Joint mobilizations as my modalities. I have found these modalities to be effective in treating various whiplash patients in the past and various papers and studies done by Elesko (2014), Buckland (2013) Norton (2013) and Sutton (2014) support this concept. I’ve also chosen these techniques, in part, because they are less invasive and less aggressive then techniques such as Neuromuscular Therapy and Swedish Deep Tissue which I feel is important when treating someone suffering from chronic pain. I hypothesize that these techniques; Myofascial release, Trigger point therapy and Joint Mobilizations, will also be effective in treating chronic WAD by decreasing the occurrences of headaches and increasing overall ROM. Myofascial Release (MFR) is a hands-on technique that involves applying gentle sustained pressure into the myofascial connective tissue in the direction of resistance. This technique is used to break up adhesions and promote unrestricted blood and lymph flow in these tissues. The definition of fascia includes all the tissues that are traditionally designated as ‘fascia’ in human anatomy as well as tendons, ligaments and bursae (Myers, 2015). When the fascial system sustains severe trauma, such as whiplash, fascia modifies the mesh of its fibers becoming more rigid and plastic than fluid and elastic; the result being that it becomes denser and the collagen fibers in its matrix align irregularly (Buckland, 2013). The use of MFR in this case study will aid in returning the fascial fibers of the deep cervical fascia to their original flexibility and fluidity. Once the fascial fibers have been realigned there should be an increase in the available ROM of the cervical spine and a decrease in tension in the cervical muscles. Trigger points are hyperirritable spots within a taut band of skeletal muscle or fascia. They are tender to touch, exhibit predictable pain referral patterns and cause shortening of affected muscles (Rattray, 2000.) They are a common disorder in even healthy individuals and can be debilitating in nature, leading to secondary conditions such as tension headaches and visceral discomfort due to their referral patterns. There are various way of treating trigger points from deep muscle stripping and skin rolling to prolonged or alternating ischemic compressions, all of which have shown to be equally effective (Rattray, 2000). The treatment of trigger points in this case study will help to realign muscle fibers and restore muscle length. This will lead to a decrease in pain and reoccurrence of headaches. Joint mobilizations are skilled passive manual therapy techniques applied to joints and related soft tissues at varying speeds and amplitudes. Speed and amplitude can range from small amplitude force at a high velocity to large amplitude and low velocity. These techniques are applied on a continuum in order to improve joint heath, increase ROM and decrease pain in a joint.(Dixon, 2003) When a joint has a dysfunction the muscles and tissue surrounding the joint work to create stability around the unstable area, this leads to hypertonicity, adhesion formation, trigger points and pain in the region. By restoring proper joint alignment and function there will be a decrease in tension in the surrounding muscles and an increase in ROM for the patient. Hypothesis Over the course of 7 weeks, on a 1 hour per week basis, I hypothesize that using Myofascial Techniques combined with Joint Mobilizations and Trigger point therapy will help to decrease the occurrences of headaches and increase the available pain free ROM in patients suffering from chronic WAD. Assessment For assessments during this treatment I took ROM measurements of the cervical spine pre and post each massage, in which all ranges were recorded. I did a full postural assessment before each treatment to examine how various muscles and joints were adapting to the massages. Subjective information regarding pain experienced pre and post massage, was recorded based upon a pain scale from 1-10 that was established and explained to the patient at the first session (1 representing a light touch and 10 representing the worst pain the patient has experienced). I also did various special tests throughout the course of the treatments in order to help isolate areas of irritation, hypertonic muscles and trigger points. The special tests I did that showed a positive result were: Spurling’s compression test was positive for muscle spasm on the left while the head was extended and rotated left, Hautant’s Test was positive for minor vertebral artery compression on the left and muscle testing for upper trapezius and levator scapula muscles showed positive results bilaterally for weakness and muscle spasm, indicating a presence of trigger points in those muscles. Through palpation of various muscles I was able to discover the presence of moderate to severe trigger points in both left and right levator scapula muscles at the insertion on the superior angle of the scapula. I recorded all my findings, subjective and objective, in order to compare any changes in the patient throughout the durations of the treatments. Subject Case History The patient in this study is a 24 year old female, suffering from chronic WAD. She was in a MVA in 2009 in which she was hit from the rear into oncoming traffic and then consecutively hit from the front causing severe whiplash. She saw a physiotherapist for a few months postaccident but stopped her treatments due to financial reasons. The physiotherapist gave her exercises for her shoulders and neck and she felt they only exacerbated her symptoms and thus she stopped doing them shortly after her last visit to the physiotherapist. Currently she suffers from frequent headaches which she explains as radiating from her occiput in a “headband style” around the posterior, lateral and anterior portions of her head. When given a scale from 1-10 she rated her headaches as between 7-10/10 on an almost consistent basis. Accompanying these headaches are symptoms such as dizziness, nausea and decreased ROM. She is currently working in the behavioral development program at OSNS. Her job entails work with special needs children and involves varying amounts of stress and noise which can, and frequently do, exacerbate her headaches. She is also a very active individual and trains at the gym 3-5x week, depending on her condition, doing various weight training and cardio exercises in order to keep herself physically healthy. She is hoping that these treatments will help her with decreasing her headaches and increasing her ROM, as well as she hopes to learn ways to manage her headaches and pain without the use of pharmaceuticals. Treatment The patient was initially treated with a 1 hour relaxation massage to assess her tissue and her tolerance for massage. After this initial session we continued with 6 more consecutive treatments on a one hour basis, one week apart. She complied with my request to not take any pain medication within 4 hours of each treatment so assessment findings would not be affected. The specific treatment goals during these massages were as follows; to increase the pain-free ROM of the cervical spine in all ranges using passive ROM and joint mobilization techniques, to decrease the patients headaches by way of releasing the trigger points in the sub occipital and levator scapula muscles, and to educate the patient on natural pain management techniques to help her with her headaches when she was out between treatments. The techniques used during each treatment were myofascial release to start, progressing to Trigger Point Therapy and then ending with Joint Mobilizations, the time used for each technique varied depending on the patient’s signs and symptoms each session. The Myofascial techniques used were limited to shaping, spreading, cutting and cross hands technique and were used on the upper traps, levator scapula, scalenes and sternocleidomastoid bilaterally. Trigger points were found in the levator scapula and sub occipital muscles and were dealt with in various ways, depending on their presentation, with focus on prolonged ischemic compressions and muscle stripping. At the end of each treatment a Gr 2 or 3 sustained cervical distraction was used to maintain joint health and increase ROM. There were modifications made during one of the treatments as the patient presented with a severe headache and so they were treated for such with hydrotherapy (derivation technique with ice on occiput and heat placed on the feet) and light swedish techniques, other than this the treatment protocol stayed the same as previously stated. The patient was sent home with various homecare suggestions such as; stretches to bilateral levator scapula muscles starting at 30 second increments 3 times per side, once per day and slowly working our way to three times per day. Ice was given to the patient as homecare to be used when she was experiencing the onset of a headache and was to be placed at the occiput for no longer then 15mins. Heat was given as a twice daily home care for levator scapula to decrease the pain referral from her trigger points. Pain free AROM of the cervical spine was also given to the patient to do, all ranges were to be done at least once a day but up to as many as three times a day at her discretion. Outcomes The following charts and tables show the changes in ROM, pain and headache occurrences throughout the treatments (Tx). Fig 1. And Fig 2. show a dramatic decrease in the subjective information the patient has provided in regards to the pain they are experiencing with each headache at the beginning of the treatments, as the treatments progressed and at the final treatment. Though all the charts in Fig4. show some increase in AROM, Fig 4d. and 4e. show the most improvement in Lateral Flexion ROM. On both sides from first treatment to final treatment there was an increase of 30°. Fig 1. Headaches on a Pain Scale Progression Pre-Tx vs PostTx (rated from 1-10) 10 9 8 6 5 4 3 2 1 Tx 1 Tx 2 Tx 3 Tx 4 Tx 5 Tx 6 Tx 7 Treatments Pre Tx Post Tx Fig 2. Pain Scale as reported by patient from 1st Tx vs 7th Tx (Pre and Post) 1st Tx 7th Tx Difference Pre Tx 8 3 -5 Post Tx 6 2 -4 Fig 3. Duration (in days) patent reported having headaches 6 5 4 Days Pain Scale 7 3 2 1 0 Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Weeks between treatments Duration of each headache Progression of headaches reported each week Fig 4. Cervical Spine Range of Motion progression Pre Tx and Post Tx (1st, 4th and 7th Tx) Fig 4a. Extension AROM Degrees of movement 70 60 50 40 30 20 10 0 1st Tx 4th Tx 7th Tx Treatments Pre Tx Fig 4b. Right Rotation AROM 70 50 30 10 -10 90 Degrees of movement Degrees of movement 90 Post Tx 1st Tx 4th Tx 7th Tx Fig 4c. Left Rotation AROM 70 50 30 10 -10 1st Tx Treatments 60 Post Tx Pre Tx Fig 4d. Left Lateral Flexion AROM Degrees of movement Degrees of movement Pre Tx 50 40 30 20 10 0 1st Tx 4th Tx Treatments Pre Tx Post Tx 4th Tx 7th Tx Treatments 7th Tx 60 Post Tx Fig 4e. Right Lateral Flexion AROM 50 40 30 20 10 0 1st Tx 4th Tx Treatments Pre Tx Post Tx **Flexion was consistently full so it was not necessary to show a progression chart. 7th Tx At the end of the treatment we were able to achieve the goals of the patient by increasing the patients active pain-free ROM and decreasing the incidences of headaches throughout her week. This was achieved because the patient was compliant with attending treatments every week and doing her homecare when she was able to do it pain free. I think this treatment would be very effective for a patient suffering from chronic WAD as long as the patient was homecare compliant as to do this without the homecare aspect would have taken more treatments and would not be as cost effective. Discussion and Conclusion At the end of this series of treatments the patient left with a decrease in pain from 8-10/10 to 4-5/10, around a 50% decrease in reported symptoms. Her headaches went from an almost daily occurrence to ~2-3x per week and her pain free AROM increased in Lateral Flexion by ~30° on both right and left sides. The increase in ROM and decrease in headache pain and headache occurrence was what was expected to happen through the course of these treatments, these outcomes are also supported by other studies done by Buckland, 2013 and Elesko, 2014. With this evidence I feel this choice of modalities is effective in treating chronic WAD. The only adverse reaction to these treatments was the patient’s consistent feeling of nausea and dizziness post every session, though such side effects could also be due to nervous system damage from her original accident, specifically of the vagus nerve. Recommendations to further improve this study would be; proper assessment and record keeping on the patients use of medication throughout the treatment period, further research on each individual modality used in this case report could be done to determine which would be most effective for a patient suffering from chronic WAD, as well as larger a larger scale version of this study on a sample population. Citations Anatomy Trains website: Fascia. Retrieved from: http://www.anatomytrains.com/fascia/ Buckland, D. (Apr 2013). Efficacy of myofascial and trigger point release in the treatment of chronic whiplash associated disorder. Retrieved from: https://www.rmtbc.ca/sites/default/files/files/Utopia%202%20Diana%20Buckland1.pdf Dixon, M. (2003) Joint Play the Right way (3rd ed.). Vancouver, British Columbia Arthrokinetic publishing Elesko, K. (April 2014) A multimodal approach for chronic whiplash associated disorder pain. Retrieved from: https://www.rmtbc.ca/sites/default/files/files/WCCMTVPT_KElesko2ndPlace.pdf Mayo clinic staff (2015). Definition of Whiplash. Retrieved from: http://www.mayoclinic.org/diseases-conditions/whiplash/basics/definition/con-20033090 Norton, H., Lowe, R., Van Horebeek, E., Bortels, S., & Kistmacher, S. (2013). Whiplash Associated Disorders. Retrieved from: http://www.physio-pedia.com/Whiplash_Associated_Disorders#Chronic_Whiplash Rattray, F. (2000) Clinical Massage Therapy (1st Ed.). Llora, Ontario: Talus Inc. Sutton, D., Côté, P., Wong, J., Varatharajan, S., Randhawa, K., Yu, H., Southerst, D., Shearer, H., Van der Velde, G., Nordin, M., Carroll, L., Mior, S., Taylor-Vaisey, A., & Stupar, M. (2014). Is multimodal care effective for the management of patients with whiplash-associated disorders or neck pain and associated disorders? A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Retrieved from: http://www.thespinejournalonline.com/article/S1529-9430(14)00650-0/fulltext