Cases and Instructions
advertisement

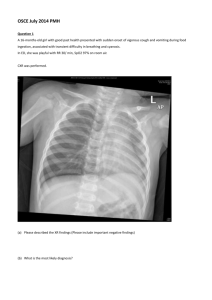
The Frugal Diagnostician Facilitator Instructions: Divide the group into 2-4 teams. Provide each team with identical patient. Each team discusses the case and can order a round of tests each “day”, during up to 3 “days” of hospitalization. For each test the team orders on a particular day, the facilitator will provide the team with the charge for each test and test result. This information is to be shared prior to decision-making and orders for the “next hospital day”. Each day of hospitalization also incurs a room charge. If a team feels they have reached a diagnosis prior to day 3, they may discharge the patient to prevent additional hospital charges. The goal is to correctly diagnose the patient in the most cost efficient manner. Thus, the team that arrived at the diagnosis with the lowest bill (by adding up their charges) wins. Charges should be obtained from the chargemaster of the trainee’s hospital. The Frugal Diagnostician #1 Your task is to correctly diagnose the patient in the most cost effective manner. Please read the history and physical below. Then, make a list of laboratory/imaging tests you would like to order. The test results will be given to you along with a charge for one night in the hospital. At that point, you can submit a diagnosis and discharge your patient, or keep them in the hospital another night and order more testing. After 3 nights in the hospital, the patient must be discharged and a diagnosis submitted. Upon discharge, your patient’s total bill will be calculated. The team that correctly diagnoses the patient with the lowest bill, will be crowned the frugal diagnostician. History of Present Illness: 52 year old man presents to the Emergency Department with chest pain and shortness of breath. Symptoms have been present for approximately 1 hour. The pain was described to be in the middle of his chest, and was acute in onset. Shortness of breath is worse with exertion, and he also notes a new cough. Past Medical History: Hypertension Obese Low back pain Family History: Mother – Systemic Lupus Erythematous Father – Diabetes Mellitus II Physical Exam: T 98.4 BP 156/87 P 84 R22 O2 91% Gen: WD, WN, WM HEENT: PERRL, EOMI Chest: CTA B CV: RRR No MRGs Abd: BS+, soft, NT, ND EXT: NO C/C/E DP2+ Neuro: CN II-XII intact, strength 5/5, DTRs NL Social History: 1ppd smoker x 30 years Occasional alcohol use No illicit drug use Monogamous with wife of 25 years Employed as a truck driver Medications: Hydrochlorothiazide 25 mg daily For Facilitator Use Only: Case #1: Diagnosis: Pulmonary Embolism Cardiac Enzymes: CK, CK-MB normal. Troponin 0.1 All labs and tests are “within the normal range” except: Electrocardiogram – sinus tachycardia D-Dimer – 500 ng/mL Lipid Profile – Total Cholesterol 200, LDL 170, HDL 25, Triglycerides 180 Lower Extremity Ultrasound – thrombus seen in the right femoral vein V/Q scan – high probability CT Chest with contrast – nonocclusive pulmonary embolus in the right pulmonary artery The Frugal Diagnostician Case #2 Your task is to correctly diagnose the patient in the most cost effective manner. Please read the history and physical below. Then, make a list of laboratory/imaging tests you would like to order. The test results will be given to you along with a charge for one night in the hospital. At that point, you can submit a diagnosis and discharge your patient, or keep them in the hospital another night and order more testing. After 3 nights in the hospital, the patient must be discharged and a diagnosis submitted. Upon discharge, your patient’s total bill will be calculated. The team that correctly diagnoses the patient with the lowest bill will be crowned the frugal diagnostician. History of Present Illness: A 58 year old woman presents to the emergency room with lower extremity edema. Over the past 3-4 weeks she's noticed an abrupt increase in lower extremity edema and abdominal swelling. She's also noticed weight gain although she is unable to quantify exactly how much weight she gained. Over the same time period, she has noticed a decrease in urine output. She denies any current dyspnea on exertion or shortness of breath at rest. She denies any fatigue, or bleeding. She really states that overall she feels very well without fatigue, tiredness, abdominal pain, nausea, vomiting or any other significant problems other than her swelling in her abdomen and her legs. Past Medical History: Hypertension Medications: Micardis/HCTZ Aspirin 81mg daily Social History: She is married and works as a teacher at a preschool. She states that she drinks socially approximately one to 2 drinks 2 times per week and has no history of heavy alcohol intake. She smokes approximately 5-6 cigarettes per day and has a 20-pack-year history of smoking. She denies any history of illicit drug use. Family History: Her father died from heart disease in his late 60s. Her mother had diabetes mellitus and died in her 60s Physical Exam: Temp 98.5 HR 88 RR20 BP 105/72 Oxygen 96% Gen:African American female in no acute distress. Eyes: EOMI, PERRL Nose, Mouth, Throat: moist oral mucosa, no erythema, no lesions, no nasal deformities Respiratory: Clear to auscultation bilaterally Cardiacvascular: regular rate and rhythm, no murmurs, rubs or gallops GI: BS+, soft, NT, distended abdomen with shifting dullness Ext: No clubbing, cyanosis, DP 2+, 2+ pitting edema to thighs bilaterally Neuro: No focal neuro deficits, normal gait, MAEW Psych: Pleasant, appropriate, normal affect Skin: No prominent rashes, no tattoos US Abdomen: Conclusion: 1. Enlarged, diffusely heterogeneous liver with innumerable solid lesions throughout both lobes. These are highly suspicious for hepatocellular carcinoma. 2. Reversed flow demonstrated within the main and right portal veins, suggestive of portal hypertension. 3. Large ascites. CT Triple Phase Abdomen Impression: 1. Innumerable hepatic masses which show enhancement characteristics compatible with diffuse multifocal hepatocellular carcinoma. Probable tumor thrombus within the right portal vein and multiple branches. 2. Hepatic artery-portal venous shunt, likely related to intratumoral shunt from the dominant right hepatic lobe mass. 3. Findings of cirrhosis and portal hypertension with large volume of ascites. MRI Abdomen: 1. Multifocal hepatic masses likely hepatocellular carcinoma. 2. Cirrhosis and portal venous hypertension. Diagnosis: Cirrhosis (from Hepatitis C with Hepatocellular Carcinoma) The Frugal Diagnostician Case #3 Your task is to correctly diagnose the patient in the most cost effective manner. Please read the history and physical below. Then, make a list of laboratory/imaging tests you would like to order. The test results will be given to you along with a charge for one night in the hospital. At that point, you can submit a diagnosis and discharge your patient, or keep them in the hospital another night and order more testing. After 3 nights in the hospital, the patient must be discharged and a diagnosis submitted. Upon discharge, your patient’s total bill will be calculated. The team that correctly diagnoses the patient with the lowest bill, will be crowned the frugal diagnostician. History of Present Illness A 29 year old white man presents to the emergency room with a 2 week history of abdominal pain, nausea/vomiting, and hematuria. He first noticed red urine on his first void of the day 2 weeks ago. He had run several miles the day prior. On subsequent voids, the redness faded and resolved, but he then noticed fatigue. Then, one week ago he developed epigastric abdominal pain, lower back pain, nausea, subjective fever/chills, and dark urine. He presented to an outside physician and was diagnosed with a urinary tract infection. He was treated with ceftriaxone and ciprofloxacin but his symptoms persisted so he presented the ER. He has no history of similar symptoms. Past Medical History: Allergic Rhinitis Past Surgical History: None Allergies: NKDA Medications: Fexofenadine Ciprofloxacin Social History: He works as a private pilot. No recent sexual activity. No tobacco, alcohol, or illicit drug use. Family History: Both parents and all siblings are alive and healthy Physical Exam: T 98.4 BP 156/87 P 84 R16 O2 100% Wt: 170lbs Gen: WD, WN, WM in NAD HEENT: PERRL, EOMI, mild scleral icterus Neck: No LAD or TM Chest: CTA B CV: RRR No MRGs Abd: BS+, soft, NT, ND EXT: NO C/C/E DP2+ Neuro: CN II-XII intact, strength 5/5, DTRs NL The Frugal Diagnostician Case #3 Preceptor Laboratory/Imaging Results: 133 / 99 / 34 -------------------155 3.4 / 20 / 7.9 5.2 3.4 \-------/ 91 22.4 Ca:8.7 mcv:100 lipase: 83 CT Abd/Pelvis: No adenopathy PT:11 PTT:25.3 Lactate: 1.3 Spleen is upper limits of normal TP 7.8 AST 102 Alk phos: 72 Otherwise normal CT abdomen Alb 4.4 ALT 37 T bili 1.9 CT Chest: normal D bili: 0.3 Urinalysis: CK: 233 Spec grav: 1.030 LDH: 2642 Protein: 2+ Retic: 5.92% Glu: 1+ ESR: 61 Blood:3+ Haptoglobin <1 Nitrate and LE: neg B12, Folate, iron studies: WBC: 3-5 normal RBC: 0-2 All other tests not listed here are “normal” RBCs positive for CD59 consistent with: Paroxysmal Nocturnal Hemoglobinuria (PNH) The Frugal Diagnostician Test Ordered Result Charge