Binge eating in binge eating disorder: A breakdown of emotion regulatory process?
Simone Munsch a,⁎, Andrea H. Meyer b, Vincent Quartier a, Frank H. Wilhelm c
a
b
c
University of Fribourg, Department of Psychology, 2, Rue de Faucigny, CH-1700 Fribourg, Switzerland
University of Basel, Faculty of Psychology, Department of Clinical Psychology and Psychotherapy, Division of Applied Statistics in Life Sciences, Missionsstrasse 62a, CH-4055 Basel, Switzerland
University of Salzburg, Institute of Psychology, Department of Clinical Psychology, Psychotherapy, and Health Psychology, Hellbrunnerstrasse 34, A-5020 Salzburg, Austria
a b s t r a c t
Current explanatory models for binge eating in binge eating disorder (BED) mostly rely on models for bulimia
nervosa (BN), although research indicates different antecedents for binge eating in BED. This study
investigates antecedents and maintaining factors in terms of positive mood, negative mood and tension in a
sample of 22 women with BED using ecological momentary assessment over a 1-week. Values for negative
mood were higher and those for positive mood lower during binge days compared with non-binge days.
During binge days, negative mood and tension both strongly and significantly increased and positive mood
strongly and significantly decreased at the first binge episode, followed by a slight though significant, and
longer lasting decrease (negative mood, tension) or increase (positive mood) during a 4-h observation period
following binge eating. Binge eating in BED seems to be triggered by an immediate breakdown of emotion
regulation. There are no indications of an accumulation of negative mood triggering binge eating followed by
immediate reinforcing mechanisms in terms of substantial and stable improvement of mood as observed in
BN. These differences implicate a further specification of etiological models and could serve as a basis for
developing new treatment approaches for BED.
1. Introduction
The core feature of binge eating disorder (BED) comprises loss of
control and consumption of large amounts of food (American
Psychiatric Association (APA), 1994). Cognitive behavioral therapy
(CBT) approaches in BED are traditionally based on corresponding
models for bulimia nervosa (BN) and constitute the established
treatment for the majority of BED patients (Vocks et al., 2009). In BN,
negative mood has been shown to be an important antecedent by a
number of studies (Polivy et al., 1984; Agras and Telch, 1998; Waters et
al., 2001). According to the affect regulation model, individuals engage
in binge-purge behavior to alleviate negative mood (Polivy et al., 1984)
or by substitution of a less aversive mood state (trade off-theory,
Kenardy et al., 1996). Masking theory suggests that rather than
decreasing or substituting negative mood, binge eating serves as an
attribution for negative mood that masks other problems (Herman and
Polivy, 1988). In other words, negative affect can be blamed on binge
eating, which seems to be more controllable to the person than the
actual causes of distress. The escape theory (Heatherton and Baumeister, 1991) posits that binge eating represents an attempt to “escape”
from distressing self-awareness and to narrow attention to the
immediate physical surroundings or stimuli (e.g. food). As a secondary
effect, the hypothesized shift in awareness impedes higher level
⁎ Corresponding author at: University of Fribourg, Department of Psychology, 2, Rue
de Faucigny, CH-1700 Fribourg, Switzerland.
E-mail address: simone.munsch@unifr.ch (S. Munsch).
0165-1781/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.psychres.2011.07.016
cognitive activities such as inhibition and thus results in the release of
previously suppressed binge eating behavior (Engelberg et al., 2007).
Recent studies using ecological momentary assessment (EMA) to
overcome known limitations of retrospective recall (for an overview,
see Shiffman et al., 2008) convincingly demonstrate that, in line with
the affect regulation model, negative mood increases and positive
mood decreases before binge eating and vomiting, whereas after BN
events, negative mood decreases and positive mood increases again.
Binge-purge behavior in BN thus seems to be reinforcing itself by
improving mood (Engel et al., 2006; Smyth et al., 2007; Engelberg et
al., 2007). Another study from Crosby et al. (2009) investigating
patterns of mood in daily lives of bulimic individuals corroborates that
negative mood drives bulimic behavior.
Research regarding antecedents of binge eating in BED used to rely
on models derived from BN, although there seem to be differences with
regard to the binge cycle. For example, Hilbert and Tuschen-Caffier
(2007), in a comparison of BED with BN patients using EMA for multiple
assessments over a 2-days period found, that BED individuals not only
reveal less dietary restraint, they also experience less intense negative
mood than BN patients and tend to binge eat also when feeling only
moderately negative. Further, BED in contrast to BN individuals turned
out to be vulnerable to negative mood, in particular when they
concurrently suffered from high levels of general psychopathology
(Hilbert and Tuschen-Caffier, 2007). Together with another naturalistic
study from Stein et al. (2007) assessing antecedents and consequences
of binge eating at 7 intervals during 7 consecutive days, these findings
underline that also in BED negative mood was increased on binge eating
S. Munsch et al. / Psychiatry Research 195 (2012) 118–124
days compared to non-binge periods, whereas there were no such
differences for ratings of positive mood. On both studies, however,
contrary to existing emotion regulation models, negative mood
remained increased when measured immediately after binge eating in
student and patient populations (Hilbert and Tuschen-Caffier, 2007;
Stein et al, 2007). The cited studies shed light on possibly different
mechanisms driving binge eating in BED, but their findings remain
limited as they did not consider longer time intervals than one
measurement immediately after binge eating. As a consequence, the
time course of mood factors after binge eating in BED remains open.
Further limitations of the earlier studies concern the application of
solely the time-contingent sampling method of the Stein et al. study as
well as the short observation method of 2 days in the Hilbert et al. study.
In summary, current research about the preceding and maintaining
factors of binge eating in BED indicates distinct processes such as less
pronounced negative mood and a lack of immediate reinforcement in
terms of a fast and pronounced decrease of aversive mood states after
binge eating in BED. Thus, research on the concrete cues and reinforcing
mechanisms of binge eating in BED may help to further specify
etiological models and to engage in developing specialized and
individualized treatment options for BED patients.
The present study aims at extending findings of current naturalistic
studies regarding binge cycles in BED and sets out to investigate in more
detail the binge cycle in BED. Besides negative mood, we additionally
included potentionally meaningful mood factors such as positive mood
and tension. We followed the temporal course of these characteristics
before, during, and after binge eating on binge and, for comparison, on
non-binge days in a small sample of overweight to obese female BED
individuals randomized for participation in a treatment trial for BED. To
minimize influences of retrospective memory recall, participants were
investigated using ecological momentary assessment (EMA). Relative to
traditional questionnaire-based methods, EMA reduces biases associated
with retrospective recall by shortening the interval between an
experience and its recall. Further the EMA method is thought to enhance
ecological validity as it is carried out within the naturalistic environment
of the participant (Shiffman et al., 2008).
The following research questions were investigated: First, we
examined whether the daily courses of the different aspects of mood
varied between binge and non-binge days. Second, to shed light on
binge cycles in BED, we not only examined the pre- but also the postbinge phase. To our knowledge, we are the first to examine
consequences of binge eating not only immediately after but during a
prolonged time span during the day after binge eating. Third, according
to Smyth and colleagues, we further acknowledge that the binge eating
event itself is affect-laden and probably influences estimates recalled
immediately after binge eating. Therefore, we analyzed the trajectories
of mood and tension by including or excluding the 30 min immediately
prior to and the 30 min following the binge episode (Smyth et al., 2007).
Fourth, to account for findings in the current literature (e.g., Hilbert and
Tuschen-Caffier, 2007), we additionally included specific participant
characteristics related to eating disorder and clinical features, i.e.
comorbidity status, body-mass index (BMI), duration of the disorder,
degree of depressiveness and severity of eating disorder pathology,
which may all potentially moderate the temporal trend of negative
mood, positive mood, and tension on binge eating days.
2. Methods
119
Psychiatric Association (APA), 2000) according to a specialized eating disorder
interview (see diagnostic assessment below). Of the 136 individuals who were initially
contacted, 28 female obese individuals with BED fulfilled these inclusion criteria. As
individuals participated in a randomized trial to evaluate treatment efficacy of a shortterm CBT approach, individuals were excluded if they were pregnant, participated in a
diet or psychotherapy, received weight loss medications (currently or during the last
3 months), had previous surgical treatment of obesity, or met DSM-IV-TR (American
Psychiatric Association (APA), 2000) criteria for mental disorders warranting
immediate treatment, as those factors might have influenced treatment response. As
patients who never exhibited a binge during the entire week were excluded from all
analyses (see results section), the final sample consisted of 22 female obese individuals
with an average age of 45.5 years (S.D. = 12.0, range = 21–65), a BMI (kg/m 2) of 33.4
(S.D. = 6.8, range = 24.4–55.5), a Beck Depression Inventory score of 12.8 (S.D. = 8.7,
range = 3–32), an Eating Disorder Examination (EDE) total score of 2.43
(S.D. = 0.86, range = 0.93–4.22), an average number of binges according to EDE of
15.6 (S.D. = 8.0, range = 4–30), and an average age of first manifestation of BED of 16.6
(S.D. = 12.2, range = 2–40). Six (27%) participants suffered from an additional affective
or anxiety disorder and one patient (3.6%) from a comorbid mental disorder on axis-II.
As only one male participant could be recruited, we excluded these data from our
analyses.
2.2. Measures and procedure
2.2.1. Diagnostic assessment
BED diagnosis and associated eating disorder pathology were assessed using the
Eating Disorder Examination (EDE, Fairburn and Cooper, 1993; Hilbert et al., 2004). The
German language screenings for mental disorders on axis-I (Mini-DIPS) (Margraf,
1994) and axis-II (SKID-II) (Wittchen et al., 1997) were administered to assess current
and lifetime mental disorders. Interviewers were trained by the principal investigator
(S.M.). In cases of discordance of interviewers regarding the diagnoses, the diagnostic
process was reevaluated using video tapes of the diagnostic interviews.
2.2.2. Daily electronic diary, ecological momentary assessment (EMA)
All patients gave written informed consent and were offered free treatment. Data
were collected for 7 days before treatment onset using a personal digital assistant (PDA,
Palm Tungsten E). According to Smyth et al. (2007), time-contingent assessment
intervals were decreased during the day to adjust for an increased likelihood of binge
eating in the evening. Time intervals were scheduled as follows: The first alarm was
preset individually at 1.5 h after awakening, the second alarm 5 h after the first, the
third alarm 4 h after the second, the fourth alarm 3 h after the third and the fifth alarm
2 h after the fourth alarm. For event-contingent monitoring, participants were
instructed to fill in the questionnaire whenever binge eating occurred. Participants
were asked to fill in the questionnaire within a 30-min interval. Please refer to Munsch
et al., (2009) for further details including test-theoretical characteristics of the
questionnaires used in this study. Questions were either dichotomous, suggesting a yes
or no response, e.g., item 1 “Did you experience binge eating since your last entry?”, or
corresponded to a computerized Likert-type or visual analogue scale (VAS) scale.
Questionnaires were programmed and displayed using Pendragon Forms software
(Pendragon Software Corporation, Libertyville, IL, USA; unpublished questionnaire
available from the authors). Feasibility of EMA, i.e. practicability (“Did you experience
any difficulties in filling in the electronic diary?”), acceptability (“How did you feel
during the week with the electronic diary entries?”, “Did the electronic diary alarm go
off too often?”, “Was your daily routine disturbed?”; correlations among items were
between 0.47 and 0.72; mean = 7.19, S.D. = 2.24, N = 20), representativeness (“Did the
previous week correspond to your usual weekly routine?”; mean = 7.21, S.D. = 2.55,
N = 17), and signal-compliance (“Was it possible for you to fill in the electronic diary
30 min after the signal?”; mean = 7.05, S.D. = 2.28; Fahrenberg (2006)) were all
measured on an 11-point Likert-type scale from 0 (“not at all”) to 10 (“yes, exactly”)
according to a self-developed exit questionnaire, EXQ (Munsch et al., 2009). EMAbased signal-compliance (filling in of the electronic questionnaire within 30 min after
being alarmed) and recording compliance (rate of overall responses to time-contingent
signaling) were all assessed by EMA. Reactivity was registered according to the EXQ
(“Did the frequency of binge eating change during the diary period?”, “Did you focus
more on your psychological well-being?”, “Did you benefit from filling in the diary?”,
“Did the previous week correspond to your usual weekly routine?”; correlations among
items were between 0.48 and 0.70; mean of averaged items = 5.72, S.D. = 3.29, N = 16;
for detailed information see Munsch et al., 2009). EMA-based signal-compliance, i.e. the
proportion of the number of recordings starting within 30 min after the signal to the
total number of recordings was 0.87. Participants' mean absolute deviation of entry
from the scheduled alarms (in min) was 16.0 (median = 1.0, S.D. = 34.8, N = 722).
2.1. Participants
Data were collected from obese individuals with BED presenting for participation in a
treatment trial to evaluate the efficacy of a short version of a cognitive behavior
therapy (CBT) trial at the Department of Clinical Psychology and Psychotherapy of the
University of Basel (Switzerland) (Schlup et al., 2009). The study was approved by the
local ethics committee of the University Hospital of Basel. Inclusion criteria for the
clinical trial included being aged between 18 and 70 years, having a BMI between 27
and 40 kg/m 2, being free from severe medical conditions such as diabetes, heart
disease, or endocrine disorders and meeting full DSM-IV-TR criteria for BED (American
2.2.3. EMA of binge eating, negative and positive emotions
After answering the electronically administered entry question (“did you
experience a binge episode”) with yes, exclusively objective binge eating (OBE, i.e.
binge eating defined as consuming unusually large quantities of food with a subjective
sense of loss of control) was assessed according to the German version of the EDE
(Hilbert et al., 2004; Munsch et al., 2009) (for a critical discussion of concordance rates
of EMA-based and self-report-based measures in order to assess binge eating in BED,
please see Munsch et al., 2009). Daily course of negative mood, positive mood, and tension
were assessed on a scale between 1 and 10 using the Mood Assessment Inventory (MAI,
120
S. Munsch et al. / Psychiatry Research 195 (2012) 118–124
German version by Feist and Stephan, 2007) developed for ambulatory assessment,
which contains five empirically derived subscales: negative mood, positive mood,
interest, tension, and sleepiness. Feist and Stephan (2007) reported sufficient
correlations (r = 0.60) of the Negative Mood Subscale with the Beck Depression
Inventory (BDI, Beck et al., 1961; Hautzinger et al., 1995) and good test–retest
reliability (r = 0.70) in a student sample. Based on clinical experience and literature on
mood in BED (Stickney and Miltenberger, 1999; Vanderlinden et al., 2001; Binford et al.,
2004; Engel et al., 2006; Smyth et al., 2007), we additionally included the following
adjectives in the electronic questionnaire: bored, stressed out, anxious, sad, tense,
lonely, and annoyed.
To combine the items of the MAI with the additional items, and to obtain a limited
number of reliable, valid and interpretable measures of mood, all items were entered
into an exploratory factor analysis using principal components as extraction and
varimax as rotation method. Items with loadings b 0.4 were excluded from further
analyses. Based on the Scree plot and the Kaiser criterion (excluding components with
Eigenvalues b 1.0), we obtained three different factors. These factors represent scale
scores, i.e., they were computed by taking the mean across all items which loaded
highly on them. The first factor, which explained 10% of the variance, was highly
correlated with the MAI-scale “negative mood” (r = 0.92) and was given this label. It
contained the MAI items discontented, depressed, and queasy plus the additional items
bored, anxious, lonely, and sad. The second factor, which explained 39% of the variance
was highly correlated with the MAI scale “tension” (r = 0.94) and received this label. It
contained the MAI items calm, nervous, and agitated plus the additional items stressed
out, tense, and annoyed. The third factor, which explained 15% of the variance, was
highly correlated with the two MAI scales “positive mood” (r = 0.92) and “interest”
(r = 0.94) and was given the label “positive mood”. It contained the MAI items
cheerful/merry, good, and happy of the positive mood scale, and fascinated, interested,
and not interested of the MAI interest scale, with no additional items. Factor scores
based on these three factors were then used as mood-related variables in subsequent
analyses.
2.2.4. Situational context of binge eating
These were assessed by the two questions “where are you at the moment?” and
“whom are you with?”. Answers were recoded into the two variables “being at
home/not at home” and “being alone/not alone“.
2.2.5. Trait specific characteristics moderating the impact of mood and tension on binge
eating
To analyze the moderating impact of participants' characteristics related to eating
disorder and clinical features on temporal trends of positive or negative mood and
tension during binge days, we included the following baseline variables: comorbidity
status, baseline BMI, duration of BED (years since first manifestation of BED), severity of
eating disorder pathology (measured by the global score, GS, of the EDE), and
depressiveness (measured by the BDI, Hautzinger, 1991).
For the temporal trend during both the pre- and post-binge phase, we included only
linear polynomials as polynomials of higher degree did not improve model fit (see
Appendix A).
Finally, Model 4 tested whether BMI, EDE global score, comorbidity status (y/n),
number of years since first manifestation of BED, and depressiveness (BDI) moderated
the temporal trends of negative mood, positive mood, and tension before and after the
first daily binge as assessed in Model 2. This model therefore included in addition to the
terms listed in Model 2 the moderator (main effect) plus the interaction between
moderator and time for the pre- and post-binge phase. Each moderator was tested in a
separate model.
Note that in all four models we did not include an individual random slope coefficient
b1i (Singer and Willett, 2003) as doing so would not have improved model fits. Mood
factors for negative mood and tension were both transformed logarithmically (natural) to
meet model assumptions. To analyze these models, we used the software SPSS 14.
Reported significances are based on an alpha of 0.05 unless otherwise specified.
3. Results
Of the 28 patients, 6 never exhibited a binge during the entire
week and were excluded from all analyses. These six patients did not
differ from those reporting one or more binges during the study
period with respect to age, educational level, BMI, BDI, BAI, EDE total
score, first manifestation of BED (years), and number of binge
episodes according to EDE (p N 0.05 for each t-test performed). For
the remaining 22 patients filling in the diary five times a day during
the entire week, a total of 770 possible time-contingent data entries
were possible. They actually completed 651 records, corresponding to a
compliance rate of 85%. In addition, 36 event-contingent data entries
were recorded, resulting in a total of 687 data entries of which 75
(11%) concerned binge episodes. Each patient had on average 0.49
binge episodes per day.
Most binge episodes occurred in the afternoon (52%, 12:00–18:00,
N = 39) and in the evening (39%, 18:00–24:00, N = 29); very few
were observed during the night (4%, 24:00–06:00, N = 3) and in the
morning (5%, 06:00–12:00, N = 4). Models 2 and 4 covered only binge
days and thus included 198 records and Model 3 in addition excluded
all measurements within 30 min before and after a binge episode and
included 149 records.
3.1. Situational context of binge eating
2.3. Statistical analysis
We used a random intercept model to analyze the data (Pinheiro and Bates, 2000).
Random intercept models are special types of linear mixed models in which each
individual is assumed to have his/her own intercept. This kind of model is suitable for
cases where each subject follows his/her own time schedule (i.e. both the number of
time points and the time interval are allowed to vary from subject to subject) which is
often observed in EMA based studies. The distinction between binge days and nonbinge days was based on whether at least one daily binge episode occurred or not. For
the precise model equations, please refer to Appendix A.
Model 1 tested whether the daily course of mood factors differed between binge
and non-binge episodes while allowing for a trajectory following a linear and quadratic
polynomial.
Model 2 tested for temporal trends in the mood factors before and after the
occurrence of the first daily binge. Hence we introduced an additional dummy variable
distinguishing between the pre- and post-binge phase during binge days that allowed
us to model the temporal trends of these two phases independently. This model
contained the interactions between time and each of the two dummy variables pre- and
post-binge phase. For the temporal trend during the pre-binge phase, we included
polynomials up to 5th degree as doing so improved model fit. The inclusion of
polynomials higher than linear during the post-binge phase in contrast did not improve
model fit and we therefore only used a linear trend (see Appendix A for the exact model
equation). The variable time was centered to the first binge episode, separately for each
patient and day. For this analysis we used a subsample covering binge days only. We
omitted days starting with a binge episode as such cases could not have been analyzed
using Model 2 since there would have been no mood factor ratings preceding a binge
rating. This concerned 14 binge episodes stemming from 6 persons. We also omitted all
data points including and following the second binge episode within the same day as
the corresponding mood factor values might have been influenced by the first binge
episode. This concerned 16 binge episodes coming from 12 persons.
According to Smyth et al. (2007), we tested in Model 3 whether trends of values of
mood factors prior to the first binge could still be observed after excluding the values at
the binge themselves. Thus in this model the values covering the 30 min immediately
prior to and the 30 min following the binge episode were excluded to prevent
recordings immediately associated with the binge event influencing the model results.
The proportion of participants being at home rather than not at
home was 67% (N = 576) during non-binge periods, 83% (N = 29)
immediately before a binge episode and also 83% (N = 35) during a
binge episode. In the same way the proportion of participants being
alone rather than not alone was 46% (N = 576) during non-binge
periods, 72% (N = 29) immediately before a binge episode and 63%
(N = 35) during a binge episode.
3.2. Daily course of negative mood, positive mood, and tension (Table 1)
3.2.1. Model 1
Values for negative mood were significantly higher during binge
than non-binge days without showing any particular daily trend
during either binge nor non-binge days. Values for positive mood
were significantly lower during binge than non-binge days, especially
later during the day. However, no significant daily trends could be
found. Values for tension did not vary between binge and non-binge
days but increased during the day until the afternoon and then
decreased again, both during binge and non-binge days.
3.2.2. Model 2
The average time period between the first measurement in the
morning and the first reported binge episode was 7.23 h (S.D. = 3.29).
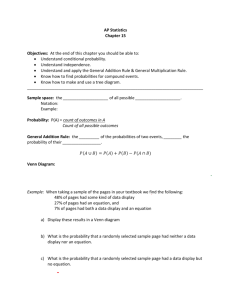
For negative mood, there was a significant curvilinear increase
immediately before the first binge episode, with particularly high
rates of increase shortly before the first binge (solid lines in Fig. 1a).
The linear post-binge trend was significantly negative. Positive mood
S. Munsch et al. / Psychiatry Research 195 (2012) 118–124
121
Table 1
Daily course of negative mood, positive mood and tension. Regression coefficients for statistical models 1–3.
ln(negative
mood) × 1000
β (SE)
Model 1
Model 2
Model 3
β10 intercept: estimated value at 2>h/>pm on a non-binge day
β11 difference between binge and non-binge days at 2 pm
β12 linear trend at 2 pm on a non-binge day
β13 quadratic trend on a non-binge day
β14 difference in linear trend at 2 pm between binge and
non-binge days
β15 difference in quadratic trend between binge and
non-binge days
905 (104)
223 (49.8)
− 0.1 (4.40)
− 0.28 (0.88)
7.12 (6.85)
0.22 (1.19)
ln(positive
mood) × 1000
β (SE)
t
8.74⁎⁎⁎
4.48⁎⁎⁎
tension × 1000
t
22.0⁎⁎⁎
− 2.48⁎
− 0.02
− 0.36
1.04
6045 (275)
− 422 (170)
17.1 (15.1)
− 3.59 (3.00)
− 24.5 (23.4)
1.14
− 1.19
− 1.05
0.18
− 10.3 (4.05)
− 2.53⁎
13.1⁎⁎⁎
5.19⁎⁎⁎
4579 (355)
− 2319 (710)
445 (102)
4.36⁎⁎⁎
80.5 (20.5)
t
1073 (103)
57.3 (52.9)
− 2.64 (4.67)
− 2.09 (0.93)
5.32 (7.27)
10.7⁎⁎⁎
1.08
− 0.56
− 2.25⁎
0.46
1.19 (1.26)
0.95
12.9⁎⁎⁎
− 3.26⁎⁎
1251 (119)
651 (182)
10.5⁎⁎⁎
3.59⁎⁎⁎
− 920 (396)
− 2.32⁎
316 (101)
3.12⁎⁎
3.92⁎⁎⁎
− 143 (79.5)
− 1.79
57.6 (20.3)
2.83⁎⁎
6.20 (1.71)
3.64⁎⁎⁎
− 9.41 (6.61)
− 1.42
4.43 (1.69)
2.62⁎⁎
β25 quintic trend during pre-binge phase immediately before first daily binge
β26 linear trend during post-binge phase
β30 intercept: estimated value at first daily binge
β31 difference between estimated values 30 min before and 30 min
after first daily binge
0.17 (0.05)
− 55.0 (16.3)
785 (114)
− 533 (137)
3.38⁎⁎⁎
− 6.86⁎⁎⁎
6.86⁎⁎⁎
− 3.88⁎⁎⁎
− 0.22 (0.19)
173 (62.8)
6472 (401)
1103 (512)
− 1.13
2.76**
16.2⁎⁎⁎
2.15⁎
β32 linear trend during pre-binge phase
β33 linear trend during post-binge phase
− 26.0 (13.5)
− 47.1 (22.1)
− 1.93
− 2.14⁎
β20 intercept: estimated value at first daily binge
β21 linear trend during pre-binge phase immediately before
first daily binge
β22 quadratic trend during pre-binge phase immediately before
first daily binge
β23 cubic trend during pre-binge phase immediately before first
daily binge
β24 quartic trend during pre-binge phase immediately before first
daily binge
1379 (105)
950 (183)
β (SE)
103 (50.5)
50.1 (82.2)
⁎ p b 0.05.
⁎⁎ p b 0.01.
⁎⁎⁎ p b 0.001.
showed a significant curvilinear decrease before the first binge
episode, with strongest rates of decrease shortly before the first
binge, followed by a linear increase during the post-binge phase,
which was also significant (solid lines in Fig. 1b). For tension there
was a significant curvilinear increase before the first binge episode,
which was also most pronounced shortly before the first binge (solid
lines in Fig. 1c). The post-binge trend for tension was significantly
negative.
3.2.3. Model 3
When the values up to 30 min before and 30 min after the first
binge were omitted, a different pattern was observed. Values for
negative mood and tension now decreased and positive mood
increased during the pre-binge phase, these trends being significant
for positive mood and failing to reach significance for negative mood
(Fig. 1a–c, broken lines). Trends during the post-binge phase, in
contrast, were similar to those in Model 2 for all three mood factors.
Thus negative mood and tension both decreased and positive mood
increased, these trends being significant for negative mood only. Note
that for each mood factor predicted values 30 min after the first daily
binge were significantly higher (negative mood and tension) or lower
(positive mood) than those 30 min before it.
3.2.4. Model 4
The trait-specific factor comorbidity status moderated the temporal course of tension prior to the first daily binge (not shown in table):
patients suffering from comorbid mental disorders had higher rates of
increase for tension immediately before the first daily binge than
patients without comorbid disorder. Also, patients with higher
depressiveness had lower rates of increase for tension immediately
before the first daily binge than patients with lower depressiveness.
The other person-specific characteristics, baseline BMI, years since
first manifestation of a binge episode, and EDE total score did not
moderate the course of negative or positive affect and tension before
and after the first daily binge.
2.04⁎
0.61
0.12 (0.05)
− 38.3 (16.2)
867 (124)
− 308 (136)
2.44⁎
− 2.37⁎
6.97⁎⁎⁎
− 2.26⁎
− 22.1 (13.4)
− 25.3 (22.0)
− 1.65
− 1.15
122
S. Munsch et al. / Psychiatry Research 195 (2012) 118–124
4. Discussion
The present study is to our knowledge the first to investigate daily
courses of mood and tension experienced during binge and non-binge
days and before and after binge eating, thereby covering an extended
time span in the natural environment of treatment-seeking women
with BED.
In general the study findings corroborate findings from studies on
BN and BED showing that negative mood ratings were higher and
positive mood ratings lower on binge days compared to non-binge
days (Smyth et al., 2007; Stein et al., 2007).
Considering binge days and temporal courses until the first daily
binge, we found that positive mood, negative mood and tension all
strongly deteriorated immediately before the first daily binge (see
Model 2), as has been observed in BN (Engelberg et al., 2007; Smyth
et al., 2007). It must be noted that in general and even during binge
eating values for mood factors, especially regarding negative mood
and tension, varied between 2.5 and 4 on a range of 1 to 10, which is
rather low (Fig. 1). Our analyses further revealed that the temporal
course of mood and tension was independent of eating disorder
severity or body weight. However, individuals suffering from
additional mental disorders were prone to higher increases in tension
shortly before the first daily binge than individuals without comorbid
disorders. Also more depressed individuals experienced a lower
short-term increase of tension before the first daily binge compared to
less depressed individuals.
Following the considerations of Smyth and colleagues, we
excluded the values covering the time span 30 min before and
30 min after the first binge as these measures could be influenced by
the affect-laden event of recent binge eating per se (Smyth et al.,
2007). In a BN sample, Smyth and colleagues found that even after
excluding these measures, accumulation of mood deterioration
remained a robust predictor of binge eating. In contrast, in our
sample of female BED individuals, excluding measures over the 1-h
interval resulted in a strikingly different pattern. We even observed a
slight improvement of mood up to 30 min before binge eating (Model
S. Munsch et al. / Psychiatry Research 195 (2012) 118–124
123
Fig. 1. Daily course of negative mood, positive mood, and tension before and after the first binge episode. Values for negative mood and tension were backtransformed from lntransformation. Solid lines denote predicted values from linear mixed models during binge days and refer to statistical Model 2. Broken lines denote predicted values when disregarding
values at the time of the binge (±30 min) and refer to statistical Model 3. Note that predicted values during non-binge days are not included. Grey lines denote means and 95% confidencelimits of observed values and were obtained by computing means and confidence limits of all observed values within defined time intervals. Intervals relative to the time variate centered at
the first daily binge were: –6 h to –4 h/–4 h to –2 h/–2 h to b 0 h/time at first daily binge/N 0 h to + 2 h/+ 2 h to + 4 h/+ 4 h to + 6 h.
3) followed by an abrupt and significant deterioration (Model 2)
immediately before the binge. These findings seem to contradict affect
regulation theory as hypothesized in BN, where binge eating is
supposed to be the result of an accumulation of negative affect. In
contrast, our results indicate that binge eating in BED might rather be
the result of an immediate breakdown of emotion and impulse
regulation caused by sudden increases of negative affect and tension,
and a rapid decrease of positive affect. Our results are more in line
with the assumption of the escape theory (Heatherton and Baumeister, 1991) in which a short decrease in self-awareness is thought to
inhibit cognitive control and thus might contribute to triggering binge
eating. They are also consistent with Wegner's theory of ironic effects
of inhibitory mental control processes, resulting in a sudden shift
toward suppressed undesired behavior (Wegner, 1994). Further,
these findings underline the importance of the concepts of affect
lability and impulsivity, characterized by a trait-like tendency to
experience rapidly shifting affective states as risk factors for binge
eating in BED and BN (Svaldi et al., 2009; Anestis et al., 2010).
Regarding the long-term course of binge eating, our findings
indicate that after a mood deterioration immediately before a binge
episode a rather slow but lasting improvement over several hours
following the binge emerged (Fig. 1). Compared to the short-term
relief of distress after binge eating in BN due to both an increase of
positive and a decrease of negative mood, in BED relief of aversive
mood states after bingeing seems to be less pronounced and reveals
itself only if longer time frames are considered (Smyth et al., 2007).
124
S. Munsch et al. / Psychiatry Research 195 (2012) 118–124
This finding does not seem to be astonishing when compared with
binge cycles in BN, as these are normally finished by purging behavior
leading to immediate, even though short-term, relief. As in BED
suffering might decrease only gradually, this might explain why
previous studies focussing on the immediate effect of binge eating on
mood in BED did not indicate an improvement of mood as a function
of a binge episode (Hilbert et al., 2004; Munsch et al., 2009). To
investigate whether the slow improvements of negative and positive
mood after binge eating have reinforcing properties as in BN and
whether they contribute to the maintenance of binge eating in BED,
more frequent assessment time points after binge eating as well as
accompanying cognitions should be considered. Generally, reinforcement is considered more potent with closer time contingeny. Future
research should also focus on the investigation of the underlying
biological mechanisms such as physiological stress levels to further
investigate the different mechanisms in binge cycles between BED
and BN.
Possible criticisms include the lack of representativeness of our
study sample as it consisted of individuals fulfilling criteria to
participate in a randomized treatment trial. As only very few men
participated, we subsequently had to exclude them from our analyses.
Further, the underpowered sample size limits the possibility to detect
moderator effects of mood factors and the sampling time of 1 week
before treatment begin was rather short. Another limitation is that we
only registered objective binge eating episodes even though there are
now considerable data indicating that the only difference between
individuals suffering from objective compared to subjective binge
eating is with respect to increased body weight for objective binge
eaters (Mond et al., 2010). We further cannot exclude that
participants did not report all occurrences of binge eating, even
though we did not find any indications for a lack of compliance to the
EMA procedure. Participants rated EMA to be an acceptable and
feasible method in their responses to our exit questionnaire. They
further estimated that the 1-week assessment period was representative and that they did not feel that their binge eating patterns were
influenced by EMA (Munsch et al., 2009). Nevertheless, even selfreported EMA remains a retrospective assessment method and might
itself be subject to memory and reporting bias in terms of, for
example, mood-dependent recall. Future research could profit from
more fine-grained and simultaneous diurnal analyses of the emotional and cognitive characteristics and of shape and weight concern
before and after binge eating using new methods such as automatic
sound sampling, which provides observational data with short
sampling intervals but nevertheless low subject burden (Mehl et al.,
2001; Hilbert et al., 2009).
Overall our findings indicate that binge eating in BED might
represent the result of an immediate break-down of emotion and
impulse regulation attempts. After binge eating, in contrast to findings
from BN, we found a less pronounced and only slow recovery of mood
after binge eating in BED. With respect to therapeutic implications of
this result, we ought to develop stimulus control strategies to increase
alertness of considered individuals in order to prevent or detect first
signs of upcoming urges to binge as especially these individuals will
have pronounced difficulties to inhibit binge eating once it has
started. Often applied training of response prevention in order to
suppress unwanted behavior during states of high mental load may in
contrast further enhance ironic effects of suppression attempts and so
increase the probability of problematic behavior (Wegner, 2009).
Response-prevention strategies, such as the acceptance of stressful
events or the disclosure of mental states, may then be options to be
considered in further research and clinical practice.
Appendix A. Supplementary data
Supplementary data to this article can be found online at doi:10.
1016/j.psychres.2011.07.016.
References