Amanda Breuer
advertisement

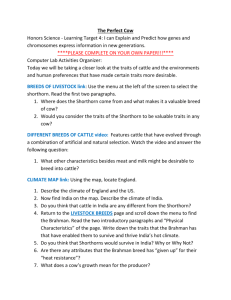
Vegetative valvular endocarditis and septicemia in a beef cow Amanda MH. Breuer Abstract – A Limousin beef cow was evaluated for progressive weight loss and poor doing following premature calving. Traumatic reticuloperitonitis was suspected and treated accordingly. The cow died two weeks following initial assessment and treatment. Post mortem examination revealed vegetative valvular endocarditis involving the left atrioventricular valve and ventricular wall. Case Description An 8-year-old Limousin beef cow presented for the evaluation of progressive weight loss and poor doing, 3 weeks following premature calving. Weight loss commenced in the 7th month of gestation and the cow gave birth to a premature but otherwise normal calf. Following calving, the cow continued to lose 200300 lbs over the course of three weeks, until at which point veterinary care was sought by the client. Physical examination revealed marked weight loss, an abnormal response to withers pinch, increased lung sounds, poor rumen motility and dry feces. A remnant of an old abscess on the skin overlying the left tuber coxae was noted. Slight favouring of the left hind foot was observed, which was consistent with a recent episode of footrot treated several weeks previously. The remainder of the physical exam was unremarkable. Traumatic reticulopericarditis (TRP) was suspected and a course of antibiotics, an antiinflammatory and a magnet were instituted as treatment. In response, the cow showed moderate signs of improvement, but deteriorated rapidly thereafter, resulting in death. A post mortem examination was performed 12 hours following death. The abdomen was explored and no discernable lesions consistent with TRP were evident; the diaphragm was clear of puncture wounds, fibrin and adhesions. In addition, no sharp objects were found in the rumen or reticulum. The magnet given previously was recovered from the reticulum and found to have minimal filings attached. A large amount of serous, amber coloured fluid was observed in the pleural space upon entry into the thorax. Severe pulmonary edema was present in the lungs and the lung tissue exuded fluid from the cut surface. The heart did not appear to be enlarged and had a normal right to left ventricular ratio of 1:3. Upon dissection a large, yellow, fibrous, vegetative mass approximately 4cm x 4cm x 5cm was found within the left ventricle, involving both the mitral valve and ventricular wall. The cut surface of the mass revealed a fibrinonectrotic center filled with purulent material. Tissue samples of the heart, vegetative mass, trachea, lung, uterus, spleen, liver and kidney were submitted for histopathology. Histopathology of the heart muscle revealed random multifocal areas of fibrosis throughout the myocardium and the Figure 1. Photograph of the vegetative mass found in the left ventricle involving the mitral valve and ventricular wall. endocardium was extremely thickened with maturing granulation and fibrous tissue. The vegetative mass on the affected valve was found to be composed of laminated fibrinonecrotic debris containing many bacterial colonies and scattered infiltrates of degenerate leukocytes. Colonies of bacteria and fibrin were present on the eroded surface of the lesion. The bronchoalveolar lumina in the diffusely congested and edematous lung contained variable amounts of proteinaceous edema. Mild and acute pulmonary hyaline membranes and alveolitis were also present. The kidney had mild to moderate multifocal interstitial fibrosis and showed small numbers of focally mineralized tubules. The liver sample displayed mild hepatic lipidosis, consistent with metabolic imbalance. The remaining tissues were markedly autolyzed and provided no other useful diagnostic information. Bacterial culture on samples of pleural fluid, mediastinal lymph node and purulent material within the mass revealed presence of Pseudomonas spp. A diagnosis of terminal septicemia and endotoxemia due to Pseudomonas spp., valvular endocarditis and myocardial fibosis in addition to mild hepatic lipidosis was made based on the post mortem and pathology reports. Discussion Bacterial endocarditis (BE) is a major cause of heart disease in adult cattle. However, it often goes undiagnosed or is frequently misdiagnosed in practice (1). BE may cause showering of bacteria from the heart and disseminated sepsis, in addition to being a potential cause of heart failure as a consequence of valvular insufficiency. In cattle, BE most commonly involves the tricuspid valve. However, the second site of predilection is the mitral valve (2). As seen in this case, the mitral valve was affected with BE due to Pseudomoas spp. colonization. Death was not a direct result of heart failure, as gross cardiac changes consistent with congestive heart failure were not evident. Instead, the histopathological report concluded death was the result of bacterial showering of Pseudomonas spp. from the vegetative lesion. Disseminated septicemia and endotoxemia from septic emboli originating from the vegetative lesion on the mitral valve lead to terminal, multi-organ failure. The clinical signs associated with heart disease resulting from BE are non-specific and infrequently observed in cattle (3). A systolic cardiac murmur, thrill, tachycardia, thoracic pain, intermittent or constant fever, polypnea, ill thrift, diarrhea, constipation and shifting lameness are all clinical signs which may be present but are not necessarily unique to BE. For a general practitioner in the field, auscultation of a cardiac murmur is the most specific clinical sign of BE, while the others listed are vague and may be present with other conditions common to cattle (1). This ambiguity of clinical signs ultimately interferes with obtaining an accurate diagnosis. For example, in a recent study, of 52 cows afflicted with endocarditis only 13 had an obvious murmur (4). Another previous study speculates that closer to half of cattle with BE will fail to have an auscultable murmur (5). Without a discernable murmur, a practitioner may fail to recognize BE as a differential diagnosis when performing an initial evaluation, and as a result, a misdiagnosis of pneumonia or TRP is frequently made. When a murmur is ascultated, ancillary tests such as echocardiography and a blood culture would permit a definitive diagnosis of BE to be made (6). In this case, both vague clinical signs similar to TRP and the absence of an auscultable heart murmur interfered with obtaining an accurate initial differential diagnosis of BE. A key component of the pathophysiology of BE is persistent bacteremia, which is often the result of a chronic septic process at a distant site in the body or a low-grade infection. Possibilities include, but are not limited to septic mastitis, chronic metritis, foot abscess, musculoskeletal abscessation, cellulitis, venipuncture of the jugular or milk vein, or the presence of an indwelling intravenous catheter for an extended period of time (5,7). Arcanobacterium pyogenes is one of the most commonly isolated pathogenic agents from endocardial lesions and/or blood (6). Other common isolates include -hemolytic streptococci, Arcanobacterium pyogenes, Corynebacterium pyogenes, Micrococcus and Staphylococcus spp., Clostridium chauvoei, Mycoplasma mycoides, Erysipelothrix rhusiopathiae and as seen in the case of this cow, Pseudomonas spp. In large animals, BE does not require pre-existing trauma to the cardiac endothelium to initiate the disease process of endocarditis. Instead, it is believed that the ability of some pathogens to adhere to normal endothelium in conjunction with persistent bacteremia can be sufficient cause (7). No direct inciting cause was identified in this case, however it is speculated the scar of a previously ruptured abscess observed over the tuber coxae is most probable. The other two possibilities of footrot and a metritis post-calving occurred after the initial onset of clinical signs, and can therefore be excluded from the possible causes. The cow likely became bacteremic with Pseudomonas spp. as a result of the ruptured abscess, resulting in the colonization of the mitral valve and the development of valvular BE. Treatment options for those cases of BE that are diagnosed ante-mortem are limited by both feasibility and economics. The minimum length of recommended antimicrobial treatment is 21 days, but is often prolonged past 4 weeks (6). When developing a treatment regime, blood culture and sensitivity is recommended. An appropriate antimicrobial providing high concentrations in the serum relative to the minimum bactericidal concentration should be selected based on culture and sensitivity results (7). Inadequate antibiotic distribution and activity within the lesions as the result of thick fibrous tissue and pyonecrotic debris are likely to be problematic in regards to treatment efficacy (1,7). Not only the quantity of drug required for treatment, but also the difficulty of administering treatment to animals, such as beef cattle, over a prolonged period of time often makes treatment impractical for clients. However, an exception may be made in some cases where the animal is of particular value. In addition, the prognosis for animals with BE is generally guarded to poor, despite attempted treatment, as most cases are identified and diagnosed late in the course of the disease. (7). Marginal improvement of prognosis with early diagnosis and early initiation of treatment has been documented. Ultimately, informed clients often opt for euthanasia or salvage for slaughter rather than a course of treatment due to the high financial cost, length of treatment and the overall guarded to poor prognosis associated with BE (1). In the case of this cow, diagnosis of BE was not obtained in a timely manner, and a treatment regime specific to BE was not an option. This case emphasizes the challenges which can complicate diagnosing BE in the field. Often clinical signs are non-specific making a definitive diagnosis difficult to obtain. Regardless of a timely diagnosis and treatment, the prognosis and practicality of treating cases of BE is an additional challenge, as prognosis remains guarded to poor, and is additionally complicated by finances. 3. 4. Acknowledgements The author would like to thank Dr. Reg Clinton for his guidance, and Dr. Charlotte Winder and Dr. Katharine Found for their support. 5. 6. References 1. 2. Dowling PM, Tyler JW. Diagnosis and treatment of bacterial endocarditis in cattle. J Am Vet Med Assoc 1994;204:1013-1016. Reef VB, McGuirk SM. Diseases of the cardiovascular system. In: Smith BP, ed. Large Animal Internal Medicine. 7. 4th ed. St. Louis, Missouri: Elsevier-Saunders, 2008:453– 489. Buczinski S, Rezakhani A, Boerboom D. Heart disease in cattle: diagnosis, therapeutic approaches and prognosis. Vet J 2010;184:258-263. Bexiga R, Mateus A, Philbey AW, et al. Clinicopathological presentation of cardiac disease in cattle and its impact on decision making. Vet Rec 2008;162:575–580 Power HT, Rebhun WC. Bacterial endocarditis in adult dairy cattle. J Am Vet Med Assoc 1983;182:806-808. Divers TJ, Peek SF. Cardiovascular Diseases. In: Rebhun’s Diseases of Dairy Cattle 2nd ed. St. Louis, Missouri: Elsevier-Saunders, 2008: 53-56. Radostits OM, Gay CC, Hinchcliff KW, et al. Diseases of the cardiovascular system In: Veterinary medicine – a textbook of the diseases of cattle, horses, sheep, pigs and goats 10th ed. Philadelphia: Elsevier-Saunders, 2007: 42443.