Hemochromatosis
10% of the dietary iron is absorbed and used in physiological functions, such as the
production of hemoglobin, a carrier of oxygen in the bloodstream. Iron cannot be
excreted from the body and when excess iron is absorbed (up to 30%) it accumulates
and is stored in various tissues and organs resulting in a condition termed
Hemochromatosis.
Hereditary hemochromatosis (HH) is a genetic disease that causes the body to absorb
and store too much iron. It is the most common cause of iron overload. Other nonhereditary or secondary (acquired) causes of increased iron levels include frequent
blood transfusion, anemia, thalassemia or liver disease.
Symptoms of Hemochromatosis
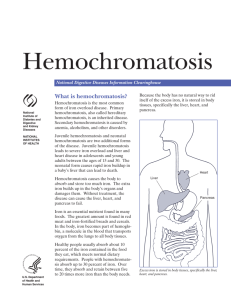
The symptoms of hemochromatosis stem from the accumulation of iron in tissues and
organs such as the heart, liver, testes, and pancreas. This leads to iron overload and
end-organ damage. Men are typically diagnosed in their forties and fifties. Because of
iron loss due to menstruation, women are first diagnosed with hemochromatosis in
later decades.
During early onset of hemochromatosis nonspecific symptoms appear such as:
Arthritis
Fatigue
Abdominal pain
Loss of libido
Symptoms after advancement of hemochromatosis may include:
Heart abnormalities and heart disease
Enlarged liver; abnormal liver enzymes; liver disease; cirrhosis
Hypogonadism – underactive testes and ovaries; impotence in men and early
menopause in women
Diabetes
Enlarged spleen
Skin discoloration; “bronzing”
The levels of transferrin and ferritin, two iron-binding proteins, are measured to
identify iron overload. An individual with iron overload will have
Elevated transferrin-iron saturation
Elevated serum ferritin concentration
The onset and advancement of symptoms may be aggravated by dietary intake of iron,
alcohol consumption and infections.
Treatment
Because iron cannot be excreted from the body, dietary uptake of iron must be severely
limited. This includes avoidance of foods that are rich in iron or that aid in the
absorption of iron from the diet (e.g. red meat, sugary foods and beverages, alcohol,
vitamin C, mineral supplements, medicinal iron, uncooked shellfish). Removal of iron
from the body by removing blood from patients (phlebotomy) is a common and
effective procedure to reduce iron levels.
Genetics of Hemochromatosis
The most common type of hereditary hemochromatosis is Type 1 (HFE1), which is
caused by mutations in the HFE gene. A genetic test is available for the most common
type of hemochromatosis, which accounts for about 85% of cases in the United States.
However, only some of those who test positive will actually develop serious illness. The
other 15% of individuals with symptomatic hemochromatosis will have mutations not
in the HFE gene, but in other genes, which may be unknown or for which gene testing
isn't routinely available.
The HFE mutations are “recessive”. Each person has two copies of the HFE gene, one
inherited from each parent. An individual with two normal copies does not have HHC
(asymptomatic or unaffected). An individual who has one normal and one defective
copy of the HFE gene is asymptomatic (unaffected), but is a “carrier”.
What is the probability of having children with Hereditary Hemochromatosis?
For example, parents who are both carriers of a defective HFE gene have a 1 in 4 chance
(25%) of passing both defective versions of HFE to their children, who will be affected.
These parents have a 50% chance of producing children who are carriers of a defective
HFE, but who are unaffected. Carrier parents also have a 25% chance of producing
children who have two normal copies of HFE, are unaffected and are non-carriers.
The HFE gene provides the code for the production of the HFE protein, which sits on
the surface of cells, mainly in the liver and intestines. The HFE protein works with other
proteins to sense the levels of iron in the blood, and to regulate iron uptake and storage
in the body. When mutations occur in the HFE gene, the HFE protein may not function
properly, or it may not be produced altogether. As a result, the sensing and regulation
of iron levels in the blood, and storage of iron are disrupted. Too much iron is absorbed
from the diet and is stored in tissues and organs where it causes damage.
Proteins are comprised of linked building blocks called amino acids. The sequence of
amino acids in any protein is encoded in the DNA or genes of an individual. In
hemochromatosis defects in the gene result in the wrong amino acid being inserted into
a protein sequence, and therefore, a potential malfunction in that protein. The most
common mutations in the HFE gene that lead to HHC are C282Y and H63D, which
account for about 85% of the cases of hereditary hemochromatosis.
Epidemiology
About 11% of the Caucasian population is a carrier of the C282Y CFTR mutation. The
incidence of individuals with HHC (posses 2 copies of C282Y) is approximately 1 in 200
to 1 in 400. Carriers of the H63D HFE mutation represent approximately 27% of the
general Caucasian population. Individuals with HHC who have both C282Y and H63D
mutations (one in each copy of HFE) account for less than 1% of the cases. Among
African Americans 2.3% are carriers and 1 in 7000 have two defective copies of HFE.
The frequency of HFE mutations is significantly lower in Asian population, of which 1
in 1000 are carriers.
References and Resources
PubMed: Hereditary Hemochromatosis Current Literature
National Library of Medicine Genetics Home Reference: Hemochromatosis
GeneReviews: HFE-Associated Hemochromatosis
Online Mendelian Inheritance in Man (OMIM): HFE (OMIM #613609)
Resources for patients and families:
American Hemochromatosis Society
American Liver Foundation: Hemochromatosis
Iron Overload Diseases: Hemochromatosis
National Organization for Rare Disorders: Classic Hereditary Hemochromatosis
Neonatal Hemochromatosis Information Center
Iron Disorders Institute: Diet Recommendations for Hemochromatosis
 0
0