Khan
advertisement

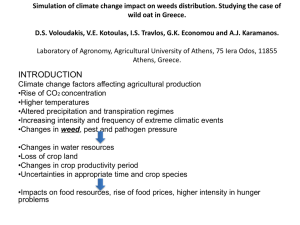
COMPARISON OF SEMI-AUTOMATED METHODS TO QUANTIFY INFARCT SIZE AND MYOCARDIAL SALVAGE BY CARDIAC MRI AT 1.5T AND 3.0T FIELD STRENGTHS Khan JN1, Nazir S1, Horsfield MA1, Singh A1, Kanagala P1, Greenwood JP2, Gershlick AH1, McCann GP1 (Affiliations: 1Department of Cardiovascular Sciences, University of Leicester and the NIHR Leicester Cardiovascular Biomedical Research Unit, Glenfield Hospital, Groby Road, Leicester, UK, LE3 9QP. 2Division of Cardiovascular and Diabetes Research, Leeds Institute of Genetics, Health and Therapeutics, University of Leeds, LS2 9JT.) Introduction: There is no consensus on the optimal method of quantifying infarct size (IS) on late gadolinium imaging (LGE) or area at risk (oedema, [AAR]) on T2-weighted STIR (T2wSTIR) in patients with ST-segment elevation myocardial infarction (STEMI). Semi-automated standard deviation (SD) based techniques, manual contouring of enhancement, and full-width half-maximum (FWHM) methods are used. Otsu’s Automated Thresholding (OAT) automatically identifies areas of enhancement by selecting the signal intensity threshold giving minimal intraclass variance within enhanced and normal myocardium and is user-independent. There are only 2 published studies using OAT quantification, of IS and AAR. There are no published studies using OAT at 3.0T, of reproducibility of OAT-based AAR or using OAT to calculate MSI. We aimed to compare the accuracy and reproducibility of IS, AAR and myocardial salvage index (MSI) quantification on LGE and T2w-STIR imaging using OAT with currently used methods at 1.5T and 3.0T in acute STEMI. Methods: Ten patients were assessed at 1.5T and 10 at 3.0T. IS was assessed on LGE using 5 standarddeviation thresholding (5SD), FWHM and OAT quantification. AAR was assessed on T2w-STIR using 2SD and OAT. Accuracy was assessed by comparison with manual quantification by an SCMR Level 3 trained reader. Inter-observer and intra-observer variabilities were assessed using Intraclass Correlation Coefficients and Bland-Altman analysis. Results: FWHM-derived IS closely correlated with manual assessment and had excellent inter-observer and intra-observer reproducibilities. 5SD and OAT overestimated IS. OAT overestimated AAR and 2SD demonstrated a trend towards overestimation (Figure 1). MSI quantified using 2SD and OAT-derived AAR was similar. AAR and MSI quantification using OAT demonstrated a trend towards better reproducibility versus 2SD, which was significant at 3T. Conclusions: FWHM-based assessment of IS is accurate and reproducible, whereas 5SD and OAT overestimate IS. OAT-based assessment of AAR and MSI has similar accuracy but with a tendency towards better observer agreement compared with 2SD thresholding in acute STEMI. ------------------------------Figure 1: Top row: IS and AAR on a patient at 3.0T showing progressively increasing IS using FWHM, 5SD and OAT. Bottom row: AAR in the same patient using OAT was greater than on 2SD thresholding at 3.0T, and was similar for patients studied at 1.5T.