- Critical Care Nutrition
advertisement

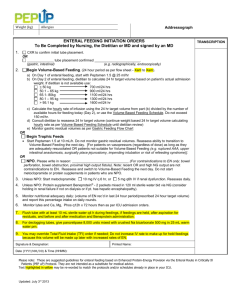
The PEPuP Protocol Self-learning Module Your ICU is implementing PEPuP Protocol. The main objective of this protocol is to improve the adequacy of enteral feeding delivery. Why is this important? Adequate nutrition is very important to support the optimal recovery of critically ill patients. Sufficient nutrition helps to: Provide fuel for cellular metabolism Prevent protein loss and muscle wasting Decrease ventilator time Help prevent infection including ventilator associated pneumonia Promote healthy wound healing Decrease ICU length of stay Reduce mortality Did you know? International audits of nutrition practices have found that ICU patients only receive 40-50% of their nutritional requirements. This means that ICU patients worldwide are iatrogenically malnourished – in other words, we made them that way! What’s New? There a few things about the PEPuP Protocol that may be quite different from how you are providing EN currently. These include: All patients will initially receive a semi-elemental enteral formula All patients will start on the protein supplement Beneprotein®: o 2 packets (14 g) mixed in 120 ml water administered bid via OG/NG All patients will be given metoclopramide on Day 1 of enteral feeding - 10 mg IV q 6h The gastric residual volume threshold is 300 mL 1 The enteral feeding initiation orders is the form that the admitting physician or resident will use to order the appropriate feeding option for your patient. You will notice that NPO is rarely an option; this should be chosen only when there is an absolute contraindication to enteral feeding. You will see some examples of contraindications given in the pre-printed orders. Even the sickest patient should be started on a low level of feeding, trophic feeds, to help maintain gut health. Gut disuse (aka NPO) causes loss of functional and structural integrity of the GI tract and is associated with increased complications. The other big difference you will see is that your patients’ feeds will now be based on a 24-hour target volume rather than the traditional hourly rate you are likely used to. This means that you may be changing hourly rates throughout the day to make up for times when the feeds are off. The case studies that follow will help you to work through these changes and become familiar with the PEP uP protocol. As you work through the case studies, we will ask you questions to test your knowledge. For the first case study, the answers are provided immediately after the questions. For the second case study, answers are found in the Appendix and there is an answer key at the end. The case studies are based on a semi-elemental formula that is 1.5 kcal/ml. The tools referred to in the case studies can be found on the PEP uP Tools page of our website www.criticalcarenutrition.com. 2 Case Studies Case Study Number 1 A 35 year old male was admitted at 0400 hr following a gunshot wound to chest. His injuries include massive trauma to right arm, left chest and left shoulder. He experienced 3 intra-operative cardiac arrests. On arrival to the ICU he is in pulmonary edema, right heart failure, vasopressin at 0.04 units/hr and his levophed continues to be titrated up to maintain a MAP of 60 mmHg; the current rate is 25 mcg/min. His weighs 70 Kg and he is 1.74 m tall. Questions: 1. On admission you inform the medical team that the patient is NPO. Which of the following interventions do you anticipate? a. Continue NPO b. Volume based enteral feeds c. Enteral feeds at 25/hr d. Trophic feeds If you chose trophic feeds you are correct. Because he is still requires vasopressors to maintain a MAP of 60 mmHg he may not be ready to start on volume based feeds. Starting on trophic feeds at 10 mL/hr will help protect his gut until he is stable. 2. He is oliguric, and his creatinine and urea continue to rise. What dose of metoclopramide will you administer? a. Metoclopramide 10 mg q6h b. Metoclopramide 5 mg q6h c. Metoclopramide 10 mg q8h d. Metoclopramide not indicated Did you find the correct answer in the enteral feeding orders? 3 On day 2 his levophed and vasopressin are discontinued. His enteral feeds are at 10 mL/hr. Questions: 3. On morning rounds you inform the medical team that the patient no longer requires vasopressor support and is receiving trophic feeds. What intervention do you anticipate? a. Increase trophic rate from 10 to 20 mL/hr b. Start enteral feeds at 25mL/hr and increase to target of 70mL/hr c. Start volume feeds at a target goal rate determined by dietitian d. Start volume feeds at 1100 mL/hr over 24 hours Starting volume feeds at a rate determined by a dietitian is the best choice. The PEPuP Protocol is meant for initial nutrition orders and reassessment by the dietitian is always the next step to make sure each patient’s individual nutrition requirements are met. If this patient was admitted on a weekend however, he could be moved over the volume feeding of 1100 mL per 24 hrs (based on his weight of 70 Kg) until Monday when he is stable. Make sure to bring this up at morning rounds. 4. At 0800 hr you measured the gastric residual volume and it is 350 mL. You replace the aspirate and continue feeding at target goal rate. At 1200 hr his gastric residuals are measured again and it remains at 350 mL. What will you do? a. Replace 300 mL of aspirate and decrease rate by 50 mL/hr b. Replace all the aspirate and maintain current feeding rate c. Replace 300 mL of aspirate and decrease rate by 25 mL/hr d. Do not replace aspirate and hold tube feeds Use the Gastric Feeding Flowchart to find the answer. The correct answer is c. As the previous residual volume measurement was greater than 300mL, replace 300 mL of aspirate, discard the remainder and reduce rate by 25 mL/hr 4 He has remained stable throughout Day 3. On Day 4 of his admission the surgical team informs you at 1000 hr that they will be taking him back to the OR; they request that he be kept NPO after 2400 hours. Questions: 5. The dietitian has determined that his daily volume goal is 1200 mL in 24 hours (starts at 0700h daily) which is a rate of 50 mL/hr. What will be his new rate to reach his goal volume by midnight? a. 64 mL/hr b. 75 mL/hr c. 82 mL/hr d. 96 mL/hr Did you calculate 75 mL/hr? Since he needs to be NPO at midnight all of his feed volume needs to be infused by midnight, or in 17 hours total. He has received 150 ml since 0700: 50 mL/hr x 3 hours. 1200 – 150 = 1050 mL remaining. 1050 mL/14 hours remaining = 75 mL/hr Note that you can also refer to the EN Guideline for Surgical Procedures in order to minimize interruptions such as this one. 6. What is the maximum hourly rate that you should infuse on volume based feeding? a. 125 mL/hr b. 135 mL/hr c. 150 mL/hr d. 160 mL/hr Refer to the Volume Based Feeding Schedule to find the answer to this question. The maximum rate is 150 mL/hr. 5 7. Your 24- hour intake indicates that he received 1100 mL in the last 24 hours. Based on the daily goal of 1200 mL in 24 hours, what will you report as his nutritional adequacy during morning rounds? a. 92% b. 94% c. 96% d. 98% Part of your daily report in rounds should now include nutritional adequacy. This reports how much of the feed your patient received in the previous 24 hour period compared to what he/she should have received. This is reported as a percentage. Calculate nutritional adequacy by dividing the actual amount given by the target volume and multiplying x 100. Actual volume/target volume x 100 = % of target delivered In this question the calculation would be 1100/1200 x 100 = 92% 8. He continues to receive 5mg metoclopramide as per the enteral feeding initiation orders. But his gastric residuals have been > 300 ml for 2 consecutive checks. What intervention do you anticipate? a. Consider Erythromycin 200 mg Q12h b. Increase Metoclopramide to 10 mg q4h c. Increase rate of feeds d. Hold feeds for 4 hours Refer to the Gastric Feeding Flowchart to find the answer to this question. The correct answer is a. consider erythromycin. 6 One week following his admission he is scheduled for an MRI at 1400 hr. The enteral feeds are stopped from 1400 hr to 1700 hr. (N.B. In this example the flow sheet start time is 0700 hr). Questions: 9. You know that he is to receive 1200 mL in 24 hours which is a rate of 50 mL/hr. Upon returning to the ICU at 1700 hr, what will be his new rate based on the 24 hour volume protocol ? a. 60 mL/hr b. 65 mL/hr c. 70 mL/hr d. 75 mL/hr Did you calculate the correct rate of 60 mL/hr? If not, here is how you would calculate the rate: 50 mL/hr x 7 hours = 350 mL delivered by 1400 hr. 1200 mL/24 hours – 350 mL= 850 mL remaining 850 mL/14 hours remaining = 60 mL/hr Now that you have worked through the first set of questions there is a second case study below. To encourage you to test your new knowledge of the PEPuP protocol, the answers to this study are found at the end rather than along with each question. See how you do! 7 Case Study # 2 73 year old male is admitted to ICU at 2100 hours with a three day history of shortness of breath and weakness. He is in respiratory distress with oxygen saturations of 88% on 15 liters with a respiratory rate of 36/min. He is intubated and placed on FiO2 of 50%, PEEP 15 and PSV of 12. His saturations have improved and his respiratory rate is 14/min. His past medical history is significant for COPD and alcohol dependence. He is admitted to ICU with a diagnosis of community acquired pneumonia. He does not have bowel sounds and is NPO. His weight is 75Kg and height is 1.8m. N.B. In this example the flow sheet start time is 0700h Questions: 1. What do you anticipate will be ordered for feeding on admission? a. NPO because no bowel sounds b. Volume based feeding because he is not receiving any vasopressors c. Start trophic feeds at 10 mL/hr d. Start metoclopramide and wait for bowel sounds 2. Does he require protein supplements? a. Yes. He requires protein supplements because we want to avoid a nutrition deficit. b. No. Protein supplements are not required because he is a new admission. The resident orders volume based feeds for him because he is adequately volume resuscitated and is not receiving vasopressors. It is now 2200 hr and you need to initiate feeds. His weight is 75 kilograms. (Remember, the 24 hours begin and end at 0700 hr daily.) Questions: 3. At what hourly rate should feeds be initiated on day 1? a. 25 mL/hr b. 46 mL/hr c. 10 mL/hr d. 92 mL/hr 8 4. At 0700 hours you will recalculate the hourly enteral feeding rate for the next 24 hours, or until he is reassessed at rounds. What will this rate be? a. 46 mL/hr b. 62mL/hr c. 67 mL/hr d. 70 mL/hr Admission day 2: He continues to receive volume based feeds per PEPuP protocol. He has developed diarrhea and is having 6-7 loose stools per day. Question: 6. Which of the following would be an appropriate action? a. Stopping the tube feeds b. Stopping the metoclopramide c. Implement the diarrhea management guidelines d. Increasing the tube feeding rate The dietitian reassesses the patient and recommends that he receives 1500 mL over 24 hours. The feeds were stopped while going for a test and were not started upon return to the unit. At 1700 hours the feeds have been off for 4 hours. Question: 7. What rate will you run the feeds for the remainder of the time? a. 62 mL/hr b. 75 mL/hr c. 80 mL/hr d. 115 mL/hr Congratulations, you have completed the Learning Module! Thank you for helping us implement the PEPuP Protocol. 9 Answers: Case study 2 1. What do you anticipate will be ordered for feeding on admission? Answer: Volume based feeding because he is hemodynamically stable 2. Does he require protein supplements? Answer: Yes. He requires protein supplements because we want to avoid a protein deficit. 3. At what rate should feeds be initiated on day 1? Answer: For day 1 only, feeds should be initiated at 25mL/hr. On subsequent days, calculate the rate by dividing the 24-hour volume goal by the number of hours left in the day. 4. At 0700 hours you will recalculate the hourly enteral feeding rate for the next 24 hours, or until he is reassessed at rounds. What will the new rate be? Answer: 1100 ml 24 hr target volume 24 hrs = 46 ml/hr 5. Which of the following would be an appropriate action? Answer: Implement the diarrhea management protocol 6. At 1700 hours the feeds have been off for 4 hours. What rate will you run the feeds for the remainder of the time? Answer: 80 ml/hr 1500ml/24 hr = 63 ml/hr. 63 x 6 hr = 378 ml infused. 1500 – 378 = 1122 ml remaining to be infused. 1122 ml/14 hr = 80 ml/hr 10