Over-The-Counter Medications Physicians Orders
advertisement

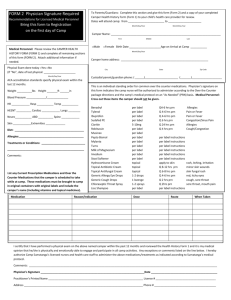
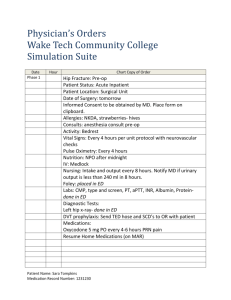
ALL CAMPERS (EXCEPT ABC CAMPERS) MUST HAVE A PHYSICIAN/HEALTHCARE PROVIDER COMPLETE THIS OVER-THE-COUNTER MEDICATIONS FORM Dear Camp Families, St. Crispin’s relies on medical volunteers to ensure the health of everyone at Summer Camp. For years, like many camps, our biggest helpers were Registered Nurses. However, I was recently made aware of concerns from the Oklahoma Board of Nursing that—under the system we were using—it was not appropriate for RNs to dispense the over-the-counter medicines that we keep in stock in the Infirmary. Things like Pepto, Tylenol, Benadryl, antibiotic ointment, and cough drops. After learning this I had a few options (explained below): 1) Though RNs cannot administer from our stock of meds, they can administer meds that each camper brought with them. This is how schools do it. This would mean that every camper would have to bring every possible medicine that they might need at Camp. I decided that this option would be too much of a hassle for our parents, too much of a confusion for our medical staff, and it ran the risk of a camper not being able to receive appropriate care simply because they didn’t pack a certain medicine. 2) I can leave RNs off the list of possible medical volunteers and focus my search on Physician Assistants, Nurse Practitioners, and doctors. It is within the scope of practice of these individuals to dispense the over-thecounter medicines we keep in stock. We did this last year and attempted it this year. However, after months of searching this year I cannot find the number of individuals we need to fill this crucial role. Summer camp is approaching too quickly to rely on this avenue. This leaves the final option as the best option: 3) The final option that addressed the Board of Nursing’s concern is to have each camper visit a doctor before coming to camp. The doctor will fill out a form which lists all medicines we keep in the Infirmary and will indicate for each camper which medicines they may be allowed to take, for what reasons, and how. Having this form on file for each camper will allow RNs to administer appropriate care for our campers. I realize that summer is rapidly approaching and this adds an extra step for our already busy Camp families. I have tried very hard to avoid this extra step for you. I hope you will agree, though, that we must be able to provide the appropriate care for campers while they are here at Camp. This form enables us to do that. If you have questions about this please contact me. Thank you for your understanding. See you at Camp! Daniel Chapman Summer Camp Director stcrispinsdirector@gmail.com 405-382-1619 Over-The-Counter Medications Physicians Orders 36302 State Highway 9, Wewoka, OK 74884 Tel: 405-382-1619 Fax: 405-382-1631 Email: stcrispinsdirector@gmail.com TO BE FILLED OUT BY PHYSICIAN/HEALTHCARE PROVIDER CAMPER NAME: _________________________________________________DATE OF BIRTH: _______________ ALLERGIES:_____________________________________________________________________________________ FOOD SENSITIVITIES:___________________________________________________RECENT WEIGHT: ________ HEALTH CONDITIONS:___________________________________________________________________________ The following over-the-counter (OTC) medications are available in the Infirmary, and can be administered as needed per label instructions by age and weight of the camper. PLEASE NOTE: Absolutely NO over-the-counter medications, supplements, vitamins, or topical ointments can be administered by the camp Registered Nurse (RN), in accordance with the Oklahoma Board of Nursing without a physician’s order. PRESCRIPTION MEDICATIONS CAN BE GIVEN FROM THEIR ORIGINAL CONTAINERS WITH LABELING INTACT TO THE PROVIDER: Please indicate approval for administration by circling YES or NO in the space indicated. MEDICATION ROUTE DOSAGE SCHEDULE & INDICATIONS MAY BE ADMINISTERED Acetaminophen (Tylenol) By mouth (elixir or tablets) Per label instructions By age and weight Every 4 hours PRN headache, pain or fever > 101 °F Yes No Ibuprofen (Motrin) By mouth (elixir, suspension or tablets) Per label instructions By age and weight Every 4 hours PRN headache, pain or fever > 101 °F Yes No Naproxen sodium By mouth (tablets) Per label instructions By age and weight Every 4 hours PRN pain Yes No Phenylephrine HCL OR Pseudoephedrine HCL Guaifenesin (Robitussin or Mucinex) OR Guaifenesin DM (Robitussin DM or Mucinex DM) Diphenhydramine (Benadryl) By mouth (tablets) Every 4 hours PRN nasal congestion Yes No Yes No Yes No Yes No Loratadine (Claritin) OR Cetrizine HCL (Zyrtec) OR Fexofenadine (Allegra) By mouth (elixir, tablets or capsules) By mouth (tablets) By mouth (tablets) By mouth (tablets) Per label instructions By age and weight Per label instructions By age and weight Per label instructions By age and weight Per label instructions By age and weight 10 mg 10 mg 180 mg Yes Yes No No Yes No Phenol (Chloraseptic Spray) Cough Drops Apply topically (oral) By mouth (lozenge) Per label instructions 1 lozenge Yes No Yes No Tums (Calcium Carbonate) By mouth (chewable tablets) Yes No Famotidine (Pepcid) OR Ranitidine (Zantac) Loperamide HCL (Imodium) By mouth (tablets) Yes No Yes No Simethicone By mouth (capsules) Yes No Maalox By mouth (suspension) Yes No Lactase (Lactaid) By mouth (caplets) Yes No Docusate sodium (Colace) By mouth (capsule) Per label instructions By age and weight Per label instructions By age and weight Per label instructions By age and weight Per label instructions By age and weight Per label instructions By age and weight Per label instructions By age and weight Per label instructions By age and weight Yes No By mouth ( tablet or exlixir) By mouth ( tablet or exlixir) By mouth (tabs or capsules) Every 4 hours PRN congestion Every 4 hours PRN cough. Every 6 hours PRN allergies or insect bites Daily PRN allergy symptoms Daily PRN allergy symptoms Daily PRN allergy symptoms or itching unrelieved by topicals Every 2 hours PRN sore throat Every 2 hours PRN cough/sore throat Every 2 hours PRN acid indigestion Daily PRN indigestion or supplement to allergic response After loose stools 1-2x daily PRN gas Every 4 hours PRN upset stomach With first bite of dairy for lactose sensitive children 1-3x daily PRN constipation BRING THIS COMPLETED FORM WITH YOU TO CAMP Page 1 of 2 MEDICATION ROUTE DOSAGE MAY BE SCHEDULE & INDICATIONS ADMINISTERED Psyllium husk (Metamucil) By mouth (capsules) Alcohol/vinegar Ear Drops In ears Hyland’s Earache drops In ears Eye Drops (Sodium Carboymethycellulose OR Saline solution) Aloe Vera Gel Bacitracin/ Neomycin sulfate /Polymyxin (Triple anitibiotic Ointment OR Bacitracin Zinc/ Polymyxin (Polysporin OR Bacitracin Hydrocortisone Cream 1% Antifungal Cream (Clotrimazole 1% or Tolnftate 1% or Miconazole nitrate 2%) Burn Relief Gel (Lidocaine HCL) Orajel Calamine /Zinc oxide Diphenhydramine HCL/Zinc acetate OR StingEze OR AfterBite OR Calamine/ Zinc Oxide OR Chiggerex EpiPen (Epinephrine) Apply topically, ocular Per label instructions By age and weight Per label instructions Apply topically EpiPen Jr(Epinephrine) Per label instructions By age and weight 5 drops 50/50 mix 1-3x daily PRN constipation Yes No After swimming to prevent swimmer ear PRN earache Yes No Yes No Every 4 hours PRN dry, irritated eyes Yes No Per label instructions Apply PRN sunburn Yes No Apply topically Per label instructions Apply 1-3x daily PRN minor cuts Yes No Apply topically Apply topically Per label instructions Per label instructions Apply 3-4x daily PRN skin irritation Apply twice daily to soothe itching Yes No Yes No Apply topically Lidocaine HCL 2.5% Apply 3-4x daily PRN minor burns Apply topically, oral Apply topically Per label instructions Per label instructions Apply 1-4x daily PRN oral pain As needed PRN itching Yes Yes No No Apply topically (spray or cream) Per label instructions Apply 1-4x daily PRN itching Yes No Intramuscular (IM) or subcutaneous (subQ) injection Intramuscular (IM) or subcutaneous (subQ) injection 1 autoinjector 0.3 mg if over 66 lbs PRN allergic emergency. May repeat 1 X after 15 minutes while transporting to emergency facility PRN allergic emergency. May repeat 1 X after 15 minutes while transporting to emergency facility Yes No Yes No 1 Jr autoinjector 0.15 mg for 33- 66 lbs ADDITIONAL/ALTERNATIVE MEDICATIONS TO BE ADMINISTERED AT CAMP MUST INCLUDE ALL PRESCRIPTION MEDS, VITAMINS, & OVER THE COUNTER MEDS MEDICATION ROUTE DOSAGE SCHEDULE COMMENTS Physician/Healthcare Provider Signature:__________________________________ Date:_______________ Practice Address:_____________________________________________________________________________________________ Phone Number:_______________________________________________________________________________________________ Parent Guardian Signature:__________________________________________ Date:_______________ BRING THIS COMPLETED FORM WITH YOU TO CAMP Page 2 of 2