Private Hospital Day Program Flyer & Referral Form
advertisement

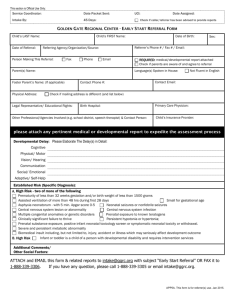
Day Program Our Royal Rehab Private Hospital Day Program specialises in: Stroke recovery Neurological Orthopaedic Post-spinal surgery Reconditioning rehabilitation. Our program is ideal for those with rehabilitation goals not requiring overnight inpatient nursing and medical care. We offer the following individually tailored high-intensity therapy programs in modern state-of-the-art facilities: Hydrotherapy Clinical Psychology Orthopaedic Clinic Dietetics Communication Group Stroke Survivors Exercise Physiology Cognitive Group Falls Prevention Occupational Therapy Energy Conservation Neuro Clinic Nursing Relaxation Physiotherapy Upper Limb Group Social Work Recreational Therapy Speech Pathology The duration of the Day Program is determined by a multidisciplinary treating team under the direction of a rehabilitation specialist and consists of either full or half-day therapy sessions. We also offer sessional therapy to clients requiring a single mode of therapy. Therapy groups are capped at a maximum of eight patients per clinician and all individual sessions are oneto-one. Cost: Varies depending upon level of private health insurance cover. Eligibility: Royal Rehab Private Day Program Referral form (refer to other side) or doctor’s referral letter. Day Program 235 Morrison Road Ryde NSW 2112 PO Box 6 Ryde NSW 1680 E. referrals@royalrehab.com.au T. (02) 9808 0527 F. (02)8088 4316 Day Program Referral (PDPR.615) MRN _________________ GIVEN NAME _______________________ MALE DoB _______/_______/_______ FEMALE M.O.____________________________ ADDRESS ___________________________________________________ 235 Morrison Road, Ryde NSW 2112 PO Box 6, Ryde NSW 1680 E. referrals@royalrehab.com.au F. (02) 8088 4316 BARCODE FAMILY NAME _____________________ _____________________________________________________________ LOCATION/WARD __________________________________________ COMPLETE ALL DETAILS OR AFFIX CLIENT LABEL HERE Date of Referral: _______________________________________ Discharge Date (if applicable): ________________________ Patient Details Name: _____________________________________ DOB: ________________ Tel: _________________________________________ Address: __________________________________________________ Interpreter required: Yes / No Binding Margin – No Writing Next of Kin: _______________________Relationship:______________ Tel: ______________________________________________ Health Fund: ____________________________ Membership No: ___________________________________________ Workcover / CTP / DVA: _____________________ ____________________ Claim No: ___________________________________ Referrer Details: Referrer’s Name: ____________________ Facility: ____________________ Tel: _________________________________________ Specialist/Surgeon/GP: __________________________________________ Tel: _________________________________________ Primary Diagnosis: Operation Date: / / Weight Bearing Status: ______________________________________ __________________________________________________________________________________________________________________ Relevant Medical History (including Allergies/ Alerts: _____________________________________________________ __________________________________________________________________________________________________________________ Current Status: Cognition: _____________________________________________________________________________________________________ Communication: ______________________________________________________________________________________________ Day Program Goals / Reason for Referral: __________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________ Services required: (minimum of 3 sessions; 3-5 sessions =half day; 5+sessions = full day) Requested duration of program: _________________________________days/weeks Days that patient is unavailable to attend: Mon am/pm, Thur am/pm, Fri am/pm INDIVIDUAL THERAPIES Therapies Duration (min) GROUP THERAPY Frequency Classes Clinics Clinical Psychology 30 / 60 Hydrotherapy Ortho Clinic Dietetics 30 / 60 Communication Group Stroke Survivors Exercise Physiology 30 / 60 Cognitive Group Falls Prevention Occupational Therapy 30 / 60 Energy Conservation Neuro Clinic Nursing 30 / 60 Relaxation Physiotherapy 30 / 60 Upper Limb Group Social Work 30 / 60 Recreational Therapy 30 / 60 Speech Pathology 30 / 60 NO WRITING Private Day Program Referral Binding Margin – No Writing Mobility/Transfers: ___________________________________________________________________________________________