Concurrent Enrollment Form
advertisement

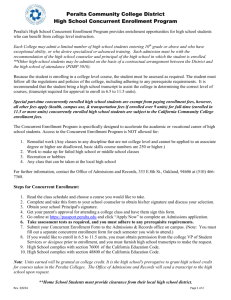
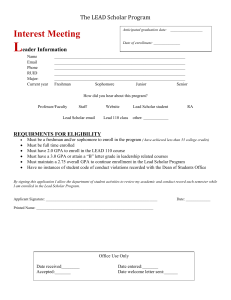
International Student and Scholar Services Request for Concurrent Enrollment Form A. To Be Filled Out By Student: Last Name First Name Student ID# Email Address Phone Number Birth Date Degree (BS, BA, MS, JD, PhD) Major Do you have a previous request for concurrent enrollment? Y / N Please initial: _____ The combined credits for which the student is enrolled are the equivalent of a full course of study during all required terms for your degree. Failure to maintain full time enrollment will result in termination of the student’s F-1 visa status and subject you to deportation. _____ Official transcript proving completion of the courses at the concurrent school listed above must be submitted to the International Student and Scholar Services within two weeks after the end of the semester. _____ Students using concurrent enrollment must take courses which apply to the student’s degree plan. Consult with your academic advisor. _____ Must be in good status. _____ The student must be enrolled [taking classes] at StMU during required terms for your degree. StMU must issue and maintain the SEVIS I-20, handle all SEVIS reporting requirements, and ensure that the student is pursuing a full course of study. _____ The StMU ISSS Office will issue a new I-20 documenting the concurrent enrollment, based on evidence that the student's enrollment in both institutions is the equivalent of a full course of study. The name of the other (concurrent) school where you are enrolled must be clearly recorded in the remarks section (page 1, item 9) of your I-20. _____ If you decide to enroll at a different institution for concurrent enrollment, you are required to notify ISSS. In such case, you must submit the concurrent form again. I have read and understand the above responsibilities. Student’s Signature Date (Don’t forget to fill out page 2) __________________________________________________________________________________________________ Please Return To: Office of International Students and Scholar Services Chaminade Tower, Ground Floor Room 105 210-431-5091 Revised: January 2014 Page 2 B. To Be Completed By Academic Advisor: Above named student will enroll in the following courses at: College/ University Class Start Date Course # Course Title Please check: The student is taking prerequisite courses The required course is not available at StMU ______ Academic Advisor (Print Name) Academic Advisor’s Signature ______ College/ Department Date C. Designated School Official Signature: Approved Print Name ______________ ______ Signature _________ Denied __________________________ Date __________________________________________________________________________________________________ Please Return To: Office of International Students and Scholar Services Chaminade Tower, Ground Floor Room 105 210-431-5091 Revised: January 2014