Assignment Two: Screening for maternal syphilis
advertisement

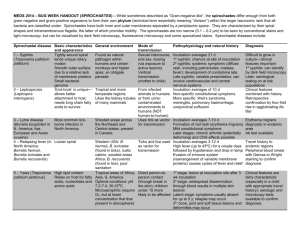
TM5541 Managing Effective Health Programmes Assignment Two: Screening for maternal syphilis Plan of an early detection activity Samantha Leggett SN 12494652 Word Count: 3342 (excluding in-text references, tables and footnotes) 9/30/2011 SN: 12494652 Samantha Leggett Contents 1. The early detection activity 3 2. 2.1 The problem screened for 3-4 2.2 The screening test used 4-7 3. Evidence justifying why the activity would be beneficial to the population 7-9 4. 4.1 The process required to establish an antenatal maternal syphilis screening programme 10-12 4.2 Running an antenatal maternal syphilis screening programme 12-13 5. Promoting a maternal syphilis screening programme to expectant mothers 14-15 6. Summary 15-16 7. Appendix A: Congenital syphilis- signs, symptoms and sequelae 17-21 8. References 22-26 2 SN: 12494652 Samantha Leggett TM5541 Managing Effective Health Programmes Assignment Two: Plan of an early detection activity 1: The early detection activity: Maternal syphilis screening as an integral component of antenatal care across Papua New Guinea 2.1: The problem screened for: Maternal and potential congenital syphilis infection Syphilis infection is a significant public health problem and remains a major infectious but preventable determinant of maternal, neonatal, infant and child morbidity and mortality in resource poor settings (Peeling & Ye, 2004; Rydzak & Goldie, 2008). Globally, each year around 12 million people are infected with syphilis; 2 million of these are pregnant women and 90% of all annual syphilis cases are in low income countries (Tucker et al. 2010). Untreated infection in a woman can lead to serious cardiovascular and neurological complications and can facilitate HIV transmission1 (Levin et al. 2007; Rydzak & Goldie, 2008). If a pregnant woman has syphilis she may transmit the infection to the foetus transplacentally at any point during the pregnancy causing congenital syphilis (see Appendix A). Additionally maternal syphilis also has the potential to lead to other adverse pregnancy outcomes such as still birth or spontaneous abortion and low birth weight babies. (Bronzan et al. 2007; Levin et al. 2007; World Health Organization [WHO], 2009). It is thought that between 49-67% of pregnant women with active syphilis will have adverse 1 Syphilis causes genital sores and these make it easier to transmit and acquire HIV infection. It is estimated that if syphilis is present an individual is at 2-5 times higher risk of acquiring HIV via sexual exposure. Ulcerative sexually transmitted infections that cause sores, ulcers or breaks in the skin or mucous membranes (such as syphilis) disrupt the bodies’ natural defence barriers that provide protection against infection. Genital ulcers caused by syphilis can bleed easily and when they come into contact with mucosa during sex increase the infectiousness of and susceptibility to HIV (Centers for Disease Control and Prevention. (2010). Sexually transmitted Diseases: Syphilis. Retrieved from: http://www.cdc.gov/std/syphilis/STDFact-Syphilis.htm). 3 SN: 12494652 Samantha Leggett pregnancy outcomes (Bronzan et al. 2007); the earlier in pregnancy the transmission, the worse the expected outcome if the maternal syphilis is left untreated (WHO, 2005). The exact burden of congenital syphilis is not truly known due to inadequate surveillance and reporting (WHO, 2009). Additionally only 68% of women in developing countries receive ante natal care (ANC) and of these, around half do not attend until after the first trimester-many pregnancies affected by syphilis end in miscarriage in the first or second trimester before women are screened for syphilis (Romoren &Rahman, 2006; WHO, 2005). However at least half a million infants are known to be born annually with congenital syphilis and maternal syphilis results in a further half million known stillbirths and miscarriages per year (WHO, 2007). Perinatal morbidity and mortality attributed to syphilis infection is on par with that of HIV, tetanus and malaria which all receive greater global public health attention (Schmid, 2004; WHO, 2008; WHO, 2009). Foetal mortality and infant and childhood morbidity and mortality due to congenital syphilis are preventable if infected mothers are identified and treated appropriately by the middle of the second trimester. Routine antenatal screening and treatment to prevent congenital syphilis has thus become the main focus of syphilis control programmes (Peeling & Ye 2004; WHO, 2004). 2.2: The screening test used Rapid point-of care testing using an onsite treponemal immunochromatographic strip test. The selection of diagnostic tools used in such programmes must take into consideration the health and economic outcomes of variables such as: adverse pregnancy outcomes (miscarriage, low-birth-weight, still birth, neonatal death, congenital syphilis); maternal life expectancy; life time health costs for both mothers and their children; life expectancy gains for children; and the availability and feasibility of resources. 4 SN: 12494652 Samantha Leggett Serological tests are cited as the method of choice for prenatal screening and are asserted to be feasible and affordable in most resource limited countries; non-treponemal tests such as Rapid Plasma Reagin (RPR) are sensitive and simple to perform but have not historically been readily available in primary health care settings as cold storage is required for reagins and electricity is needed to operate a rotator. In general, non-treponemal tests can be prone to providing pregnant women with false positive results (as much as 28%) and ideally in this situation results would be confirmed in a laboratory using for example a venereal disease research laboratory (VDRL) test. However, it is acknowledged that in resource poor settings this is technologically and logistically unlikely (Peeling & Ye, 2004). Another important drawback of using a two-step diagnostic method is the potential of loss of patients to follow-up due to women having to return to the clinic for test results and potential treatment. Loss to follow up represents a waste of resources, adverse clinical outcomes due to a delay in early treatment or no treatment at all and continued transmission of infection (Munkhuu, Liabsuetrakul, Chongsuvivatwong, McNeil, & Janchiv, 2009; WHO, 2006). Stoner (2008) asserts that the new generation rapid point-of-care treponemal test (immunochromatographic strip (ICS) test) offers an opportunity for the immediate detection and treatment of infected pregnant women without the drawbacks of the other two methods. These tests are simpler to use, interpretation does not rely on subjectivity and they do not require electricity/refrigeration or additional equipment. A number of researchers, in comparisons of RPR, VDRL and ICS tests have found the ICS test, used in a one stop screen-and-treat strategy was: more effective in the prevention of congenital syphilis; resulted in increased screening coverage; improved the rate of case detection in women and their partners; was more cost-effective; and had the added benefit of ease of use even in the most rudimentary conditions (Levin et al. 2007; Munkhuu et al. 2009; Peeling & Ye. 2004; Rydzak & Goldie, 2008; Watson-Jones et al. 2005). Comparisons between these tests are presented in table 1. 5 SN: 12494652 Samantha Leggett Table 1. Comparison of suitable diagnostic tests for maternal and congenital syphilis screening in resource poor settings Criteria RPR VDRL ICS Rapid Test (non-treponemal) (non-treponemal) (treponemal) Sensitivity 86-100% 78-100% 84-98% Specificity 93-98% 98% 94-98% Ease of use Easy Easy Easy Where used Exam room/on-site Exam room/on-site Exam room/on-site lab lab lab Rotator/refrigerator Light microscope None Training Needed Minimal Minimal Minimal Average Cost US$0.50 US$0.50 US$0.55-3.00 Comments Most RPR agents Reagents require Most tests are stable require refrigeration refrigeration at room temperature Cannot be used on Cannot be used on for >6 months whole blood-serum whole blood-serum Test doesn’t only only distinguish between Test results Test results active infections and interpreted interpreted previously treated subjectively-margin subjectively-margin infections for reporting error for reporting error Uses whole blood Extra Equipment Needed (Bronzan et al. 2007; Peeling & Ye, 2004; WHO, 2006) Stoner (2008) points out that the ICS tests also have some performance limitations: the treponemal antibody is present for many years and because of this treponemal tests are unable to distinguish between active syphilis infection and a previously treated infection. So, despite having had prior and adequate treatment for syphilis, a previously positive but cured woman will have persistently positive ICS tests and without laboratory confirmation 6 SN: 12494652 Samantha Leggett will always receive treatment for syphilis. The treponemal test also only presents a positive or negative result and is also therefore unsuitable for monitoring therapy responses. In resource constrained settings, facilities for immediate testing and treatment and the subsequent reduction of losses to follow-up provide considerable advantages, since the benefits of preventing serious sequelae and onward transmission of syphilis clearly outweigh the risks and costs of over treatment (Benzaken et al. 2011; Bronzan et al. 2007; Peeling & Ye, 2004). Rydzak and Goldie (2008) argue that unnecessary treatment increases costs and the probability of treatment side effects in addition to potentially contributing to antimicrobial resistance. However they point out that the net impact of overtreatment is expected to be marginal relative to the magnitude of the benefits. 3: Evidence justifying why the activity would be beneficial to the population of Papua New Guinea To date, Papua New Guinea’s (PNG) performance towards achieving the Millennium Development Goals (MDGs) has been variable, with progress made in some areas and stagnation or even reversal in others. The WHO (2010) believe this to be due to a combination of factors: restricted institutional frameworks; severe resource limitations (both material and human); and many socioeconomic, cultural and political constraints. Table 2 presents some important comparisons in local health related statistics. Table 2: Western Pacific health statistics Papua New Infant Neonatal Still births per At least one mortality per mortality per 1000 total antenatal care 1000 live 1000 live births visit births births 52 26 15 79% Guinea 7 SN: 12494652 Samantha Leggett Vanuatu 30 15 15 84% Fiji 15 9 13 100% Australia 4 3 3 98% WHO (2011) The successful implementation of a programme to eliminate congenital syphilis would significantly contribute to PNG’s progress towards three key health related MDGs: MDG 4: reduce child mortality –mortality rates in children under five will be reduced as a result of a decreased incidence of low-birth-weight babies, perinatal death and congenital infection. Additionally mother to child transmission of HIV should be reduced. MDG 5: improve maternal health-maternal health will be improved as a result of fewer spontaneous abortions, and a lowered incidence of syphilis and its sequelae including the increased risks of contracting HIV. MDG 6: combat HIV/AIDS, malaria and other diseases-screening and treatment for syphilis in women will help to prevent the spread of HIV (WHO 2005a; WHO, 2008) The WHO (2010) report that in PNG the syphilis prevalence rate amongst antenatal care attendees is 5.78%. Of the seventy seven countries reporting antenatal care attendance, only five had a higher prevalence of syphilis amongst attendees than PNG: Central African Republic (5.88%); Ghana (6.91%); Mozambique (6.93%); Chad (7.3%); and Madagascar (7.7%). Frank and Duke (2000) found a syphilis prevalence of 7.1% in a small rural Highlands centre and in the same study congenital syphilis accounted for 22% of all neonatal deaths over a two year period; the major risk factor for death in affected babies was low-birth-weight. Duke et al. (2002) point out that in the same setting potentially avoidable factors accounted for 50% of childhood mortality and a lack of maternal syphilis screening was cited amongst these variables as were a lack of antenatal care and a failure of disease screening programmes. 8 SN: 12494652 Samantha Leggett Syphilis surveillance was endorsed by the PNG Ministry of Health in 2006 and initiated in 2008. As a component of the five year HIV and syphilis surveillance plan, routine antenatal syphilis screening is recommended for all pregnant women although the literature is unclear regarding testing methodology (HIV & AIDS Data Hub, 2011). UNICEF (2011) purports that syphilis screening is routinely conducted for all antenatal care attendees in PNG however it would be wise to remain mindful of previous warnings of poor surveillance and reporting, antenatal care attendance figures, topographical challenges, access constraints and known resource constraints. The WHO (2007) point out that policy guidelines are building blocks only and Hawkes, Miller, Reichenbach, Nayyar and Buse (2004) warn that policy doesn’t automatically translate into an effective health programme. A considerable challenge that faces the delivery of health care services in PNG is that 86% of the country’s population live in rural areas and access to these widely scattered communities is often difficult, slow and expensive. Only 3% of roads are paved and many villages can only be reached on foot or via river transportation. The nations’ capital Port Moresby is not linked by road with the rest of the country. (WHO, 2010). These constraints also make it difficult and costly for the population to access the services that are available (AusAID, 2009). Section 2.2 discusses the general benefits of a same day screen-and-treat syphilis detection programme. In addition to this and relevant to the PNG context, the choice to use ICS tests over other options is important in PNG if aiming to scale up syphilis screening programmes in distant settings of high maternal syphilis prevalence and with the lowest levels of health care service delivery. Regions for example characterised by the need for river transportation, a lack of well equipped laboratories, a lack of electricity and refrigeration facilities, inadequate staff training and a poor continuity of supplies (Benzaken et al. 2011). These characteristics are typical of much of PNG. 9 SN: 12494652 Samantha Leggett 4: The process required to establish and run an antenatal syphilis screening programme 4.1 Establishing a screening programme would utilise the following steps: 1. Planning: The literature highlights the utmost importance of comprehensive planning as the first step in implementing a screening programme in resource limited countries. The inclusion of the national Ministry of Health (MoH), programme decision makers and managers, health care staff and importantly, representatives of the women and their male sexual partners who are to be offered screening is imperative. In doing this a culturally appropriate intervention responsive to needs can be crafted using a partnership approach. Additionally barriers to and opportunities for turning health policy into effective practice can be identified. Hawkes et al. (2004) assert that political support is vital for getting issues such as congenital syphilis onto the health policy agenda and for helping to ensure that programmes are implemented in a sustainable way. Planning should include: a review of the evidence on disease prevalence and associated sequelae; any previous cost-effectiveness analyses in the local setting; lobbying for the cause, addressing sustainability issues (e.g. funding and capacity), addressing procurement and supply issues and strengthening existing systems; how partner notification is best to be addressed; how an integrated approach is best achieved (i.e. linking screening to another more politically successful issue e.g. prevention of mother-to-child transmission of HIV (PMTCT-HIV); identifying areas of responsibility and ownership; and planning for any trial sites. 2. Training: The second stage should be comprehensive training for health personnel to include: correct use and interpretation of the chosen ICS test; a comprehensive understanding of maternal and neonatal syphilis and the importance of incorporating early screening into ANC programmes; pre- and post-test counselling skills; and documentation skills. The WHO (2007) advocate training traditional birth attendants and traditional healers to refer women to appropriate antenatal health 10 SN: 12494652 Samantha Leggett services. It is thought that this may be an important method of increasing early attendance for antenatal care since many women consult these caregivers first. Further, training of lay community health workers to deliver promotion of early ANC is also advocated (Howlett, Larsh, Dobi & Mai, 2009; Tanjasiri, Sablan-Santos, Merrill, Quitugua & Kuratani (2008). 3. Information, education and communication (IEC)2 activities should be planned. A high visibility campaign is essential in a country such as PNG where much news travels by word of mouth via the ‘wantok system’3. Pasick, Hiatt and Paskett (2004) also stress the centrality of the church as a source of education and social support. The influence of church leaders on individual’s beliefs and practices is thought to offer great potential for positive health related behaviour change. Social networks such as this can help women to not only initiate behaviours but also maintain them over time (Byles, Sanson-Fisher & Redman, 1996; Tanjasiri et al. 2008). In terms of the number and diversity of potential screening participants reached, information aimed at communities has been found to achieve the widest scope (Pasick et al. 2004). MoH endorsement of all activities promoted must be explicit. 4. MoH endorsed manuals and technical guidelines on syphilis testing during antenatal care must be developed and made available to all relevant health personnel. 2 IEC activities should include the design of a national informational and media campaign to encourage women to seek antenatal care services early in pregnancy, to promote the benefits of early antenatal care and syphilis testing, the plan for the rollout of the new programme. The campaign must be highly visible and could include themed posters, leaflets to be given out in key locations such as markets, radio adverts, television adverts, newspaper adverts and reports and may also employ the use of mobile telephone technology (UNFPA. (1999). Reproductive Health in Refugee Situations. Appendix One: Information, Education and Communication (IEC) Programmes. Retrieved from: http://www.unfpa.org/emergencies/manual/a1.htm) 3 The “wantok” (lit. one talk) system is PNG’s safety net, under which the extended family and clan members are obligated to support each other. It also functions as an informal country-wide news network (UNDP. (2004). Millennium Development Goals, Progress Report for Papua New Guinea. Retrieved from: http://www.undp.org.pg/documents/mdgs/National_MDG_Progress_Report_2004.pdf) 11 SN: 12494652 Samantha Leggett 5. Procurement, importation and stocking of ICS tests and other supplies. 6. Roll out of screening programme (Garcia et al. 2007; Gloyd et al. 2007; Hawkes et al. 2004; Howlett et al. 2009; WHO, 2006; WHO, 2007) 4.2 Running a screening programme should follow the proceeding steps: Ideally all pregnant women will be screened at least once as early in antenatal care as possible integral to routine and existing antenatal/HIV-PMTCT programmes. The test and treatment will be free. Group IEC activities should be carried out in the antenatal clinic each morning by health care staff. The woman will receive pre-test counselling. If informed consent is given blood will be obtained from a finger prick for rapid ICS testing for syphilis (+/- HIV testing). The woman will receive her result and post-test counselling. If the result is positive she will receive the appropriate treatment on the same day as the test4. The woman will receive a notification card to give to her male sexual partner asking them to attend the clinic. It is advised that the reason for visiting the clinic is not explicitly stated on the card, but wording such as ‘there are issues regarding the pregnancy that we wish to discuss with you’. It is thought that messages focusing on the health of the unborn child will have a more positive effect and that this will 4 If penicillin allergy is not a known issue treatment is with intramuscular Benzathine Penicillin. It is inexpensive (median cost US$0.25 per treatment), on the WHO essential drugs list and resistance is not known to be a widespread problem. (World Health Organization. (2005). Eliminating Congenital Syphilis. Retrieved from: http://www.who.int/reproductivehealth/publications/rtis/eliminating_congenital_syphilis.pdf). 12 SN: 12494652 Samantha Leggett promote a higher male sexual partner attendance rate at the clinic where maternal and congenital syphilis can be discussed with them and they can receive free presumptive treatment should they choose (Gichangi, Fonck, Sekande-Kigondu & Ndinya-Achola, 2000; WHO, 2007). The woman will also receive counselling regarding intimate partner violence (IPV) risks. The health care professional will clearly and concisely document all aspects of the consultation including counselling given, screening, treatment and partner notification in the woman’s health record and clinic health records. Ongoing supervision, training and audit procedures should include: evaluating test use and interpretation; stock management; staff rostering and cover (Kamb et al. (2010) assert that an especially difficult barrier to surmount in many settings is ensuring adequate human resources-not only in numbers (recruiting and retaining) but in currency of training and practical experience); record keeping; quality control (QC)5; and partner tracing activities. (Garcia et al. 2007; Gloyd et al. 2007; Maggwa, Askew, Mugwe, Hagembe & Homan, 2001; WHO, 2006; WHO, 2007) NB Ideally all women should be screened in their first trimester and again in the third trimester to account for later primary infection and the possibility of re-infection, particularly if partners aren’t treated. Optimally a third test would be performed on the woman at delivery. As a minimum, one test should be performed at the first antenatal visit and if this doesn’t happen, then at or soon after delivery (Saloojee et al. 2004). 5 QC of the validity of the rapid tests is advocated as most manufacturers recommend that the rapid test kits are transported and stored at 4-30 degrees Celsius. It is acknowledged that temperatures above 30 degrees Celsius may sometimes be unavoidable, as in many remote locations where rapid tests are intended to be used. QC should be carried out in a central laboratory (World Health Organization. (2006). The use of rapid syphilis tests. Retrieved from: http://whqlibdoc.who.int/hq/2006/TDR_SDI_06.1_eng.pdf). 13 SN: 12494652 Samantha Leggett 5: Promoting a maternal syphilis screening programme to expectant mothers In general, common barriers to participation in screening activities include: 1) lack of awareness and understanding of the importance of screening; 2) not knowing the required screening frequency; 3) not knowing how to access screening; 4) emotional barriers (fear of the test, fear of finding disease, embarrassment, previous negative experiences); and 5) cognitive barriers (lack of knowledge, not understanding concept of prevention) (Howlett et al. 2009). Promoting a screening activity to a potential client should therefore aim to address these barriers. Ideally, as previously stated, before the antenatal clinic commences each morning and afternoon the women waiting will be part of a group IEC activity run by the health care staff. Information should include: the importance of early ANC and syphilis testing in pregnancy; complications of untreated syphilis to the mother and unborn child and children who are born with congenital syphilis; HIV-PMTCT; voluntary counselling and testing and the promotion of condom use in pregnancy. Face to face information delivered by health care workers plus visual media has been shown to be the most effective strategy for increasing the uptake of screening (Byles et al. 1996). The one-to-one dialogue between the healthcare provider and the client would then proceed as follows: The information related to maternal and congenital syphilis from the IEC session would be re-iterated, emphasizing both the health and economic benefits to the woman and her family of the early treatment and detection of maternal syphilis. Meissner et al. (2004) emphasize that health care workers play a pivotal role in facilitating screening uptake and highlight that messages communicating the advantages of early screening must use clear language. Efforts should be made to address individual barriers to early screening uptake face-to-face; counselling provides the perfect opportunity for this (Tanjasiri et al. 2008). Since syphilis is often asymptomatic (WHO, 2007) and therefore cannot necessarily be seen, it is important to stress the normalcy of lack of symptoms in syphilis infection and the simplicity of testing and treatment (Tanjasiri et al. 2008). That both screening and 14 SN: 12494652 Samantha Leggett treatment is rapid, on-site and free would also be emphasized-a number of studies have shown that the lower the response cost to the client, the greater the likelihood of screening uptake (Byles et al. 1996; Meissner et al. 2004). At this point the client would also receive counselling regarding the event of a positive result and the need for partner notification and treatment to gain optimal results. IPV screening would take place and counselling given regarding the best ways to inform partners when IPV is feared. Gichangi et al. (2000) state that women who inform their spouse of an STI often face increased violence, divorce or loss of security. Programmes involving partner notification should weight the benefits and risks for the woman involved. Edwards et al. (2005) stress that adequate discussion about the risks and benefits associated with different choices that could be made is required if client involvement is to be secured through informed decision making. 6: Summary In summary, maternal and congenital syphilis are a significant public health concern and untreated, cause a high burden of morbidity and mortality, particularly in resource poor settings. Early screening and treatment for maternal syphilis as an integral component of antenatal care has been shown to be an effective method of combating this somewhat neglected burden of disease. The use of new generation rapid point-of-care ICS tests provides a simple and cost-effective method for the immediate detection and treatment of syphilis without the drawbacks of other methods which is particularly relevant to the Papua New Guinea context. Evidence demonstrates that a comprehensively and inclusively planned screening programme that is well run and consistently evaluated has the ability to significantly raise the profile of a disease, dramatically increase screening coverage and subsequently considerably reduce the burden of disease. Screening programmes such as this can assist resource poor countries such as PNG improve maternal and child morbidity and mortality 15 SN: 12494652 Samantha Leggett and can thus act as an aid to making real progress toward the achievement of the Millennium Development Goals. 16 SN: 12494652 Samantha Leggett 7: Appendix A Congenital Syphilis- signs, symptoms and sequelae Congenital syphilis is caused by the bacterium Treponema pallidum which spreads from a pregnant mother who is infected with syphilis to her unborn child via the placenta. T. pallidum can also be contracted via the birth canal. Nearly half of all children infected with syphilis while they are in utero will die before or shortly after birth. For the rest congenital syphilis can be a severely disabling condition. It is possible for a baby to be born without signs and symptoms of the disease but, if left untreated, the baby may develop serious problems within a few weeks. Signs and symptoms in the newborn: Failure to thrive Irritability Fever Early rash (small blisters on the palms of the hands and soles of the feet) Later rash (a copper coloured maculopapular rash esp. on the extremities) 17 SN: 12494652 Samantha Leggett (Peihong, J., Zhiyong, L., Rengui, C., & Jian, W. (2001). Early congenital syphilis. International Journal of Dermatology, 40(3), 198-202). Rash of the mouth genitalia and anus Watery discharge from the nose (Congenital syphilis in a newborn. Retrieved from: http://menshealth.about.com/cs/stds/l/blsyph_photo2.htm) Hepatosplenomegaly Lymphadenopathy 18 SN: 12494652 Samantha Leggett Signs, symptoms and sequelae in older infants and young children: Abnormal notched and peg-shaped teeth (http://www.duke.edu/~ema5/Golian/Slides/1) Clouding of the cornea (Syphilis: congenital interstitial keratitis. Retrieved from: http://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/syphilis-congenitalinterstitial-keratitis.html). Blindness Poor hearing/deafness Gray, mucous-like patches on the anus and outer vagina Scarring of the skin around the mouth, genitalia and anus Joint swelling Bone pain ‘Saber shins’-a malformation of the tibia 19 SN: 12494652 Samantha Leggett (http://www.rightdiagnosis.com/phil/html/syphilis/2387.htm)l Saddle nose deformity (http://www.duke.edu/~ema5/Golian/Slides/6/InfDis-Bacteria7.html) (http://medphoto.wellcome.ac.uk/) Neurological sequelae including seizures and developmental delay 20 SN: 12494652 Samantha Leggett Taken from: PubMed Health. (2009). Congenital Syphilis. Retrieved from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002320/ And British Association for Sexual Health and HIV (BASHH). (2008). UK National Guidelines on the Management of Syphilis 2008. Retrieved from: http://www.bashh.org/guidelines 21 SN: 12494652 Samantha Leggett 8: References AusAID. (2009). Working Paper 1: Papua New Guinea Country Report. Evaluation of Australian aid to health service delivery in Papua New Guinea, Solomon Islands and Vanuatu. Retrieved from:http://www.ode.ausaid.gov.au/publications/documents/ working-paper-health-service-delivery-png.pdf Benzanken, A.S., Sabido, M., Galban, E., Pedroza, V., Araujo, A.J.G., Peeling, R.W., & Mabey, D. (2011). Field performance of a rapid point-of-care diagnostic test for antenatal syphilis screening in the Amazon region, Brazil. International Journal of STD and AIDS, 22, 15-18. Bronzan R.N., Mwesigwa-Kayongo, D.C., Narkunas, D., Schmid, G.P., Neilsen, G.A., Ballard, R.C., Karuhije, P., Ddamba, J., Nombekela, E., Hoyi, G., Dlali, P., Makwedini, N., Fehler, H.G., Blandford, J.M., &Ryan, C. (2007). Onsite rapid antenatal syphilis screening with an immunochromatographic strip improves case detection and treatment in rural South African clinics. Sexually Transmitted Diseases, 34(7), S55-S60. Byles, J.E., Sanson-Fisher, R.W., & Redman, S. (1996). Promoting screening for cervical cancer: realising the potential for recruitment by general practitioners. Health Promotion International, 11(4), 299-308. Edwards, A.G.K., Evans, R., Dundon, J., Haigh, S., Hood, K., & Elwyn, G.J. (2005). Personalised risk communication for informed decision making about taking screening tests. Retrieved from: http://onlinelibrary.wiley.com.elibrary.jcu.edu.au/doi/10.1002 /14651858.CD001865.pub2/abstract Frank, D., & Duke, T., (2000). Congenital syphilis at Goroka Base Hospital: incidence, clinical features and risk factors for mortality. Papua New Guinea Medical Journal, 43(1-2), 121-126. Garcia, S.G., Tinajeros, F., Revello, R., Yam, E.A., Richmond, K., Diaz-Olavarrieta, C., & Grossman, D. (2007). Demonstrating public health at work: A demonstration project 22 SN: 12494652 Samantha Leggett of congenital syphilis prevention efforts in Bolivia. Sexually Transmitted Diseases, 34(7), S37-S41. Gichangi, P., Fonck, K., Sekande-Kigondu, C., & Ndinya-Achola, J. (2000). Partner notification of pregnant women infected with syphilis in Nairobi, Kenya. International Journal of STD and AIDS, 11(4), 257-261. Gloyd, S., Montoya, P., Floriano, F., Chadreque, M.C., Pfeiffer, J., & Gimbel-Sherr, K. (2007). Scaling up antenatal syphilis screening in Mozambique: Transforming policy into action. Sexually Transmitted Diseases, 34(7), S31-S36. Hawkes, S., Miller, S., Reichenbach, L., Nayyar, A., & Buse, K. (2004). Antenatal syphilis control: people, programmes, policies and politics. Bulletin of the World Health Organization, 82, 417-423. HIV and AIDS Data Hub. (2011). Papua New Guinea country factsheet. Retrieved from: http://aidsdatahub.org/dmdocuments/png_country_factsheet_20_may_2011_with_f unding_revised_12_July_2011.pdf Howlett, R.I., Larsh, S., Dobi, L., & Mai, V. (2009). Promoting cancer screening among Ontario Chinese women. Canadian Journal of Public Health, 100(4), 315-319. Kamb, M., Newman, L.M., Riley, P.L., Mark, J., Hawkes, S.J., Malik, T., & Broutet, N. (2010). A road map for the global elimination of congenital syphilis. Obstetrics and Gynecology International. doi: 10.1155/2010/312798 Levin, C.E., Steele, M., Atherly, D., Garcia, S.G., Tinajeros, F., Revollo, R., Richmond, K., DiazOlavarrieta, C., Martin, T., Floriano, F., Massango, I., & Gloyd, S. (2007). Analysis of the operational costs of using rapid syphilis tests for the detection of maternal syphilis in Bolivia and Mozambique. Sexually Transmitted Diseases, 34(7), S47-S54. 23 SN: 12494652 Samantha Leggett Maggwa, B.N., Askew, I., Mugwe, E., Hagembe, B., & Homan, R. (2001). A case study of Nairobi City Council’s decentralised syphilis screening programme in antenatal clinics. Retrieved from: http://www.popcouncil.org/pdfs/frontiers/reports /kenyasyphrpt.pdf Meissner, H.I., Smith, R.A., Rimer, B.K., Wilson, K.M., Rakowski, W., Vernon, S.W., & Briss, P.A. (2004). Promoting cancer screening: Learning from experience. Cancer, 101(S5), 1107-1117. Munkhuu, B., Liabsuetrakul, T., Chongsuvivatwong, V., McNeil, E., & Janchiv, R. (2009). Onestop service for antenatal syphilis screening and prevention of congenital syphilis in Ulaanbaatar, Mongolia: A cluster randomized trial. Sexually Transmitted Diseases, 36(11), 714-720. Pasick, R.J., Hiatt, R.A., & Paskett, E.D. (2004). Lessons learned from community-based cancer screening intervention research. Cancer, 101(S5), 1146-1164. Peeling, R.W., & Ye, H. (2004). Diagnostic tools for preventing and managing maternal and congenital syphilis. Bulletin of the World Health Organization, 82, 439-446. Romoren, M., & Rahman, M. (2006). Syphilis screening in the antenatal care: a crosssectional study from Botswana. BMC International Health and Human Rights, 6, 8. Retrieved from: http://www.biomedcentral.com/1472-698X/6/8 Rydzak, C.E., and Goldie, S.J. (2008). Cost-effectiveness of rapid point-of-care prenatal syphilis screening in Sub-Saharan Africa. Sexually Transmitted Diseases, 35(9), 775784. Saloojee, H., Velaphi, S., Goga, Y., Afadapa, N., Steen, R., & Lincetto, O. (2004). The prevention and management of congenital syphilis: an overview and recommendations. Bulletin of the World Health Organization, 82, 424-430. Schmid, G. (2004). Economic and programmatic aspects of congenital syphilis prevention. Bulletin of the World Health Organization, 82, 402-409. 24 SN: 12494652 Samantha Leggett Stonor, B.P. (2008). Rapid tests for maternal syphilis screening: Effective and cost-effective. Sexually Transmitted Diseases, 35(9), 785-786. Tanjasiri, S.P., Sablan-Santos, L., Merrill, V., Quitugua, L., & Kuratani, D. (2008). Promoting breast cancer screening among Chamorro women in Southern California. Journal of Cancer Education, 23(10), 10-17. Tucker, J.D., Bu, J., Brown, L.B., Yin, Y.P., Xiang. S., & Cohen, M.S. (2010). Accelerating worldwide syphilis screening through rapid testing: a systematic review. Lancet Infectious Diseases, 10, 381-386. UNICEF. (2011). Elimination of new paediatric HIV infections and congenital syphilis in AsiaPacific, 2011-2015: Conceptual framework and monitoring and evaluation guide. Retrieved from: http://www.unicef.org/eapro/PPTCT_CF_and_ME_guide _17Aug11.pdf Watson-Jones, D., Oliff, M., Terris-Prestholt, F., Changalucha, J., Gumodoka, B., Mayaud, P., Semakafu, A.M., Kumaranayake, L., Gavyole, A., Mabey, D., & Hayes, R. (2005). Antenatal syphilis screening in sub-Saharan Africa: lessons learned from Tanzania. Tropical Medicine and International Health, 10(9), 934-943. World Health Organization. (2004). Guidelines for the management of sexually transmitted infections. Retrieved from: http://www.who.int/hiv/pub/sti/pub6/en/ World Health Organization. (2005). Eliminating Congenital Syphilis. Retrieved from: http://www.who.int/reproductivehealth/publications/rtis/eliminating_congenital_ syphilis.pdf World Health Organization. (2006). The use of rapid syphilis tests. Retrieved from: http://whqlibdoc.who.int/hq/2006/TDR_SDI_06.1_eng.pdf 25 SN: 12494652 Samantha Leggett World health Organization. (2007). The global elimination of congenital syphilis: Rationale and strategy for action. Retrieved from: http://www.who.int/reproductivehealth /publications/rtis/9789241595858/en/index.html World Health Organization. (2008). Report of the workshop for the global fund proposal writing in maternal and newborn health service delivery area. SEARO, New Delhi, 1922 August 2008.Retrieved from: http://www.searo.who.int/LinkFiles /Making_Pregnancy_Safer_SEA-MCH-252.pdf World Health Organization. (2009). Regional strategy for the elimination of congenital syphilis. Retrieved from: http://www.searo.who.int/LinkFiles/Publications_RSelimination-syphilis.pdf World Health Organization. (2010). Towards universal access: Scaling up priority HIV/AIDS interventions in the health sector. Progress Report 2010. Retrieved from: http://www.who.int/hiv/pub/2010progressreport/report/en/index.html World Health Organization. (2011). Global health Observatory Data Repository Country Statistics. Retrieved from: http://apps.who.int/ghodata /?vid=15600&theme=country 26