Genomics and the Implications for Health Care
advertisement

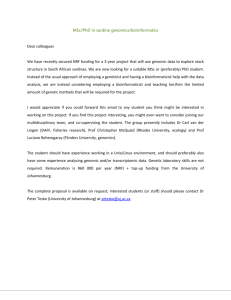
National Health Committee Genomics and the Implications for Health Care March 2015 National Health Committee – Genomics and the Implications for Health Care National Health Committee (NHC) The National Health Committee (NHC) is an independent statutory body charged with prioritising new and existing health technologies and making recommendations to the Minister of Health. It was reformed in 2011 to establish evaluation systems that would provide the New Zealand people and the health sector with greater value for money invested in health. The NHC Executive is the secretariat that supports the Committee. The NHC Executive’s primary objective is to provide the Committee with sufficient information for it to make decisions regarding prioritisation and reprioritisation of interventions and services. They do this through a range of evidence-based products chosen according to the nature of the decision required and timeframe within which decisions need to be made. The New Zealand Government has asked that all new diagnostic and treatment (non-pharmaceutical) services, and significant expansions of existing services, are to be referred to the NHC. In August 2011 the NHC was appointed with new Terms of Reference and a mandate to establish the capacity to assess new and existing health technologies. Its objectives (under Section 4.2 of its Terms of Reference – www.nhc.health.govt.nz) include contributing to improved value for money and fiscal sustainability in the health and disability sector by: providing timely advice and recommendations about relative cost-effectiveness based on the best available evidence; providing advice and recommendations which influence the behaviour of decision makers including clinicians and other health professionals; providing advice and recommendations which are reflected in resource allocation at national, regional and local levels; and contributing to tangible reductions in the use of ineffective interventions and improved targeting to those most likely to benefit. In order to achieve its objectives under Section 4.2 and to achieve ‘Value for Money’, the NHC has adopted a framework of four assessment domains – Clinical Safety & Effectiveness; Economic; Societal & Ethical; and Feasibility of Adoption – in order that assessments cover the range of potential considerations and that the recommendations made are reasonable. It is intended that the research questions asked will fall across these domains to ensure that when the Committee comes to apply its decision-making criteria, it has a balanced range of information available to it. When the NHC is setting those questions they will have the decision-making criteria in mind. The 11 decision-making criteria will assist in the determination of the NHC work programme and in the appraisal and prioritisation of assessments. Page 2 National Health Committee – Genomics and the Implications for Health Care Contents 1 Introduction 4 2 Clinical application of genomic testing 5 2.1 Genetic risk prediction 5 2.2 Disease diagnosis 6 2.3 Clinical management 6 3 Test performance 8 4 Supporting infrastructure 9 4.1 Diagnostic test assessment 10 4.2 Laboratory perspective 10 4.3 Workforce 11 4.4 Clinical application 12 5 Ethical perspective 13 6 A wider health perspective 14 7 New Zealand services provision 15 8 Summary 16 Glossary 18 References 19 National Health Committee (NHC) and Executive 22 Disclaimer 22 Page 3 National Health Committee – Genomics and the Implications for Health Care 1 Introduction Greater understanding of the human genome offers the opportunity to improve the delivery of personalised medicine: ‘to tailor medical care to specific individual characteristics, needs and preferences of a patient, from prevention, to diagnosis, treatment and to follow-up’.(7) The completion of the Human Genome Project in 2003 was a major driver for the current period of biomedical discovery, the pace of which continues to accelerate.(1) Genetic predisposition plays a central role in most common diseases, and is the primary cause of most rare diseases.(8) Enormous advances have been made in the understanding of genetic disease.(9) The next-generation sequencing technology will enhance further analysis and the US Food and Drug Administration (FDA) has recently approved a sequencing technology for use.(10) The cost of genomic analysis is falling and it may soon be easier and cheaper to sequence the whole genome rather than to extract and test relevant sections for a number of known mutations.(11) From the viewpoint of the FDA, personalised medicine has arrived, as since 2011 one-third of new drug approvals have had an associated genetic or other bio-marker that influences treatment choice. Patients with breast, colorectal, and lung cancers, and melanomas, can be offered a molecular diagnosis allowing the selection of treatments that are more likely to improve outcomes. Genotyping for drug-metabolising enzymes has allowed potential improvements in dosing of drugs.(7) However, it is recognised that, at the current phase of development, the amount of available data is increasing significantly, but the capacity for interpretation of the data is still rudimentary, generating the risk of doing harm.(8) In conjunction it is recognised that access to testing and data will increase as the cost of testing continues to fall, and the challenges of storage, analysis and interpretation will be substantial.(9) Additionally, who should be tested, how much of the genome sequenced, what should be tested, validated and communicated to patients as well sharing data for further development are key considerations.(12) Page 4 National Health Committee – Genomics and the Implications for Health Care 2 Clinical application of genomic testing Broadly the areas of health care in which genomic testing is seen to be playing a role, though not with equal impact, are: risk assessment for disease incidence disease diagnosis clinical management of diagnosed disease for both intervention effectiveness and safety surveillance of disease recurrence. 2.1 Genetic risk prediction The importance of genetics is well recognised in single gene related disorders, where mutation to a single gene results in the expression of clinical disease. The inheritance of common diseases is usually polygenic and disease outcome is also dependent on environmental factors. Genome-wide association studies (GWAS) look for associations between typically thousands of specific genetic variations, commonly single-nucleotide polymorphisms (SNPs), and particular diseases or traits. The variations do not cause the disease but are closely linked in space to an unidentified gene that does influence the disease presentation. Each of the identified variations tends to have a relatively small individual effect.(4, 6) Generally the association between individual SNPs and traits is small and currently known variants explain too little about the risk of disease occurrence to be clinically useful.(3, 13) Testing is possible for multiple diseases and the predictive results may provide conflicting options: actions may reduce the risk for one and increase the risk for another disease development.(3) As with other forms of screening, the potential benefits are dependent on more than test performance alone. The disease prevalence and the costs and benefits of potential interventions are crucial.(13) The genetic susceptibility of individuals to developing type 2 diabetes has been elucidated for the rarer forms of the disease. GWAS of population-based samples have identified loci that influence the risk of obesity and diabetes, but the effect size of identified variants is small. The overall explained predisposition is small, up to 10% for diabetes and 1% for obesity. Currently high-risk individuals are better identified on the basis of known risk factors. There is limited evidence to indicate that information on genetic disposition can be used to guide modification of long-term behaviour. The rationale for testing is to improve pathological understanding and to stratify patients for potential future therapeutic interventions.(4) Similarly, with respect to cardiovascular diseases, there is insufficient evidence to warrant the use of a genetic risk score based on SNPs.(6) Direct to consumer testing, a form of screening that provides prediction of risk for future disease, is available at a cost of about US$100. The clinical usefulness is low.(14) Page 5 National Health Committee – Genomics and the Implications for Health Care Susceptibility genes increase the risk of an individual developing a particular disease. For example, mutations of the BRCA1 and BRCA2 genes predispose substantially towards the development of breast and ovarian cancers, and mutations of the MLH1 and MLH2 genes increase the risk of colorectal cancer. Testing for these is part of routine practice in specific populations.(15) 2.2 Disease diagnosis Genomic examination is being used to increase the understanding of the genetic components of intellectual disability. Copy-number changes, micro-deletions and micro-duplications have been identified with intellectual disability and autism. About 14% of cases of developmental delay can be explained by copy-number variation.(5) There is potential to identify biomarkers of Alzheimer’s disease which could lead to earlier interventions.(16) 2.3 Clinical management Genomic analysis has become part of clinical practice, particularly in the field of oncology. The technology has been applied in practice in a number of ways:(15) Prognostic indicator. The use of gene-expression markers of tumours to identify prognostic subgroups and then appropriate therapy options. There is a need to ensure that the testing is appraised adequately and its use may have implications for the size and complexity of clinical trials.(15) A health technology assessment, so far unpublished, has considered the benefits and harms of 11 prognostic tests. The study found that there was good evidence in half that prognostic accuracy was increased, but evidence was lacking as to whether this led to improved patient outcomes.1 Monitoring of disease burden and early recurrence. Monitoring of genetic markers in blood has been used for haematological cancers and may develop to be effective for solid tumours, in addition to usual imaging methods.(15) Pharmacogenomics is the study of the inherited and acquired genetic variation in drug response.(17) In the cancer field, the following have been used: Optimising the use of therapeutics. The expression of particular genes by a tumour can determine the effectiveness and safety in response to a specific agent, e.g. the metabolism of the immunosuppressive agent azathioprine is dependent on the presence of the enzyme Thiopurine S-methyltransferase (TPMT). Its deficiency can lead to serious toxic effects from the drug.(18, 19) Genomic marker identification has been used to reduce drug adverse reaction in the treatment of HIV.(20) Identification of new therapeutics. The presence of a tumour expressed gene, with an understanding of how it affects cellular function, may lead to the development of drugs targeted at that part of the pathway, e.g. the presence of BRAF mutation in melanoma and the development of drugs that act on specific cellular function to a specific agent.(21, 22) 1 Agency of Healthcare Research and Quality. Page 6 National Health Committee – Genomics and the Implications for Health Care Acquired resistance to therapy. Identification of genomic changes in a sub-clone of cancer cells that indicate resistance to primary therapy may be used to decide on appropriate initial stage multiple agent therapy.(15) In cardiovascular medicine it is well known that there is variable patient response to dosing with warfarin, with impact on the risk of serious adverse events associated with anti-coagulation. Two common alleles have been identified that have a small fraction of the activity for the enzyme that metabolises the drug, that results in increased risk of complications. The FDA drug labelling now includes genetic information. However clinical uptake of the information has been slow.(17) Though trials show promise, addition of pharmacogenomics has yet to be of proven additional benefit.(23) The timely access to genomic information to guide prescribing has been a limitation to its potential use.(10) Page 7 National Health Committee – Genomics and the Implications for Health Care 3 Test performance In whatever field of health care genomic testing is used, particular tests must provide meaningful information. The Centre for Disease Control and Prevention has produced the ACCE framework for evaluating genetic tests (Figure 1). The acronym is taken from its primary components: Analytic validity, clinical validity, clinical utility and associated ethical, legal and social implications. Figure 1. ACCE model process for evaluating genetic tests PPV = positive predictive value; NPV = negative predictive value. Source: CDC-http://www.cdc.gov/genomics/gtesting/ACCE/ The analytical and clinical validity of the test set the foundations of how well a particular test operates technically and measures a clinical entity. The elements of analytical validity include how well it detects the genotype of interest (sensitivity), how well it classifies samples without the specific mutation (specificity), laboratory quality control and assay robustness in the face of pre-analytical and analytical variables. Clinical validity is measured by sensitivity and specificity and the predictive value of the test, which is dependent on the disease prevalence. Clinical utility considers the value of testing in the context of real-world clinical delivery. Page 8 National Health Committee – Genomics and the Implications for Health Care 4 Supporting infrastructure To ensure genetic testing is successfully integrated into medical practice, necessary aspects that have been recognised include: oversight to ensure the accuracy and reliability of genetic tests; an educated health care workforce; data protection and protection from discriminatory use.(21) In the UK, Genomics England is the arm of the Department of Health leading the development of genomic medicine into the health service. As well as planning to link genomic mapping with 100,000 patients with selected cancers, infectious diseases and rare diseases, the project plans to develop the necessary medical scientists and educate the wider medical community to support the technology. There is also the need to manage and integrate data for clinical and research use.2 A US Centers for Disease Control and Prevention (CDC) sponsored report, based on engagement with multiple stakeholders, identifies a number of key elements: professional education, public education, research to have a public health lens with a health outcomes focus, test assurance and the regulation of technologies.(24) A report on the use of whole genome sequencing within the UK health system recommended that genomic testing should be clinically targeted and with clear benefits over existing tests. Health care professionals need further development of competencies and support and clear and rational commissioning pathways are necessary.(11) Given the limitations in understanding genomic data, testing should be used to answer clinical questions.(12) Genomic testing will generate large amounts of data that will create a storage challenge.(9) Secure storage will need to cover retrieval for the individual’s use while allowing approved research access for the future benefit of all.(25) The development of clinical informatics is crucial.(11) Genomic data may be incorporated into a national New Zealand breast cancer registry with the amalgamation of the current regional registries.3 The FDA has considered its position in response to the changing medical technology. It highlights that in the translation of the biological knowledge there are considerable challenges related to the accuracy and performance of the diagnostic tests. The co-development of diagnostic tests and linked therapeutic agents brings an added challenge. In assessing a diagnostic test the analytical validity, clinical validity and clinical utility are to be assessed. It notes the problems generated when different testing technologies are used. Diagnostic test kits are standardised and used across laboratories while laboratory developed tests are site-specific and are more commonly used in the current field of genomics. This leads to risk in the quality of testing and interpretation. 2 http://www.genomicsengland.co.uk/100k-genome-project/ 3 Personal communication: Sector Capability and Implementation, Cancer Services Page 9 National Health Committee – Genomics and the Implications for Health Care In its response the FDA is developing regulatory standards, reference libraries and research methods. These include: Biomarker Qualification Programme − once a biomarker has been approved within a specified context of use, drug developers do not need to reconfirm its approval MicroArray and Sequencing Control Project − development of standards, quality control and guidance for these technologies Genomic Reference Library for Evaluating Whole Genome Sequencing − sharing of performance data for instruments and uses guidance for clinical trial designs and methodologies. 4.1 Diagnostic test assessment The CDC has established the Evaluation of Genomic Applications in Practice and Prevention (EGAPP) to establish and test a systematic, evidence-based process for evaluating genetic tests and other applications of genomic technology that are in transition from research to clinical and public health practice. This independent, multidisciplinary panel prioritises and selects tests, reviews CDC-commissioned evidence reports and other contextual factors, highlights critical knowledge gaps, and provides guidance on appropriate use of genetic tests in specific clinical scenarios.(26) A summary of its recommendations are available.4 European Union(27) and UK(28) organisations also assess genetic tests for clinical utility and laboratory quality management, with the UK Genetic Testing Network leading in the development of governance that ensures proper evaluation of tests before clinical use.(9) 4.2 Laboratory perspective The Royal College of Pathologists of Australasia (RCPA) has proposed a National Framework for Genetic Testing.5 It incorporates assessment of the diagnostic test as well as classification of laboratories. It is suggested that genetic tests should be classified by clinical utility and that would determine its availability or not. Tests should be assessed by complexity and classification of laboratories would determine the range of tests they could offer. Test by volume and complexity: High volume simple testing: technically simple assays, with simple interpretation. For example BCR/ABL1 testing in chronic myeloid leukaemia. Moderate volume complex testing: tests of more complexity than the high volume tests in both their execution and interpretation. For example Huntington disease testing. 4 http://www.egappreviews.org/recommendations/index.htm 5 RCPA response to Genetics Working Party Chair’s request for options – November 2012 Page 10 National Health Committee – Genomics and the Implications for Health Care Low volume testing: tests usually more complex in both execution and interpretation, the complexity compounded by the infrequent nature of the assays, especially if the small number of assays was distributed over more laboratories than necessary, for example RB1 testing in children with retinoblastoma. Classification of laboratory subsequent to test classification: Class 1: These laboratories are those approved to perform high volume simple tests only. The only requirement on a Class 1 laboratory is that it has the New Zealand accreditation to perform molecular genetic testing. Class 2: These laboratories are those approved to perform moderate volume complex testing in addition to high volume simple tests. These laboratories must operate in close and effective liaison with relevant specialist clinical services, potentially including genetic and counselling services. Class 3: These laboratories would be classed as national genetic reference laboratories that must have the requisite clinical and genetic expertise to offer a comprehensive genetic testing and advisory service for the disorder in question. 4.3 Workforce Developments in genomic technology are expected to have significant workforce implications. Highly skilled programmers and analysts are necessary to interpret the complex data. Increased preventative screening will potentially lead to increased need for multiple professions to be involved in the interventional response to the screening programme, such as dieticians and pharmacists.(16) However training, recruitment and retention of laboratory staff is seen as a challenge. There is a shortage of pathologists as well as technical staff.6 The RCPA recognises the need for workforce development requirements for laboratory staff as well as clinical referrers.7 Many non-geneticist clinicians have limited insight into the genetics of the diseases they deal with(29) or of genetics in general.(30) Education of health professionals could begin with integration of genomics into primary training programmes in addition to training of existing professionals. Similarly public education can commence with integration into the school curricula as well as wider community engagement,(24) including the work of national museums.(31) 6 Community Pathology Services in New Zealand: Environmental Scan and Background Paper, May 2011 prepared for Ministry of Health 7 RCPA response to Genetics Working Party Chair’s request for options – November 2012 Page 11 National Health Committee – Genomics and the Implications for Health Care 4.4 Clinical application The development of simple algorithms will be necessary to help clinician interpretation of genetic data.(17) Linking results of genomic testing to the patient electronic clinical records may allow effective use of the information but increases risk of unauthorised access.(21) However, as point-oftesting develops, such as specific testing for drug sensitivity, with rapid results,(8) clinical application may become easier. Page 12 National Health Committee – Genomics and the Implications for Health Care 5 Ethical perspective In respect of research using medical records and specimen data in conjunction with genomic data, the consent for future research after the original specimen is collected remains unclear. The pressure to share data more broadly to enhance understanding brings increased risk to privacy. Broadening consent is an option to allow further research as knowledge progresses, and overcomes the issue of retracing participants. However, broader consent for future use of data reduces consent as there is less clarity at the time of consent. A tiered approach to consent regarding future research is an option.(21) The UK Genomic project has utilised an “everything can be done” consent for their data. Participants can be contacted in future to enrol in future trials.(32) Consideration should be given to consent withdrawal, implications for relatives, what secondary use is allowed and the potential impact of commercial gain by the private sector from the data.(9) Privacy is at risk through the linking of databases, even if research data is collected anonymously.(9) In the US genetic information cannot be used when considering health care insurance, but can be used by companies when assessing risk of life, disability or long-term care insurance. Employers cannot use genetic data to discriminate.(21) As the clinical usefulness of personal genomic screening is considered low, with the risk of misinterpretation, professional bodies have published position statements and some countries have regulated its use.(33) It is unknown how individuals may respond to genetic data with an estimation of future risk. They may react fatalistically and be less inclined to use protective options and so knowledge of the result does the individual a disservice. Also currently known risk behaviours are much more important than genetic variation.(9) When the whole genome is interrogated, in the context of answering a specific clinical problem, incidental findings can result. These are results that are not directly related to the clinical question. The interpretation of these results may be less or more clear, and have implications for the individual or their family. In response to the risk of ‘dumping heaps of molecular uncertainty on patients’, geneticists in the Netherlands try to interpret exomes provided by clinicians and pass on information about variants of known relevance plus incidental findings of obvious importance.(8) The American College of Medical Geneticists issued a policy statement on the reporting of incidental findings.(34) It provides a list of mutations that should be reported regardless of the indication for testing, based on their potential to be verified by other means and for the individual to be offered medical intervention as appropriate. The European Society of Human Genetics recommended filtering of results to avoid unsolicited results.(35) Proposals for dealing with results from whole genome testing in Canada considered the issue from ethical guiding principles and with respect to groups of varying competence and proximity to the person tested. Its recommendations note the need for professional expertise, use of testing to answer a clinical question, maintenance of confidentiality and to consider the best interests of the children and adults.(35) Page 13 National Health Committee – Genomics and the Implications for Health Care 6 A wider health perspective The determinants in health are multifactorial; genetics is one determinant that interacts with behavioural factors and socioeconomic factors.(36) The FDA, though acknowledging the importance of genomics in the development of ‘personalised medicine’, also points out that diseases are not only the result of our genes but that there is an important interaction with environmental, social and cultural factors.(7) Research using genomics should be done in conjunction with exploring the environmental contributions to disease.(24) A challenge is to formulate how screening via GWAS operates without undermining effective population health policies that reduce exposure to the common risk factors responsible for common diseases.(37) Page 14 National Health Committee – Genomics and the Implications for Health Care 7 New Zealand services provision The Genetic Health Service New Zealand (GHSNZ) is the provider of expert genetic diagnosis and advice, and was set up in 2011 to provide a consistent New Zealand wide service. It has 7.8 FTE consultants and 12.4 FTE genetic counsellors. In 2012/13 the service had nearly 5000 referrals, arranged 2972 tests at a total cost of $925,000 and an average cost of $310. The expected increase in demand for services with advances in technology is an acknowledged risk. Currently the GHSNZ does not have a national database to link family data.(38) The service expresses concerns about the current clinical utility of some genomic testing, and that the ability to apply the vast increase in data clinically is a limiting step to its use. A pilot clinical programme focused on families with undiagnosed rare diseases has been initiated by University of Otago in conjunction with a genomics corporate. The service recommends that: new tests have proven clinical utility and technical and clinical expertise is available requesters are fully aware of clinical utility and cost of testing GHSNZ does not necessarily have the resources to support referrers, laboratories and DHBs in the use of tests.(38) A report commissioned prior to the setting up of GHSNZ noted the current challenges:(30) inequity of service delivery insufficient IT support the need for workforce planning the need for demand management a lack of genetic knowledge among referrers. GHSNZ is not involved in ‘companion testing’ where genetic testing determines the clinical value of a specified medication such as in cancer services. Genetic testing is done in ‘standalone’ laboratories and can be an income stream for the laboratory. Advice on clinical utility is not requested and requests come via clinicians who may not have sufficient understanding of the clinical utility of the test.8 There are New Zealand test result repositories that may be an appropriate starting point to consider the storage of genomic data. 8 Personal communication, Dr Joanne Dixon, National Clinical Director, GHSNZ, October 2013 Page 15 National Health Committee – Genomics and the Implications for Health Care 8 Summary When the previous National Health Committee considered molecular genetic testing in 2003, it acknowledged future developments following the Human Genome Project, and the challenges it would bring; the speed of change in knowledge, the level of genetic knowledge among clinicians, the level of knowledge amongst the public and the configuration of services. Its recommendations related to assessing tests by their clinical validity and utility, access to safe and effective testing, quality control and accreditation for laboratory services, workforce development including the education of the medical providers and more accessible information for the public.(39) These considerations remain relevant as the potential role for genomic medicine has developed. A framework to ensure that genomic medicine is provided safely and effectively has a number of components: 1. Assessment and designation of specific genomic tests to demonstrate validity and clinical utility In order for tests to be provided within the public health system, tests must clear utility based on evidence. New Zealand does not need to perform this task de novo as US and European authorities have structures in place currently for this task. New Zealand would be in a position to transfer the knowledge to its own circumstances. Tests should be applied to the management of clear clinical questions. The National Laboratory Roundtable strategic framework identified the opportunity for a national process for the introduction of all new testing. 2. Assurance of genomic testing Assurance of both testing methods and of the laboratories performing tests is required. Laboratory accreditation could be based on the Royal College of Pathologists of Australasia tiered approach to laboratory service designation. 3. Workforce development The provision of genomic health technology and services requires a skilled scientific workforce in testing and interpretation environments. The current health care workforce: genetic specialists, general medical specialists and primary care physicians need to have sufficient understanding of genomics to be able to apply the technology appropriately to clinical practice. This requires short to medium-term training as well as longer-term education of the students. The development and maintenance of the laboratory workforce is already viewed as challenging. 4. Public education The general population needs to be informed and educated in the abilities and limitations of the technology in order to promote informed decision-making. This too has medium and longer-term aspects. Page 16 National Health Committee – Genomics and the Implications for Health Care 5. Information technology development It is necessary to develop the resources to archive and retrieve the large amounts of data that are generated in the genome sequencing. Clinically relevant information must be made available effectively and in a timely manner to clinical IT systems to provide support to clinicians. 6. Broader health The development and application of genomic medicine knowledge to improve health should be used in conjunction with existing knowledge on the behavioural and social determinants of health, to provide a coherent approach to achieving health gain. 7. Ethical The ethical implications of genomic testing and the possible impact on privacy and discrimination need consideration within the development of services and more broadly. Page 17 National Health Committee – Genomics and the Implications for Health Care Glossary Gene The traditionally defined unit of hereditary. Genome The whole of the inheritable information. Allele One of two or more versions of a genetic sequence at a chromosomal location. Genomics The study of function and interactions of all the genes in the genome. Genetics Study of single genes. Exome Protein coding sequences of the genome. Polygenic Produced by two or more genes. Epigenetic Non-mutational phenomena that alter the expression of a gene. Single-nucleotide polymorphism (SNP) A single-nucleotide variation in a genetic sequence; a common form of variation in the human genome. Mutation Usually term reserved for genetic variation in DNA that is known to cause pathology. Copy number changes A deletion of duplication of a stretch of DNA. Germ cells Gametes that pass on hereditary information to the next generation. Germ line changes Become ubiquitous in the earliest stages of the developing body and so are present in all cells. Somatic mutation A deleterious genetic variation occurring in any cell of the body except sperm or egg cells. Variations in somatic cells can affect the person in whom they occur but are not passed on to offspring. Whole-genome sequencing Sequencing the coding regions, or exons, of the entire genome. Next-generation sequencing DNA sequencing that harnesses advances in miniaturisation technology to simultaneously sequence multiple areas of the genome rapidly and at low cost. Genomewide association study An approach used in genetics research to look for associations between many (typically hundreds of thousands) specific genetic variations (most commonly single-nucleotide polymorphisms) and particular diseases. Sources: (1-6) Page 18 National Health Committee – Genomics and the Implications for Health Care References 1. Feero WG, Guttmacher AE, Collins FS. Genomic Medicine — an Updated Primer. New England Journal of Medicine. 2010;362(21):2001-11. doi: doi:10.1056/NEJMra0907175. 2. Guttmacher AE, Collins FS. Genomic Medicine — a Primer. New England Journal of Medicine. 2002;347(19):1512-20. doi: doi:10.1056/NEJMra012240. 3. Manolio TA. Genomewide Association Studies and Assessment of the Risk of Disease. New England Journal of Medicine. 2010;363(2):166-76. doi: doi:10.1056/NEJMra0905980. 4. McCarthy MI. Genomics, Type 2 Diabetes, and Obesity. New England Journal of Medicine. 2010;363(24):2339-50. doi: doi:10.1056/NEJMra0906948. 5. Mefford HC, Batshaw ML, Hoffman EP. Genomics, Intellectual Disability, and Autism. New England Journal of Medicine. 2012;366(8):733-43. doi: doi:10.1056/NEJMra1114194. 6. O’Donnell CJ, Nabel EG. Genomics of Cardiovascular Disease. New England Journal of Medicine. 2011;365(22):2098-109. doi: doi:10.1056/NEJMra1105239. 7. Paving the Way for Personalized Medicine: FDA’s Role in a New Era of Medical Product Development2013 27/01/2014. Available from: http://www.fda.gov/downloads/scienceresearch/specialtopics/personalizedmedicine/ucm372421. pdf. 8. Burn J. Should We Sequence Everyone’s Genome? Yes. BMJ. 2013;346. doi: 10.1136/bmj.f3133. 9. Flinter F. Should We Sequence Everyone’s Genome? No. BMJ. 2013;346. doi: 10.1136/bmj.f3132. 10. Collins FS, Hamburg MA. First Fda Authorization for Next-Generation Sequencer. N Engl J Med. 2013;369(25):2369-71. doi: 10.1056/NEJMp1314561. 11. Wright C. Next Step in the Sequence: The Implications of Whole Genome Sequencing for Health in the U.K2013 September 2013. Available from: http://www.phgfoundation.org/file/10363/. 12. Wright CF, Middleton A, Burton H, Cunningham F, Humphries SE, Hurst J, et al. Policy Challenges of Clinical Genome Sequencing. BMJ. 2013;347:f6845. doi: 10.1136/bmj.f6845. 13. Kraft P, Hunter DJ. Genetic Risk Prediction — Are We There Yet? New England Journal of Medicine. 2009;360(17):1701-3. doi: doi:10.1056/NEJMp0810107. 14. Doerr M, Eng C. Personalised Care and the Genome. BMJ. 2012;344. doi: 10.1136/bmj.e3174. 15. McDermott U, Downing JR, Stratton MR. Genomics and the Continuum of Cancer Care. New England Journal of Medicine. 2011;364(4):340-50. doi: doi:10.1056/NEJMra0907178. 16. The Technology Horizon: Preliminary Review on Technologies Impacting the Future Health and Social Care Workforce2013. Available from: http://www.cfwi.org.uk/publications/the-technologyhorizon-preliminary-review-on-technologies-impacting-the-future-health-and-social-careworkforce. 17. Wang L, McLeod HL, Weinshilboum RM. Genomics and Drug Response. New England Journal of Medicine. 2011;364(12):1144-53. doi: doi:10.1056/NEJMra1010600. Page 19 National Health Committee – Genomics and the Implications for Health Care 18. Weinshilboum RM, Sladek SL. Mercaptopurine Pharmacogenetics: Monogenic Inheritance of Erythrocyte Thiopurine Methyltransferase Activity. American journal of human genetics. 1980;32(5):651. 19. Dean L. Azathioprine Therapy and Tpmt Genotype: Azathioprine Therapy and TPMT Genotype; 2013. Available from: http://www.ncbi.nlm.nih.gov/books/NBK100661/. 20. Martin M, Klein T, Dong B, Pirmohamed M, Haas D, Kroetz D. Clinical Pharmacogenetics Implementation Consortium Guidelines for Hla-B Genotype and Abacavir Dosing. Clinical Pharmacology & Therapeutics. 2012;91(4):734-8. 21. Hudson KL. Genomics, Health Care, and Society. New England Journal of Medicine. 2011;365(11):1033-41. doi: doi:10.1056/NEJMra1010517. 22. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, et al. Improved Survival with Vemurafenib in Melanoma with Braf V600e Mutation. N Engl J Med. 2011;364(26):2507-16. doi: 10.1056/NEJMoa1103782. 23. Zineh I, Pacanowski M, Woodcock J. Pharmacogenetics and Coumarin Dosing — Recalibrating Expectations. New England Journal of Medicine. 2013;369(24):2273-5. doi: doi:10.1056/NEJMp1314529. 24. Priorities for Public Health Genomics 2012–20172011. Available from: http://genomicsforum.org/files/geno_report_WEB_w_RFI_1122rev.pdf. 25. Wright CF, Middleton A, Burton H, Cunningham F, Humphries SE, Hurst J, et al. Policy Challenges of Clinical Genome Sequencing. BMJ. 2013;347. doi: 10.1136/bmj.f6845. 26. Evaluation of Genomic Applications in Practice and Prevention [cited 2014 27/01/2014]. Available from: http://www.egappreviews.org/. 27. Eurogentest [27/01/2014]. Available from: http://www.eurogentest.org/index.php?id=138. 28. UK Genetic Testing Network. Available from: http://ukgtn.nhs.uk/our-work/. 29. Kent A. Commentary: Patients Will Need Knowledgeable Guidance. BMJ. 2013;347:f6991. doi: 10.1136/bmj.f6991. 30. Heffors M, Artus J, van Hessen E. Development of a National Clinical Genetics Service. 2009. 31. Smithsonian National Museum of Natural History. Unlocking Life’s Code [12/02/2014]. Available from: http://unlockinglifescode.org/. 32. Torjesen I. Genomes of 100,000 People Will Be Sequenced to Create an Open Access Research Resource. BMJ. 2013;347:f6690. doi: 10.1136/bmj.f6690. 33. Doerr M, Eng C. Personalised Care and the Genome. BMJ. 2012;344:e3174. doi: 10.1136/bmj.e3174. 34. Green RC, Berg JS, Grody WW, Kalia SS, Korf BR, Martin CL, et al. Acmg Recommendations for Reporting of Incidental Findings in Clinical Exome and Genome Sequencing. Genet Med. 2013;15(7):565-74. doi: 10.1038/gim.2013.73. 35. Zawati MH, Parry D, Thorogood A, Nguyen MT, Boycott KM, Rosenblatt D, et al. Reporting Results from Whole-Genome and Whole-Exome Sequencing in Clinical Practice: A Proposal for Canada? J Med Genet. 2014;51(1):68-70. doi: 10.1136/jmedgenet-2013-101934. Page 20 National Health Committee – Genomics and the Implications for Health Care 36. Social Determinants of Health: The Solid Facts, Second Edition. World Health Organisation, 2003. Available from: http://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf. 37. Hall WD, Mathews R, Morley KI. Being More Realistic About the Public Health Impact of Genomic Medicine. PLoS Med. 2010;7(10):e1000347. doi: 10.1371/journal.pmed.1000347. 38. Genetic Health Service New Zealand. Annual Report: July 2012-June 2013. 2013. 39. National Health Committee. Molecular Genetic Testing in New Zealand. 2003. Page 21 National Health Committee – Genomics and the Implications for Health Care National Health Committee (NHC) and Executive The National Health Committee (NHC) is an independent statutory body which provides advice to the New Zealand Minister of Health. It was reformed in 2011 to establish evaluation systems that would provide the New Zealand people and health sector with greater value for the money invested in health. The NHC Executive are the secretariat that supports the Committee. The NHC Executive’s primary objective is to provide the Committee with sufficient information for them to make recommendations regarding prioritisation and reprioritisation of interventions. They do this through a range of evidence-based reports tailored to the nature of the decision required and timeframe within which decisions need to be made. Citation: National Health Committee. 2015. Genomics and the Implications for Health Care. Wellington: National Health Committee. Published in March 2015 by the National Health Committee PO Box 5013, Wellington, New Zealand ISBN 978-0-478-42861-2 (online) HP 5952 This document is available on the National Health Committee’s website: http://www.nhc.health.govt.nz/ Disclaimer The information provided in this report is intended to provide general information to clinicians, health and disability service providers and the public, and is not intended to address specific circumstances of any particular individual or entity. All reasonable measures have been taken to ensure the quality and accuracy of the information provided. If you find any information that you believe may be inaccurate, please email to NHC_Info@nhc.govt.nz. The National Health Committee is an independent committee established by the Minister of Health. The information in this report is the work of the National Health Committee and does not necessarily represent the views of the Ministry of Health. The National Health Committee makes no warranty, expressed or implied, nor assumes any legal liability or responsibility for the accuracy, correctness, completeness or use of any information provided. Nothing contained in this report shall be relied on as a promise or representation by the New Zealand government or the National Health Committee. The contents of this report should not be construed as legal or professional advice and specific advice from qualified professional people should be sought before undertaking any action following information in this report. Any reference to any specific commercial product, process, or service by trade name, trademark, manufacturer, or otherwise does not constitute an endorsement or recommendation by the New Zealand government or the National Health Committee. Page 22